Article Text

Abstract
Objectives With early and intensive treatment many patients with early RA attain remission. Aims were to investigate (1) the frequency and time to sustained remission and subsequent tapering in patients initially treated with conventional synthetic disease modifying anti-rheumatic drug ((cs)DMARD) strategies and (2) the frequency and time to flare and regained remission in patients tapering csDMARDs and biological (b)DMARDs during 2 years of follow-up.
Methods Two-year follow-up data from the treatment in the Rotterdam Early Arthritis Cohort (tREACH) cohort were used. Patients were randomised to initial treatment with triple DMARD therapy (iTDT) with glucocorticoid (GC) bridging or methotrexate monotherapy (iMM) with GC bridging. Patients were evaluated every 3 months. In case Disease Activity Score (DAS) was >2.4 treatment was switched to a TNF-blocker. In case DAS<1.6 at 2 consecutive time points, tapering was initiated according to protocol. Outcomes were rates of sustained remission (DAS<1.6 at 2 consecutive time points), flare (medication increase after tapering) and remission after flare (DAS<1.6). Data were analysed using Kaplan-Meier analyses.
Results During 2 years of follow-up, sustained remission was achieved at least once by 159 (57%) of patients, of whom 118 and 23 patients initiated tapering of csDMARDs and bDMARDs, respectively. Thirty-four patients achieved drug-free remission. Flare rates were 41% and 37% and within 1 year, respectively. After flare, 65% of patients tapering csDMARDs re-achieved remission within 6 months after treatment intensification.
Conclusions Regardless of initial treatment strategy, 57% of patients achieved sustained remission during 2 years of follow-up. Flare rates were 41% and 37% within 12 months in patients tapering csDMARDs and bDMARDs, respectively.
Trial registration number ISRCTN26791028; Post-results.
- Early Rheumatoid Arthritis
- DMARDs (synthetic)
- DMARDs (biologic)
- Disease Activity
- Treatment
Statistics from Altmetric.com
Introduction
Several studies,1–3 among which the treatment in the Rotterdam Early Arthritis Cohort (tREACH) study,1 have shown that by early and intensive treatment remission can be achieved in many patients with early RA. Current evidence suggests that once remission has been achieved, treatment de-escalation may be considered,4 ,5 but most recent studies have focused on de-escalation of biological disease modifying anti-rheumatic drugs ((b)DMARDs) only.4
In this follow-up study of tREACH,1 we investigated the frequency and time to remission and subsequent tapering of conventional synthetic (cs)DMARDs and bDMARDs and the frequency and time to flare and regained remission in patients tapering csDMARDs and bDMARDs.
Methods
Data were used from the tREACH cohort, a detailed description of the inclusion criteria and protocol can be found in the original tREACH paper.1 In short, patients with early arthritis (duration of complaints <1 year) and a high risk of developing persistent arthritis (score >6 points on Visser model)6 were eligible. Of included patients, 97% fulfilled the American College of Rheumatology/European League Against Rheumatism 2010 criteria for RA.1 ,7 Patients were randomised for induction treatment strategies with triple DMARD therapy (iTDT); methotrexate (MTX) 25 mg/week, sulfasalazine 2000 mg/day and hydroxychloroquine 400 mg/day or MTX monotherapy 25 mg/week (iMM). Both groups received bridging therapy with glucocorticoids (triamcinolone acetonide 80 mg or methylprednisolone 120 mg once by intramuscular injection or oral prednisone 15 mg for 4 weeks, thereafter tapered by 5 mg/week). For this analysis, the two groups receiving iTDT with oral or intramuscular glucocorticoids were combined (n=184). Patients were evaluated every 3 months and treated in a treat-to-target fashion. If Disease Activity Score (DAS) was >2.4 on initial treatment, patients were switched to a TNF-blocker combined with MTX 25 mg/week. If sustained remission (DAS<1.6 at 2 consecutive visits) was achieved, medication was tapered according to protocol (expert opinion of project group) while remission remained1: iTDT: sulfasalazine stop, half-dose MTX, quarter-dose MTX, stop MTX, stop hydroxychloroquine; iMM: half-dose MTX, quarter-dose MTX, stop MTX; Combination of MTX and TNF-blocker: randomisation to taper MTX first (aforementioned regimen) or TNF-blocker first: doubling of interval, then half dose, then stop. In case MTX or TNF-blocker had been completely tapered, the remaining agent was tapered according to the aforementioned scheme (also see online supplementary file 2). Flare was defined as an increase in medication after initiation of tapering. Initially, duration of follow-up was 12 months, which was soon extended to ≥24 months after the trial had started. For this reason 76 (27%) of patients missed one or more visits during the second year of follow-up. Groups were compared using simple descriptive statistics. Sustained low disease activity (LDA) was defined as DAS<2.4 at 2 consecutive visits. Drug-free remission was defined as DAS<1.6 without using DMARDs. Rates of sustained remission, flares and time to regain remission between groups were analysed using Kaplan-Meier analyses. Baseline predictors for drug-free remission were evaluated using logistic regression. Statistical analyses were performed using STATA V.14.1 (StataCorp, 4905 Lakeway Drive College Station, Texas, USA). p Values <0.05 were considered statistically significant.
Supplemental material
Supplemental material
Results
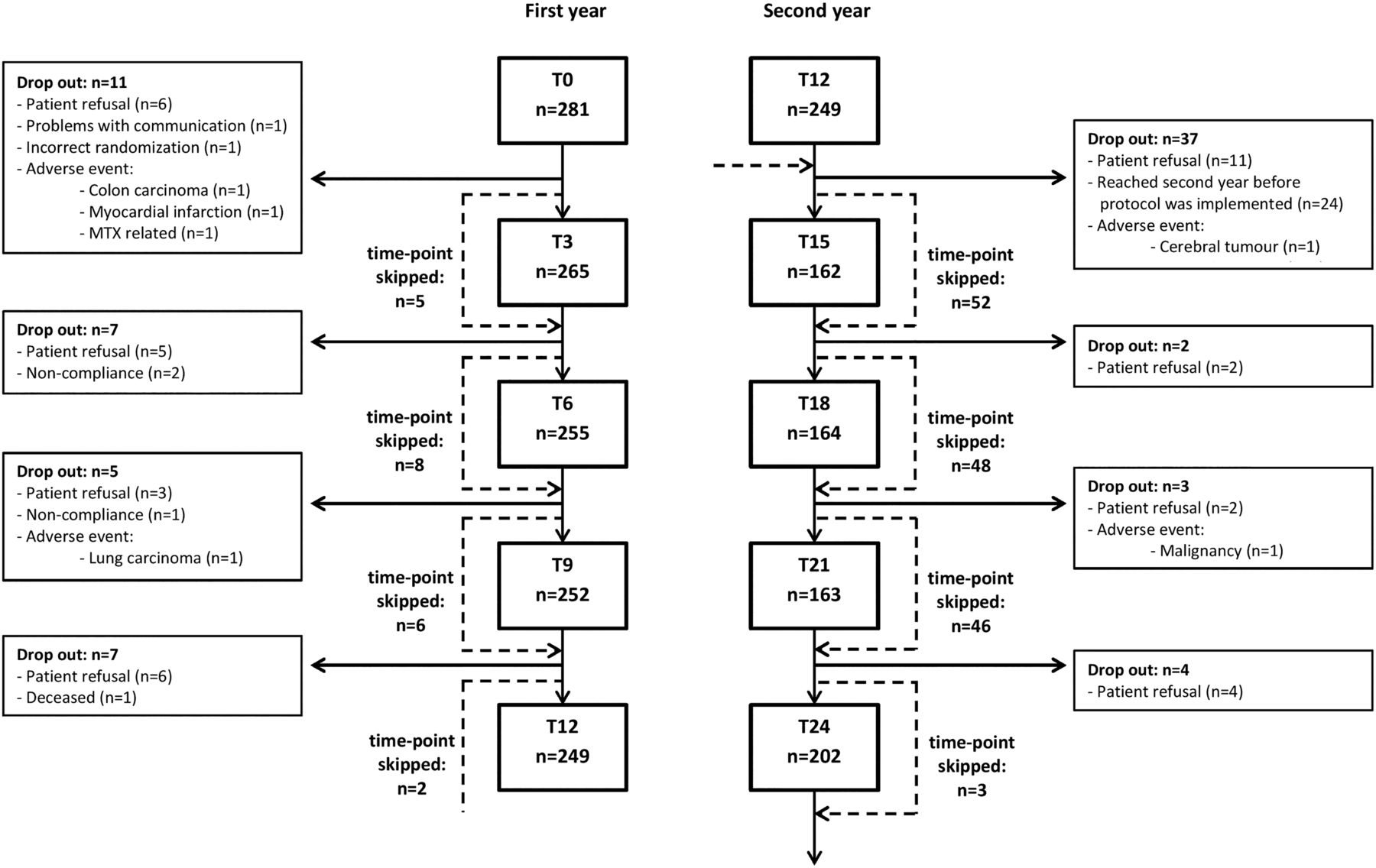
Data from 281 patients participating in tREACH were available for analysis. Overall, 68% of patients were female and mean age was 53.2 years. Mean baseline DAS was 3.36 (95% CI 3.24 to 3.47). At baseline, groups were similar with respect to demographic-related and disease-related characteristics (table 1). A flowchart of follow-up is shown in figure 1. During 2 years of follow-up, sustained remission was achieved in the iTDT and iMM groups in 108 (59%) and 51 (53%) of patients and sustained LDA in 148 (80%) and 76 (78%) of patients, respectively. Remission was achieved with a biological in 12 (11%) and 13 (26%) patients in the iTDT and iMM groups, respectively. After sustained remission had been achieved, 94 (87%) and 47 (92%) initiated tapering in the iTDT and iMM groups, respectively. Tapering involved a conventional DMARD in 84% (n=118) of the cases and a biological DMARD in 16% (n=23) of the cases.
Baseline characteristics of all patients initiating with csDMARD therapy and the subset of patients tapering DMARDs (synthetic and/or biological)
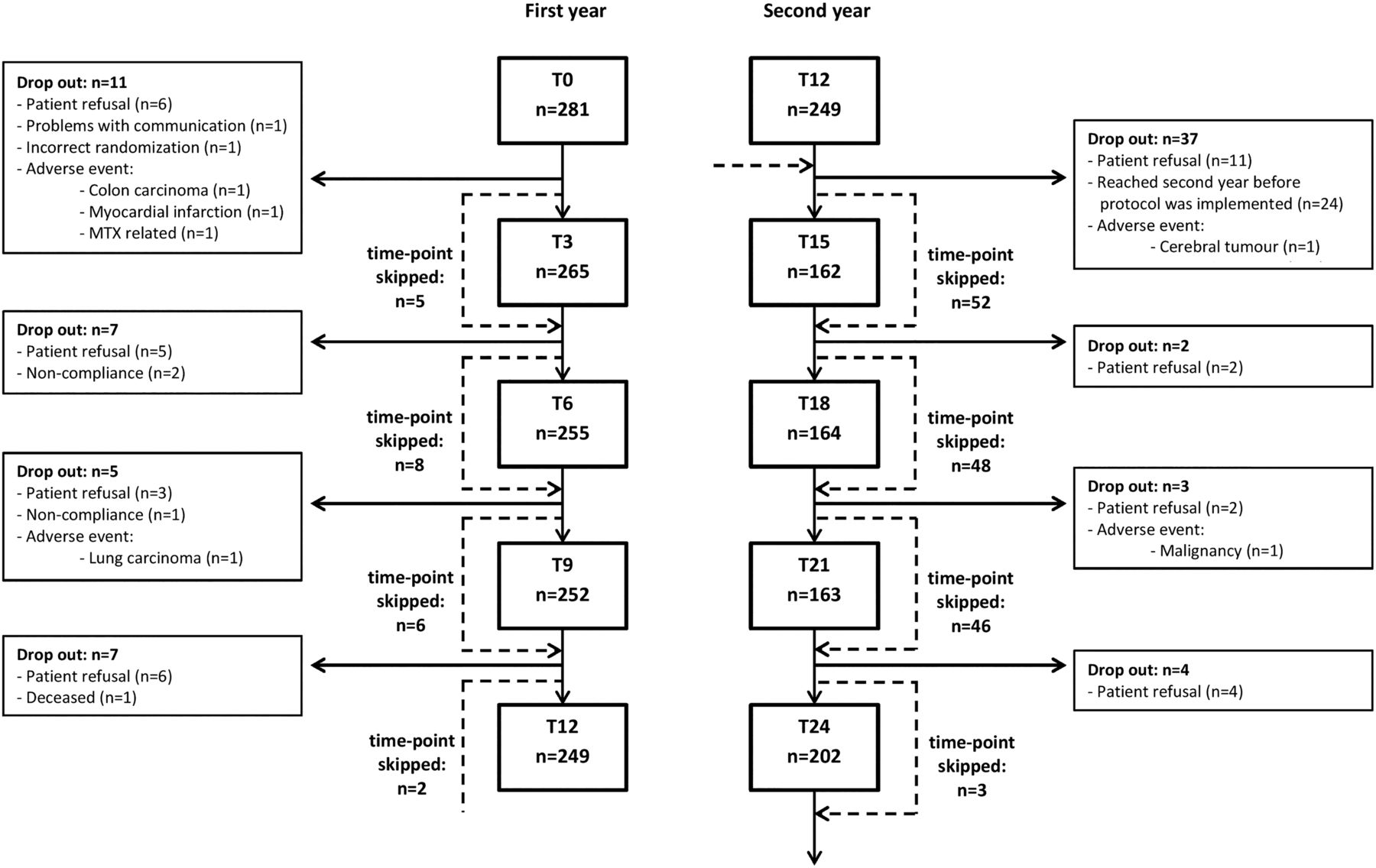
Flow-chart of follow-up.
Time to remission
Of patients achieving sustained remission, 56 (52%) and 19 (37%) achieved this within 6 months (p=0.09) and 91 (84%) and 39 (76%) within 1 year (p=0.27) in the iTDT and iMM groups, respectively. Therefore, a trend for higher frequency of sustained remission and subsequent tapering was observed in the iTDT group compared with the iMM group, but this trend became less prominent over time (figure 2A). Kaplan-Meier analysis over 2 years also revealed no significant difference between groups (figure 2A).

{kind=link}
{kind=link}
Survival analysis of patients initiating with triple DMARD therapy (iTDT, blue line) versus patients initiating with methotrexate (MTX) monotherapy (iMM, red line) with respect to sustained remission (A), of patients achieving early remission (light blue line) versus late remission (orange line) with respect to occurrence of flare (C), of patients tapering csDMARDs (green line) or bDMARDs (+csDMARDs) (purple line) with respect to occurrence of flare (C), and time to regain remission after flare of patients tapering csDMARDs (green line) or bDMARDs (+csDMARDs) (purple line) (D).
Remission duration
Sustained remission at ≥3 consecutive visits was achieved by 123 patients (3 visits: n=27, 4: n=40, 5: n=22, 6: n=11, 7: n=7, 8: n=16). After tapering DMARDs 34 patients achieved drug-free remission, of whom 11 and 7 remained in drug-free remission for at least 3 and 6 months, respectively. Nine and seven patients failed drug-free remission or were censored after 3 months, respectively. Baseline predictors male sex, lower DAS and Health Assessment Questionnaire (HAQ) and not having paid work were associated with achieving drug-free remission (see online supplementary file 1).
Flare
For all 141 patients tapering any DMARD, no difference in flare rate was observed for patients achieving remission early (≤6 months) or thereafter (figure 2B). Of 118 patients tapering csDMARDs, 52 (44%) experienced a flare during the 2-year follow-up period. Kaplan-Meier analysis revealed a flare rate of 41% (95% CI 32% to 50%) within 1 year and 51% (95% CI 42% to 62%) within 18 months after initiation of tapering (figure 2C). Of 23 patients tapering bDMARDs, 7 (30%) experienced a flare during 2 years of follow-up. Kaplan-Meier analysis revealed a flare rate of 37% (95% CI 19% to 64%) within 1 year after initiation of tapering (figure 2C). Upon medication increase after a flare, Kaplan-Meier analysis revealed that 53% (95% CI 40% to 68%) of patients tapering csDMARDs regained DAS-remission within 3 months and 65% (95% CI 50% to 79%) within 6 months (figure 2D). Of five patients tapering bDMARDs, three regained DAS-remission within 6 months after flare.
Discussion
In this study of early RA, a trend for a higher frequency of achieving sustained remission, with less use of biologicals, was observed in patients with initial triple DMARD therapy compared with initial MTX monotherapy. We found that 57% of patients reached sustained remission and 80% sustained LDA at least once during 2 years of follow-up. This is in line with findings by others. Previous studies found sustained remission rates of 50% during 2 years of follow-up in patients initiating with MTX monotherapy8 and an LDA rate of 78% at 2 years of follow-up in patients with early RA initiating with combination csDMARD therapy with tapered high dose prednisone.9 Although in recent years, many clinical trials and observational studies on tapering DMARDs have emerged,4 most deal with the de-escalation of biological DMARDs4 ,10–12 or report mixed results for groups in which both bDMARDs and csDMARDs were tapered.13 ,14 A recent publication on data from a Dutch registry study found that de-escalation of MTX in patients using concomitant TNFi did not influence average DAS and drug survival.15 However, studies that specifically focus on de-escalation of conventional DMARDs generally date from the nineties or before and were performed in patients with established RA.4 Results from this study on the tapering of conventional DMARDS may therefore provide additional value to current literature. The 1-year flare rates after tapering csDMARDS (41% (95% CI 32% to 50%)) and bDMARDS (37% (95% CI 19% to 64%)) appear to be comparable to the pooled flare rate found for studies de-escalating TNF-blockers of 33% (95% CI 23% to 45%).4 Also in line with the findings of the systematic review, we found that the majority of patients (65% (95% CI 50% to 79%)) regained a state of remission within 6 months after treatment intensification.
This study has several strengths and limitations. Strong points of this study include the fact that we performed an analysis in a large clinical trial population of patients with early RA treated in a treat-to-target fashion. Some limitations in the analysis should be noted as well. First of all, follow-up with respect to the outcome measures used in this analysis was not complete. Especially, during the second year of follow-up we had a substantial amount of missing observations. This had to do with the fact that initially the trial was set up to have a follow-up duration of 12 months. The follow-up was soon extended to 36 months after the trial had started. Hence, part of the patients has only been followed for 1 year. This problem was addressed by using Kaplan-Meier estimates, which allowed to correctly analyse censored data. The tapering of medication was performed largely according to protocol; however, this protocol was not always exactly followed by the rheumatologists in practice. Reasons may vary from unfamiliarity with the protocol to deviation on purpose because the disease status as indicated by the DAS did not agree with the rheumatologists' opinion. Although this may be seen as a limitation, it may also be a strong point as our results are likely to better reflect the way in which tapering is performed in clinical practice. Another potential limitation is that the flare rates in this study may depend on the tapering scheme used. We used stepwise tapering as long as sustained remission was maintained. It is possible that more patients would have remained in sustained remission if only dose reduction of csDMARDs were applied, which has already been shown for TNF-inhibitors.16 ,17 Considering the DMARDs patients received at the moment flare occurred (see online supplementary file 2), we observe that 15/32 of patients that had a flare while tapering combination DMARD therapy experienced the flare during the first two steps (tapering sulfasalazine and MTX, arguably cutting dose in half) and 6/15 patients when tapering MTX to half dose. Possibly, dose reduction is more difficult to achieve in patients receiving csDMARDs only than in patients treated with bDMARDs. It should be noted that after flare, the majority of patients regained remission within 6 months which is similar to re-remission rates observed in studies de-escalating biological DMARDs.4 At last it should be noted that data are from an early RA population with relatively mild disease. Results may not be generalisable to populations with established RA for which rates of remission and successful tapering may be lower.
In conclusion, we found a trend for earlier achievement of sustained remission, with less use of biologicals, in patients with early RA initiating with triple DMARD therapy compared with MTX monotherapy. Regardless of initial treatment strategy, 57% of patients achieved sustained remission during 2 years of follow-up. Of patients tapering csDMARDs, 41% experienced a disease flare within 12 months. After flare, 65% of patients tapering csDMARDs regained a state of remission within 6 months after treatment intensification.
Acknowledgments
We thank all patients, rheumatologists and research assistants from the following rheumatology centres for making this study possible: Erasmus MC, Rotterdam; Maasstad Ziekenhuis, Rotterdam; Sint Franciscus Gasthuis, Rotterdam; Vlietland Ziekenhuis, Schiedam; Admiraal de Ruyter Ziekenhuis, Goes and Vlissingen; ZorgSaam Ziekenhuis, Terneuzen.
References
Footnotes
Handling editor Tore K Kvien
Contributors All authors meet the criteria for authorship as stated in the ICMJE recommendations.
Funding This work was supported by an unrestrictive grant from Pfizer B.V. [0881-102217]. Pfizer had no involvement in the study design; in collection, analysis and interpretation of data; writing of the report, and decision to submit for publication. The corresponding author had full access to all data and had final responsibility for the decision to submit for publication. Data management was sponsored by the Dutch Arthritis Foundation.
Competing interests None declared.
Ethics approval Medical ethics committee of the Erasmus Medical Center, Rotterdam.
Provenance and peer review Not commissioned; externally peer reviewed.