Article Text

Abstract
Objective To compare the performance of a new three-dimensional MRI sequence (volumetric interpolated breath-hold examination; MR-VIBE) with a conventional T1-weighted sequence (MR-T1) for the detection of erosions in the sacroiliac joints (SIJs) using low-dose CT (ldCT) as reference.
Methods ldCT and T1-MRI and MR-VIBE of 110 prospectively included patients with low back pain and suspected axial spondyloarthritis (axSpA) were scored for erosions by two readers. The presence of erosions on the patients’ level, the erosion sum score, sensitivity and specificity of both MRI sequences using ldCT as a reference as well as agreement between the readers were assessed.
Results MR-VIBE had a higher sensitivity than MR-T1 (95% vs 79%, respectively) without a decrease in specificity (93% each). MR-VIBE compared with MR-T1 identified 16% more patients with erosions (36 vs 30 of 38 patients with positive ldCT findings). The erosion sum score was also higher for MR-VIBE (8.1±9.3) than MR-T1 (6.7±8.4), p=0.003. The agreement on erosion detection was also higher for MR-VIBE (κ=0.71) compared with MRI-T1 (κ=0.56).
Conclusion VIBE detected erosions in the SIJs with higher sensitivity without a loss of specificity and superior reliability compared with a standard T1-weighted sequence. Its value for the diagnosis of axSpA has still to be determined.
- spondyloarthritis
- ankylosing spondylitis
- magnetic resonance imaging
Statistics from Altmetric.com
Introduction
Lesions of the sacroiliac joints (SIJs) are key findings in axial spondyloarthritis (axSpA).1 2 Typical imaging findings include structural changes such as erosions or ankylosis in radiographs and signs of active inflammation such as osteitis in water-sensitive, fat-suppressed sequences in MRI. Structural MRI changes remain to be standardised for the diagnosis and classification of patients with axSpA and are not yet part of a positive MRI definition of sacroiliitis according to the Assessment of SpondyloArthritis international Society (ASAS).1 Moreover, it has been argued that bone marrow oedema might be too non-specific for a reliable diagnosis of axSpA in some cases—a limitation that might be overcome by adding structural lesions to the definition of a positive MRI.3–5 Furthermore, recent studies show that a T1-weighted MRI sequence is at least equally able to depict structural changes compared with radiography6 or even superior.7 State-of-the-art MRI techniques that provide a high contrast of joint space and bone and thinner slices may further improve sensitivity for those changes and, therefore, the diagnostic accuracy of MRI.
The aim of our study was to compare a fast 3D spoiled gradient echo sequence (volumetric interpolated breath-hold examination, MR-VIBE) with a standard T1-weighted sequence (MR-T1) for the detection of erosions in the SIJs8 9 using low-dose CT (ldCT) as standard of reference.
Patients and methods
Subjects
One hundred and ten patients (53 men and 57 women) from the SacroIliac joint MRI and CT (SIMACT) study, a prospective cross-sectional single-centre investigator-initiated study, and 18 healthy age-matched and sex-matched controls were included in this analysis.
The study complies with the declaration of Helsinki and was approved by the local ethics committee. All patients gave written informed consent.
Imaging procedures
All patients, but for ethical reasons (radiation) not the healthy controls, underwent a ldCT scan of the SIJs on a 64-row dual-source scanner (Somatom Definition Flash, Siemens, Erlangen, Germany) as described in detail elsewhere.7 Directly thereafter, the patients underwent a 3-Tesla pelvic MRI (Magnetom Skyra, Siemens, Erlangen, Germany). Besides a standard STIR-weighted sequence, a standard T1-weighted (repetition time 652.0 ms, echo time 11.0 ms, slice thickness 3 mm, flip angle 156°, spatial resolution 410×512 pixels) and a high-resolution iso-voxel VIBE sequence were acquired with a TE of 5.2 and TR of 11.7 ms, a flip angle of 10° and a matrix of 256×256 pixels with a slice thickness of 0.6 mm. Oblique coronal slices parallel to the axis of the second sacral segment were acquired.
Postprocessing and scoring
The ldCT, MR-T1 and MR-VIBE datasets were anonymised separately using Osirix 6.4 (Pixmeo SARL, Bernex, Switzerland). Two readers were trained and scored 15 test cases in consensus before they separately evaluated the images blinded to clinical data and findings of the other modality. However, they had access to a T2-weighted fat-suppressed sequence when scoring the MR images.
Each SIJ was divided into 12 regions (4 quadrants in ventral, middle and dorsal position), resulting in 24 regions per patient.7 The anterior position is defined as ventral to the slices depicting the sacral neuroforamina (<180% circumference of S2). Pelvic organs and fat are seen in the middle of the image. In the middle position, the anterior sacral neuroforamina and the sacral bone is visualised. The posterior position is defined as visualising the entheseal joint compartment that stretches to the posterior-inferior aspect of the joint. Accurate oblique-coronal slice orientation is crucial. For each region, erosions were scored on a four-point scale as described earlier in detail7: 0—no erosions; 1—small isolated erosions (1–2) or questionable single erosion; 2—definite erosions (3-5; <3 mm) or larger single erosion (>3 mm); 3—multiple (>5) or confluent erosions. Therefore, the sum-score ranged from 0 to 72. The total number of erosions was calculated by summing the number in each region.
A patient was considered positive for erosions if any of the 24 regions was assigned a score ≥2. The agreement of both, reader 1 and 2, was considered necessary for a positive finding.
Additionally, the readers were asked to rate their diagnostic confidence using ldCT, MR-T1 and MR-VIBE on a 0-to-10 numerical scale.
Statistical analysis
We performed a contingency table analysis on the patient level to relate the positivity of MR-VIBE and MR-T1 for erosions to ldCT, which served as standard of reference. The inter-rater reliability was evaluated using Cohen’s kappa10 for the presence or absence of erosions on the patients’ level, and the intraclass correlation coefficient (ICC) for the total number of erosions and erosions sum score using a two-way mixed model for single measures. Erosion sum-scores, total numbers of erosions and diagnostic confidence related to ldCT, MR-T1 and MR-VIBE were tested for significant differences by a repeated-measurements analysis of variance with pair-by-pair comparison. The p values were corrected for multiple comparisons using Tukey’s test with individual variances and considered significant if smaller than 0.05. Missing data, for example, incomplete imaging of a region, were included in the analysis as negative for all modalities. Statistics were performed using GraphPad Prism (V.6.0 for MacOS, GraphPad Software, La Jolla, California, USA).
Results
The patients had a mean age of 36.1 years (range, 19–57 years) with a mean duration of chronic back pain of 6 years and 10 months (range, 2 months to 32 years; median: 4 years). Eighty-seven patients had inflammatory back pain (79.1%), 71 (64.5%) were HLA-B27 positive. Fifty-eight patients were diagnosed with axSpA (63% male, 81% HLA-B27 positive) by the expert rheumatologist (axSpA group: 23 with radiographic and 35 with non-radiographic axSpA) and 52 had other diagnoses (non-axSpA group; 34.6% male, 46% HLA-B27 positive).
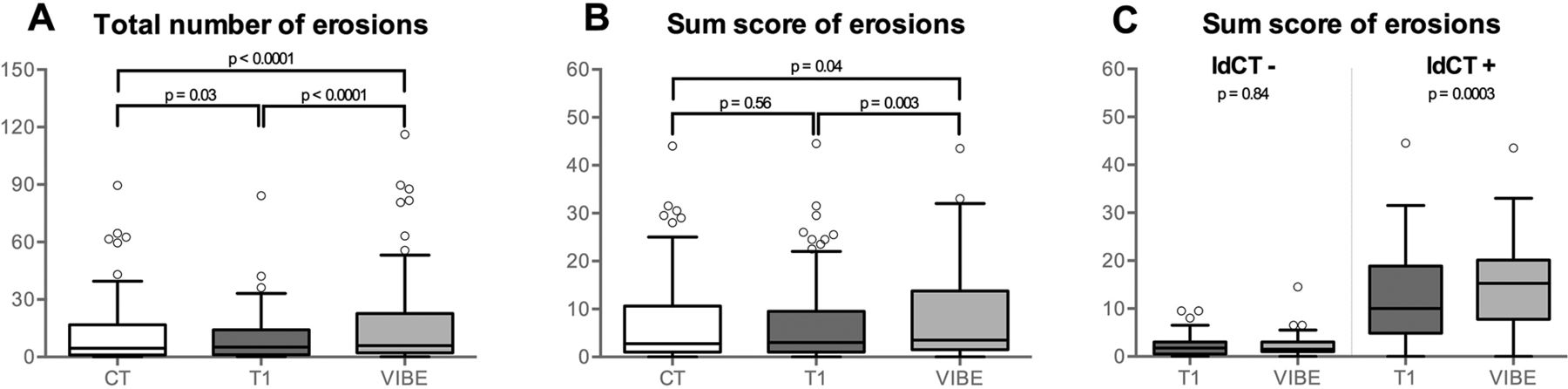
All regions were assessable in T1 and ldCT, in VIBE only 0.3% (10/3072) regions were not fully depicted by the sequence. Results and overview of statistics are presented in a flow chart (figure 1). Using ldCT positivity (score of ≥2) as standard of reference the sensitivity of VIBE (93%) was higher than of T1 (79%) with a similar specificity of 93%. The mean sum score of both readers for erosions was 7.1±9.0 in ldCT, 6.7±8.4 in MR-T1 and 8.1±9.3 in MR-VIBE with a total number of erosions of 11.4±16.5 in ldCT, 9.2±12.1 in MR-T1 and 15.5±21.8 MR-VIBE (see figure 2A and B). For MR-VIBE, the erosion score was higher in patients positive for erosions in ldCT (figure 2C). Examples in figure 3 illustrate that erosions are better visible by ldCT and MR-VIBE than by MR-T1, but also that MR-VIBE is sometimes even more sensitive for erosions than ldCT (figure 3G and I). None of the 18 healthy controls was scored positive for erosions by either reader in MR-T1 or MR-VIBE. When using the clinician’s diagnosis of axial SpA and an erosion score of ≥2 as a cut-off (online supplementary figure S1B) MR-VIBE showed a better sensitivity than MR-T1 (65% vs 53%, respectively) and a better specificity for a cut-off of a ≥1 erosion score (68 vs 53%, respectively) while there was no difference for an erosion score of ≥3 (see online supplementary figure S1).
Supplemental material

Findings in a flowchart. (A) Positivity for erosions in MR-T1 and MR-VIBE is reported separately for patients positive and negative in ldCT. MR-VIBE detected more erosions in patients with erosions in ldCT, while there was no difference in patients who were ldCT-negative. This increases sensitivity without a loss of specificity. (B) For the assessment of inter-reader reliability, we analysed the number of concordant and discordant ratings for MR-T1 and MR-VIBE. Sensitivity, specificity and kappa values are given with the 95% CI in brackets. ldCT, low-dose CT; VIBE, volumetric interpolated breath-hold examination.
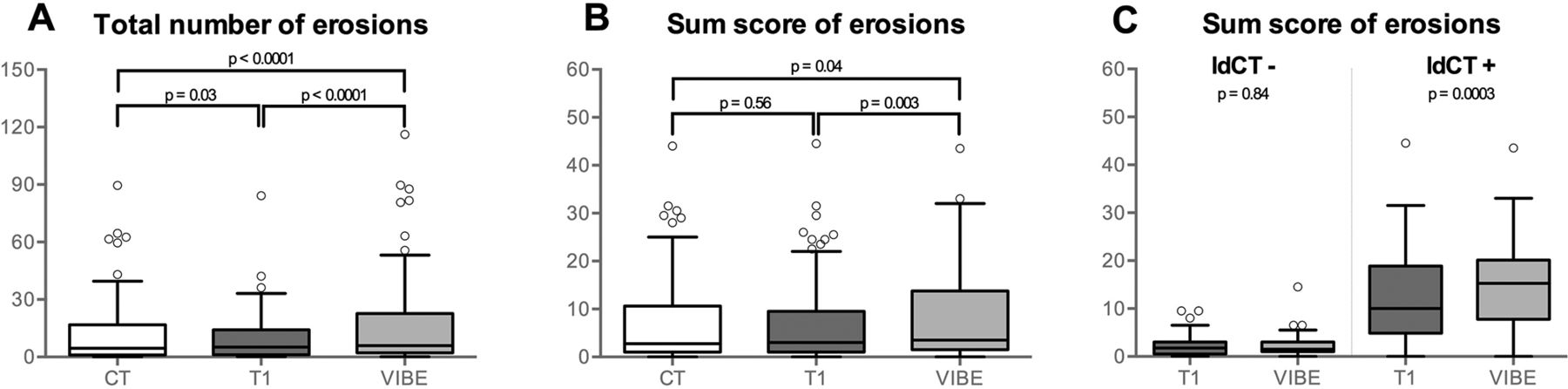
Comparison of results in terms of the total number of detected erosions (A), the erosion sum score (B) and erosion sum score in patients positive and negative for erosions in ldCT (C) for ldCT (CT), MR-T1 (T1) and MR-VIBE (VIBE). MR-VIBE detects significantly more erosions (total number and sum score, A and B) than the other modalities, however, only in patients positive in ldCT (C). The total number of erosions is also significantly lower for MR-T1 compared with ldCT (A). ldCT, low-dose CT; VIBE, volumetric interpolated breath-hold examination.

{kind=link}
{kind=link}
{kind=link}
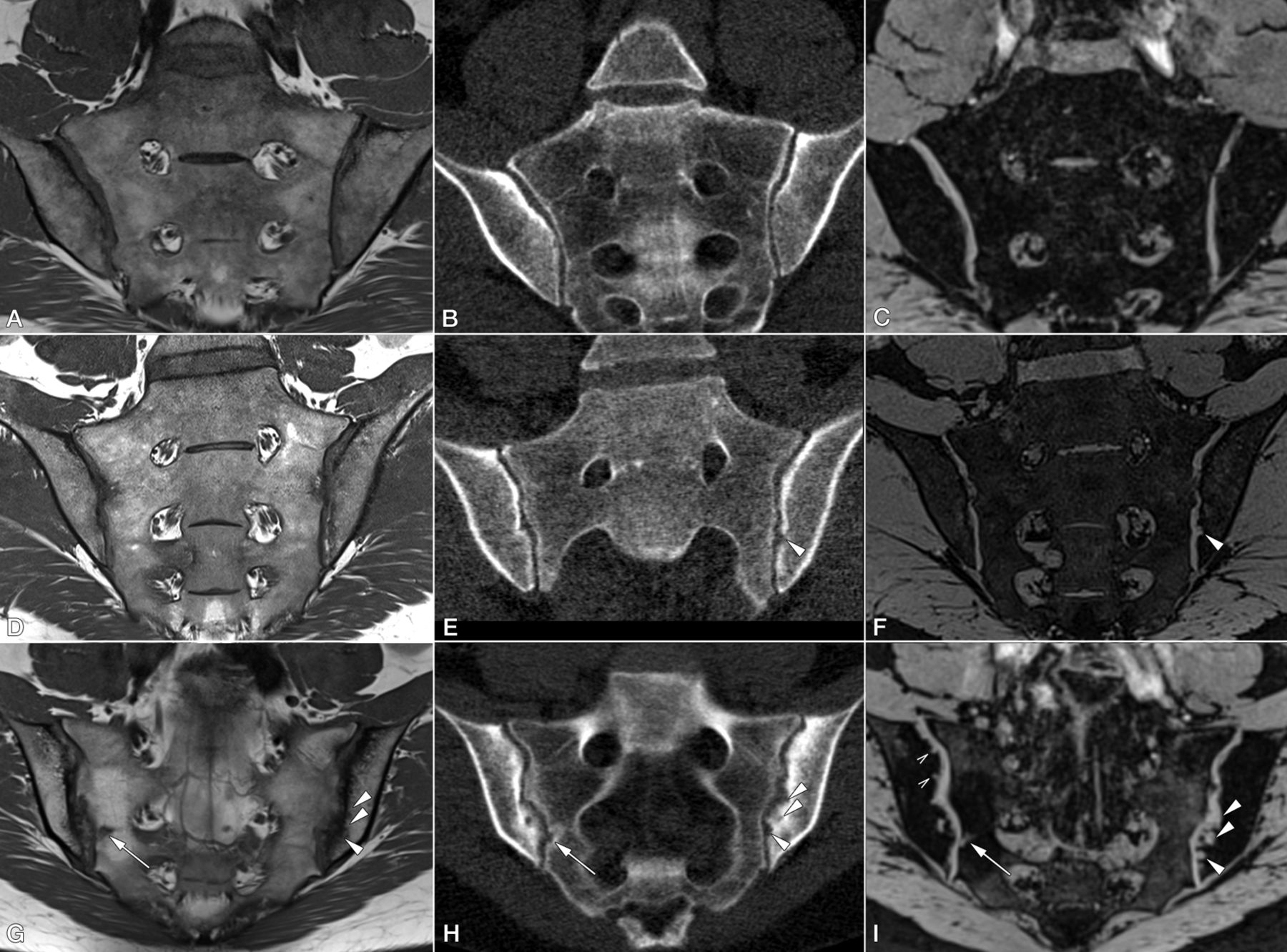
Imaging examples. (A, D and G) Oblique coronal MR-T1 sequence; (B, E and H) ldCT images in oblique coronal reconstruction; (C, F and I) oblique coronal MR-VIBE sequence. Slice positions and orientation are identical for T1 and VIBE. ldCT was reconstructed to match orientation and position. (A–C) normal findings in the SIJ without erosions (erosion sum score 0 for both readers). (D–F) Patient with axial spondyloarthritis with a single but prominent erosion of the left iliac surface that is shown by ldCT and MR-VIBE (arrowheads) but not by MR-T1. (G–I) Patient with axial spondyloarthritis and multiple erosions. Some erosions (arrow) are depicted by all modalities. However, some larger erosions are hardly seen with MR-T1 due to sclerosis, while they are more conspicuous using ldCT and MR-VIBE (arrowheads). The smallest erosions are only depicted with MR-VIBE (open arrowheads). ldCT, low-dose CT; VIBE, volumetric interpolated breath-hold examination.
The agreement on erosion detection on the patients’ level was good for ldCT and MR-VIBE (Cohen’s κ=0.77, 95% CI 0.65 to 0.89 and 0.71, 95% CI 0.57 to 0.84, respectively) and only moderate for MR-T1 (κ=0.56, 95% CI 0.4 to 0.71). The ICC of the total erosion score was comparable for all three imaging modalities (online supplementary table S1).
The diagnostic confidence was highest for MR-VIBE (6.9±2.6), followed by ldCT (6.3±2.7) and MR-T1 (5.6±2.9). These differences were statistically significant for all modalities: MR-VIBE vs ldCT, p=0.006; ldCT vs MR-T1, p=0.002; MR-VIBE vs MR-T1, p<0.0001.
Discussion
This is the first study comparing a modern three-dimensional MR technique (VIBE) with a standard-of-care T1-weighted sequence using ldCT as standard of reference for the detection of erosions in the SIJs. We found that MR-VIBE had a higher sensitivity for erosions than MR-T1 without a decrease in specificity. MR-VIBE identified 16% more patients with erosions compared with MR-T1 (figure 1). MR-VIBE detected significantly more erosions (sum score and total number) than MR-T1 but also than seen on ldCT. When erosion counts were analysed in ldCT-negative patients only, the use of MR-VIBE did not increase the number of false positive findings compared with MR-T1. MR-VIBE performed also better than MR-T1 in terms of inter-rater reliability. Similarly, readers’ overall diagnostic confidence for detecting erosions was significantly higher using MR-VIBE than MR-T1 or ldCT. It has to be shown how much a better and more reliable detection of erosions in the SI-joint can contribute to a better diagnosis of axSpA where all clinical, laboratory and imaging aspects, and not only erosions, are taken into account.
We believe that the higher sensitivity of MR-VIBE vs ldCT can be explained by the high contrast of cartilage and bone in VIBE images and by the image noise in the ldCT scan, which might obscure small lesions. This assumption is also supported by the absence of erosions in MR-VIBE in the healthy controls. The search for sensitive and specific imaging technique for detecting structural lesions of the SIJs has become of high relevance6 11 12 because interpretation of radiographs has repeatedly been shown to be unreliable.13 14
Regarding other studies addressing this topic, Algin et al tested different sequences in a small cohort of 30 patients with SpA and 9 controls and found that 3D-FLASH with fat saturation (VIBE is such a sequence) is the most useful technique to detect cartilage and bone abnormalities.15 In other anatomical locations (eg, hands or knee), similar high-resolution techniques are already standard of care.16 17
The investment of another 3 min for acquiring an MR-VIBE sequence to supplement the standard T1 and STIR MR protocol can increase the sensitivity for erosions and improve diagnostic confidence. That our results obtained with 3-Tesla MRI can also be achieved at lower field strengths is likely but has to be proven. Also, due to the limitations of this single-centre study, the application and interpretation of MR-VIBE should be tested in a larger multicentre trial. The availability of T2 fat-suppressed images during reading might have influenced the result, however, is more close to clinical practice.
In summary, MR-VIBE detected SIJ erosions with higher sensitivity and reliability and in more patients compared with standard T1 MRI in a patient population with low back pain. Thus, the MR-VIBE sequence seems to be a valuable supplement to standard MR protocols for axSpA and its differential diagnosis; however, its value for the diagnosis of axSpA still has to be determined.
Acknowledgments
The authors thank Bettina Herwig for language editing.
References
Footnotes
Handling editor Josef S Smolen
Contributors TD: conception and design of the study, design of scoring system, image scoring, data evaluation, statistical calculations, article draft, critical revision of the manuscript for important intellectual content. JG: patient acquisition, data management, image scoring, critical revision of the manuscript for important intellectual content. JS: patient acquisition, conception and design of the study with critical revision of the manuscript for important intellectual content. DP: patient acquisition, critical revision of the manuscript for important intellectual content. BH: conception of the study, critical revision of the manuscript for important intellectual content. K-GAH: conception and design of the study, design of scoring system, image scoring, data evaluation, with critical revision of the manuscript for important intellectual content and final approval of the version to be published.
Funding This work was supported by a research grant to TD from the Assessment of Spondyloarthritis international Society (ASAS).
Competing interests None declared.
Patient consent Obtained.
Ethics approval Institutional Review Board of Charité Medical School, Berlin, Germany.
Provenance and peer review Not commissioned; externally peer reviewed.