Article Text

Abstract
Objectives To investigate the association between infection or respiratory tract disease and future risk of developing idiopathic inflammatory myopathy (IIM).
Methods A case–control study was performed using Swedish nationwide registers. Adults with newly diagnosed IIM were identified (2002–2011) from the National Patient Register (NPR) and the Swedish Rheumatology Register (n=957). Controls were matched by age, sex and place of residence (n=9476). Outpatient visits and hospitalisations preceding IIM diagnosis indicating infection or respiratory disease were identified from NPR. Conditional logistic regression models were used to calculate OR and 95% CI. Sensitivity analyses were performed by varying the exposure definition, adjusting for previous healthcare consumption and excluding individuals with connective tissue disease, IIM lung phenotype or IIM-associated cancer.
Results Preceding infections were more common in IIM cases compared with controls (13% vs 9%) and were associated with an increased risk of IIM (OR 1.5, 95% CI 1.2 to 1.9). Gastrointestinal and respiratory tract infections were associated with an increased risk of IIM while cutaneous infections were not.
Preceding respiratory tract disease was present in 10% of IIM cases and 4% of controls (OR 2.3, 95% CI 1.8 to 3.0). Both upper and lower respiratory tract diseases were associated with an increased risk of IIM.
Variations in exposure and outcome definitions did not greatly affect the results.
Conclusions Infections and respiratory tract diseases are associated with an increased risk of IIM which suggests that the triggering of the immune system may take place outside the skeletal muscle.
- epidemiology
- dermatomyositis
- polymyositis
- infections
Statistics from Altmetric.com
Introduction
Idiopathic inflammatory myopathies (IIM) are a heterogeneous group of rare autoimmune disorders characterised by weakness and inflammation in skeletal muscles. Based on clinical and muscle biopsy findings, IIM is often divided into three clinical subtypes, polymyositis (PM), dermatomyositis (DM) and inclusion body myositis (IBM).1
IIM is believed to be caused by an interaction between environmental and genetic risk factors. The HLA-DRB1*0301 gene has been identified as the strongest genetic risk factor.2 Few environmental risk factors have been identified, although ultraviolet light and vitamin D have been discussed.3 4 Infections could trigger autoimmunity through multiple mechanisms including molecular mimicry5 and epitope spreading6 and have been implicated in the development of other rheumatic diseases such as rheumatoid arthritis (RA).7 8 For IIM, there are case reports and case series showing an increased frequency of infections preceding IIM but population-based studies investigating infection as a risk factor for IIM are lacking.9 10
Because the lung is a common extra-muscular manifestation in IIM and many patients display lung involvement at diagnosis,11 it is of special interest in IIM aetiology. Infectious initiation of inflammation is one suggested mechanism of autoimmunity but the location of the inflammation could be key. A possible site of autoimmunity initiation is the lung’s mucosal tissue, which is the first line of defence against some exposures such as infection and smoking.12 Evidence has accumulated that smoking is a triggering factor for the development of anticitrullinated peptide antibodies in RA.13 In IIM, anti-Jo-1 antibody positive cases are more likely to be smokers, which suggests that smoking and the lung play important roles in IIM development as well.14 A recent case–control study showed that a history of lung disease (sarcoidosis, pneumonia or tuberculosis) reported via questionnaire was associated with IIM, providing further evidence that IIM could start in the lung.15
Both infections and respiratory disease could cause disease through different or overlapping mechanisms but it is unclear whether it is the cause of inflammation or the site where it occurs that is important in immune-system activation. We, therefore, aimed to investigate the association between an infection or respiratory tract disease and future risk of developing IIM.
Methods
Study design
We conducted a population-based case–control study including newly diagnosed cases with IIM and matched controls from the general population. Respiratory tract disease and infections were identified from the time period before IIM diagnosis.
Setting
In Sweden, adult patients with IIM are treated by specialists in internal medicine, rheumatology, dermatology and neurology. There is universal access to publicly funded healthcare, including inpatient, non-primary outpatient and primary care, for all residents. Using the unique personal identification number issued to all Swedish residents, data on demographics, morbidity and mortality from national administrative and clinical registers can be linked.
Study population
The National Patient Register (NPR) contains data on hospitalisations since 1987 and outpatient visits since 2001, listing main and up to 10 contributory diagnoses at each visit. The coverage is 99% for hospitalisations and 80% for outpatient care mainly due to lower reporting from private and psychiatric care. As 95% of Swedish specialists taking care of patients with myositis are hospital based, the coverage of outpatient visits is high. Cases with a first ever visit (index date) listing an International Classification of Diseases (ICD) code for IIM were identified from the NPR (see online supplementary table 1). They were required to have ≥2 visits listing an IIM code in a specialist clinic (rheumatology, internal medicine, dermatology or neurology). To exclude possible miss-coding, a subsequent visit to a specialist clinic between 1–12 months from index date was required to be included in the study.16 Cases were also identified from the Swedish Rheumatology Quality register which includes information provided by rheumatologists on diagnosis, treatment and disease activity including IIM since 2003.
Supplementary file 1
Both register sources were available until December 31 2012 and cases were identified between January 1 2002 and December 31 2011. This allows for a 12-month washout period before study start to exclude prevalent cases and 12 months following index date to allow time for a second visit for individuals identified in the NPR. Because diagnosis is set by name by a rheumatologist in SRQ rather than by ICD code, IIM subdiagnosis was assigned with the following priority: (1) SRQ-given diagnosis, (2) latest diagnosis at a rheumatology clinic. As there is no ICD code available for IBM, the code for PM is commonly used in clinical practice. Therefore, DM is presented separately and PM and IBM are presented together as ‘other IIM’.
Controls were identified from the National Population Register and were matched 10:1 to each individual with IIM on age, sex and place of residence. Controls were required to live in Sweden and to have no history of IIM at the time the matched case was diagnosed (index date).
Identification and classification of exposure
The NPR was used to identify the most recent hospitalisation or specialist outpatient visit from 2001 to index date using ICD codes (see online supplementary table 1) indicating infections or respiratory tract disease (non-infectious). In addition, tuberculosis was identified from the Swedish Tuberculosis Register, to which reporting is mandatory from treating physicians and tuberculosis laboratories. To minimise the risk of reversed causality, a latency period of 1 year between exposure and diagnosis was used (hospitalisations or visits indicating infection of respiratory tract disease in the year before IIM diagnosis were not considered as exposures).
Exposures were classified based on anatomical location: gastrointestinal, skin, or respiratory tract for infections and lower or upper airways for respiratory tract diseases (see online supplementary table 1). Groups were analysed separately and were not mutually exclusive.
Other variables
Sex and age were available from the Total Population Register. Previous healthcare consumption was assessed by counting the number of hospitalisations (excluding exposure-related, pregnancy-related and IIM-related visits) occurring within 5 years prior to exposure or within 1-6 years prior to index date for unexposed individuals to account for the 1-year latency period. We chose to identify visits in this time period to allow all individuals to have the same possibility to present and to exclude visits in close proximity to diagnosis as they could be caused by the outcome.
History of a connective tissue disorder (CTD) was defined as having ≥1 hospitalisation or outpatient indicating CTD before the index date. IIM-associated cancer was defined as having a registration of a malignant cancer within 3 years before or after index date. Cancers were identified from the National Cancer Register to which reporting of cancers is mandatory by clinicians and pathologists and coverage is close to 99% of all malignant cancers in Sweden.17 Having a hospitalisation or outpatient visit indicating fibrosis or lung infiltrates within 3 years before or after the index date was defined as having an IIM lung phenotype.
Statistical analyses
Conditional logistic regression models were used to estimate OR and 95% CI which approximate the relative risk between the exposures and IIM. To investigate if there was a dose–response relationship between exposure and outcome, the number of visits indicating a specific exposure was categorised as 0, 1, 2–4 and ≥5 and added to the model as a single categorical exposure variable.
We performed several sensitivity analyses to test our definition of exposure. First, we investigated whether varying the latency period from 1 year to 0 or 3 years changed the results. Second, we examined a stricter definition of exposure requiring the diagnosis of infection or respiratory tract disease to be listed as the main diagnosis in the NPR. Last, we explored whether the effect differed by varying register sources and time periods used to identify exposures. Only hospitalisations were used to identify more severe infections and respiratory tract disease in one analysis. Because hospitalisation data were available from 1987, we could identify exposures occurring up to 24 years before disease diagnosis. We also used the Prescription Drug Register (PDR), listing all prescribed drug dispensations in Sweden from July 2005, in addition to the NPR. The addition of the PDR enabled us to identify less severe types of exposure treated in primary care where prescription drugs were used (see online supplementary table 1).
Because future IIM patients might have an impaired immune system which can potentially cause poorer health leading to more contact with care providers, previous healthcare consumption was assessed as a proxy for general health, categorised into quartiles and added to the model as a confounding variable in a sensitivity analysis.
To investigate if the associations were primarily caused by other IIM-related conditions, individuals with a history of CTD, IIM-associated cancer or IIM lung phenotype were excluded in a sensitivity analysis.
The study was approved by the Ethics Committee at Karolinska Institutet.
Results
We identified 957 IIM cases and 9476 controls between 2002 and 2011. For cases, mean time since most recent infection and respiratory tract disease was 3.4 and 3.0 years, respectively. The time since infection and respiratory tract disease was similar for controls (table 1).
Descriptive characteristics of 957 identified incident IIM cases and matched controls
The most common infections were pneumonia, gastrointestinal and fungal infections while chronic obstructive pulmonary disease (COPD), asthma and ILD were the most common respiratory tract diseases (see online supplementary table 2).
Previous infections were present in 125 (13%) of IIM cases and 877 (9%) of controls (OR 1.5, 95% CI 1.2 to 1.9). Both gastrointestinal infections (OR 1.9, 95% CI 1.1 to 3.5) and respiratory tract infections (OR 1.6, 95% CI 1.1 to 2.3) were associated with an increased future risk of IIM while skin infections were not (OR 1.2, 95% CI 0.8 to 2.0) (figure 1).

ORs for developing idiopathic inflammatory myopathies (IIM) associated with having a history of hospitalisation and/or outpatient visit for infections or respiratory tract disease (overall and by location). Groups are not mutually exclusive. Exposures occurring within 1 year before IIM diagnosis were not considered. ORs were estimated using conditional logistic regression conditioned on the matching set.
A history of respiratory tract disease was more common in IIM cases compared with controls (n=92, 10% vs n=423, 4%) and was associated with an increased risk of IIM (OR 2.3, 95% CI 1.8 to 3.0). Both lower (OR 2.4, 95% CI 1.8 to 3.0) and upper (OR 1.9, 95% CI 1.3 to 2.7) respiratory tract disease were positively associated with IIM (figure 1).
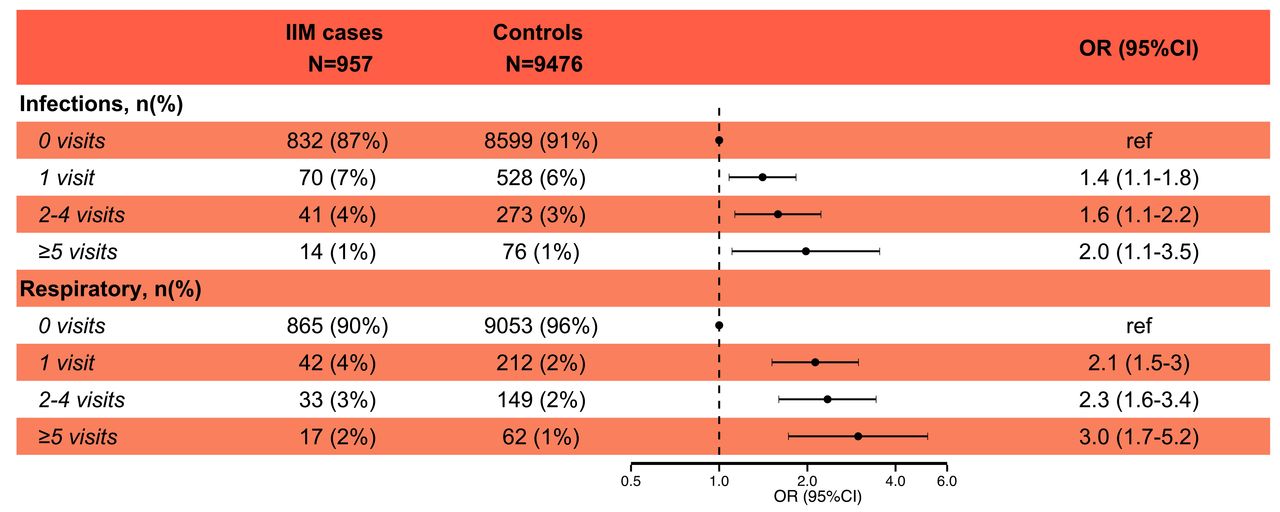
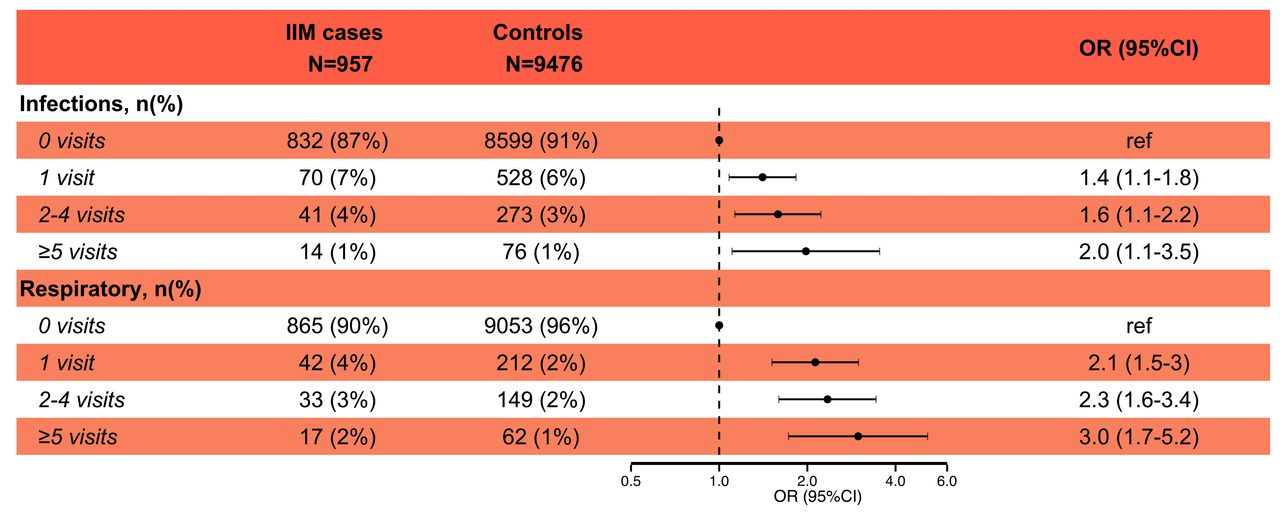
Individuals with more registered visits indicating infections and respiratory tract disease were at an increased risk to develop IIM (figure 2).
{kind=link}
{kind=link}
Effects of having multiple previous visits indicating infections or respiratory tract disease on the future risk to develop idiopathic inflammatory myopathies.CI, confidence interval; OR, odds ratios.
No differences were seen when stratifying by diagnosis for infection (DM OR=1.6 and other IIM OR=1.5) or for respiratory tract disease (DM OR=2.3 and other IIM OR=2.3).
Sensitivity analyses
When the latency period between exposure and outcome was removed, the ORs increased for both infections (1.9 vs 1.5) and respiratory tract disease (2.8 vs 2.1). However, when a latency period of 3 years was used, the ORs remained similar to the main analyses. ORs were similar when requiring the diagnosis of infection or respiratory tract disease to be listed as the main diagnosis in the NPR (table 2).
Sensitivity analysis presenting number of identified idiopathic inflammatory myositis (IIM) cases and controls and corresponding ORs when varying latency time and excluding contributory diagnosis from the National Patient Register
Using different data sources to identify exposure resulted in similar OR estimates (online supplementary table 3).
When adjusting for previous healthcare consumption, the associations decreased but remained significant for both infections (OR 1.3, 95% CI 1.1 to 1.7) as well as for respiratory tract disease (OR 2.2, 95% CI 1.7 to 2.8).
One-third (n=297, 31%) of the cases were removed when individuals with CTDs (n=144, 15%), IIM-associated cancer (n=106, 11%) or IIM lung phenotype (n=84, 9%) were excluded. A positive association remained for both infections (OR 1.4, 95% CI 1.1 to 1.9) and respiratory tract disease (OR 2.2, 95% CI 1.6 to 3.1).
Discussion
In this nationwide population-based case–control study including almost 1000 IIM cases, individuals with a history of an infection had a 50% increased risk of IIM while respiratory tract disease more than doubled the risk. Investigating exposures occurring more than 1 year before the IIM diagnosis enabled us to examine the potential role of exposure long before disease onset which could have a greater influence on disease development rather than exposures occurring in close proximity to disease onset.
Most studies suggesting infections as risk factors for IIM are based on case reports and have examined events in close proximity to diagnosis9 18 or have relied on antibody tests or immune assays in prevalent cases,19–21 making it difficult to infer anything about the temporality of the association. In a study with newly diagnosed PM and DM, similar findings as ours have been reported for infections (IRR=1.70).8
Respiratory inflammatory exposures were found to be associated with IIM in a recent study15 but it only included three specific respiratory outcomes (sarcoidosis, pneumonia and tuberculosis) while our study includes a wider range of respiratory tract diseases. Their identification of IIM using hospitalisation data only likely led to the inclusion of more severe cases of IIM. Relying on questionnaire data may have caused some recall bias, and because the questionnaires were sent out years after diagnoses, only surviving patients could be included. Our findings suggest that respiratory tract disease is a stronger risk factor than infections. This could be due to the location of the inflammation and that the lung could act as the initial site of immune activation and auto-antibody production, as has been seen in RA.12 In addition, the duration of the inflammation may play an important role as the increased inflammatory burden of chronic respiratory tract disease may lead to the break of self-tolerance.
This study has national coverage, enabling us to identify all individuals seeking care for IIM in Sweden and is to our knowledge the largest study to date investigating risk factors for IIM. In a recent study, we developed a stable algorithm to identify patients with IIM from the NPR.16 The same study did, however, demonstrate the difficulties of discriminating between PM and IBM by only using ICD codes from the NPR. Therefore, only DM was analysed separately. If PM and IBM are affected differently by these exposures, we may have underestimated the effect on one and overestimated the effect on the other.
Using national register sources with long follow-up, it was possible to identify exposures occurring up to 10 years before diagnosis. However, with this design we did not identify triggers of disease occurring in close proximity to development of IIM but rather our aim was to identify exposures which occurred years before disease diagnosis. We believe an early time window is relevant for disease pathogenesis, as immunomodulation preceding development of clinically manifested disease could be initiated years before disease onset and therefore may be triggered by exposures occurring long before disease diagnosis. As has been demonstrated in other rheumatic diseases.7 22 Furthermore, by excluding exposures occurring less than 1 year from IIM onset, we aimed to decrease the risk of reversed causality and detection bias. Also, we investigated if there was a difference in the number of cases and controls who had no visits in the NPR prior to index date. Most individuals in the study had at least one previous visit in the NPR and even though there was a difference between cases and controls (13% vs 16% with no visits), we do not believe this explains the associations observed in our study.
Regarding the identification of exposures, the validity of the Swedish patient register is considered high with a positive predictive value (PPV) between 85%–95% for included diagnoses in one study.23 For infections, both sepsis, pneumonia and infections of the central nervous system have a specificity over 95% while for respiratory tract diseases, asthma and COPD have a PPV of 75%–94% and 90%, respectively.24 25 It would be interesting to further group exposures on specific type (eg, bacterial and viral) but as some ICD codes can be used for multiple types of infections, the specificity of these types would be too low.
Respiratory conditions could lead to a respiratory infection but because respiratory infections are only a small proportion of overall infections and results are similar between cases and controls, we believe this does not greatly influence our overall interpretation of the results (see online supplementary figure 1).
We conducted several sensitivity analyses to identify alternative explanations to these findings but the results remained the same. First, the associations found in this study may be due to an underlying cause of both IIM and infection or respiratory tract disease. Cases might have poorer health or an affected immune system increasing the risk of having the exposure. Therefore, previous healthcare consumption was adjusted for in the model as a proxy for general health. Also, individuals with IIM-associated conditions which could have a different disease aetiology were excluded. Second, because severity and timing of exposure could affect the associations, we varied the methods through which exposures were identified. When only hospitalisations were used to identify more severe exposures, it was possible to identify visits dating back to 1987. This did not affect the association for infections while the association with respiratory tract disease was weakened. Furthermore, because some infections and respiratory tract disease are treated in primary care, and may not have been captured, we likely missed some exposures. We addressed this by using drug dispensings, which enabled us to identify all exposures treated with prescription drugs. Still we could not identify exposures that were untreated, for example, common cold. We did observe a dose–response relationship between the number of visits and increased risk to develop IIM for both infections and respiratory tract disease which strengthens our hypothesis.
We cannot rule out that the observed associations are caused by residual confounding. Smoking has been suggested as a risk factor for a subgroup of IIM with anti-Jo-1 autoantibodies and is closely linked to respiratory conditions like COPD, asthma as well as upper respiratory conditions like chronic rhinitis. As we do not have smoking status available in these data, we were unable to adjust for this effect. However, we do not believe smoking would fully explain our results.
Our findings do not provide evidence of a protective effect of infections which has been suggested for autoimmune disease and allergies through the hygiene hypothesis.26 Rather our findings imply that infections in the gastrointestinal and respiratory tracts can increase the risk of IIM. Molecular mimicry where a foreign antigen shares similarities with self-antigens, has been suggested as a potential mechanism.5 Furthermore, gastrointestinal infections could change the gut microbiota, causing autoimmunity by affecting immunoregulatory mechanisms.27 Infections also cause local inflammation as do many respiratory tract diseases like asthma, COPD and rhinitis and an increased inflammatory load or a general activation of the immune system could be involved in disease pathogenesis, possibly through priming of self-reactive lymphocytes and autoantibody production.6 12
In conclusion, we observed associations between IIM and infections of the gastrointestinal and respiratory tract as well as both upper and lower respiratory inflammatory conditions in our study. These findings suggest that external triggers of immunomodulation could be part of the aetiology of IIM and that these events could appear years before clinical manifestations of IIM.
References
Footnotes
Contributors Planning of the study: JS, EA, MH, IL. Analyses: JS. Interpretation of results: JS, EA, MH, IL. Writing: JS, EA, MH, IL.
Funding This study was supported by grants from the Swedish Society of Medicine, Swedish Research Council K2014-52X-14045-14-3, the Swedish Rheumatism Association, King Gustaf V 80 Year Foundation, Konung Gustaf V:s och Drottning Victorias Frimurarstiftelse, Funds at the Karolinska Institutet (KID) and through the regional agreement on medical training and clinical research (ALF) between Stockholm County Council and Karolinska Institutet.
Competing interests IL has received honoraria from Bristol Myers Squibb and is currently receiving a research grant from Bristol Myers Squibb and from Astra Zeneca.
Ethics approval Ethics Committee at Karolinska Institutet.