Article Text

Abstract
Objective Anti-citrullinated protein antibodies (ACPA) in rheumatoid arthritis (RA) patients display a unique feature defined by the abundant presence of N-linked glycans within the variable domains (V-domains). Recently, we showed that N-glycosylation sites, which are required for the incorporation of V-domain glycans, are introduced following somatic hypermutation. However, it is currently unclear when V-domain glycosylation occurs. Further, it is unknown which factors might trigger the generation of V-domain glycans and whether such glycans are relevant for the transition towards RA. Here, we determined the presence of ACPA-IgG V-domain glycans in paired samples of pre-symptomatic individuals and RA patients.
Methods ACPA-IgG V-domain glycosylation was analysed using ultra-high performance liquid chromatography (UHPLC) in paired samples of pre-symptomatic individuals (median interquartile range (IQR) pre-dating time: 5.8 (5.9) years; n=201; 139 ACPA-positive and 62 ACPA-negative) and RA patients (n=99; 94 ACPA-positive and 5 ACPA-negative).
Results V-domain glycans on ACPA-IgG were already present up to 15 years before disease in pre-symptomatic individuals and their abundance increased closer to symptom onset. Noteworthy, human leucocyte antigen class II shared epitope (HLA-SE) alleles associated with the presence of V-domain glycans on ACPA-IgG.
Conclusion Our observations indicate that somatic hypermutation of ACPA, which results in the incorporation of N-linked glycosylation sites and consequently V-domain glycans, occurs already years before symptom onset in individuals that will develop RA later in life. Moreover, our findings provide first evidence that HLA-SE alleles associate with ACPA-IgG V-domain glycosylation in the pre-disease phase and thereby further refine the connection between HLA-SE and the development of ACPA-positive RA.
- rheumatoid arthritis (RA)
- anti-citrullinated protein antibodies (ACPA)
- N-linked variable domain (V-domain) glycans
- ‘Sweet’ biomarker
- HLA-SE effects
Statistics from Altmetric.com
- rheumatoid arthritis (RA)
- anti-citrullinated protein antibodies (ACPA)
- N-linked variable domain (V-domain) glycans
- ‘Sweet’ biomarker
- HLA-SE effects
Key messages
What is already known about this subject?
IgG anti-citrullinated protein antibodies (ACPA) are abundantly N-glycosylated within their variable domains (V-domains).
What does this study add?
ACPA-IgG V-domain glycosylation is already extensively present in pre-symptomatic individuals who developed rheumatoid arthritis later in life.
ACPA-IgG V-domain glycosylation increases closer to symptom onset and associates with anti-CCP2 antibody levels pre-disease.
Human leucocyte antigen class II shared epitope alleles (HLA-SE) associate with V-domain glycosylation and therefore predispose to the formation of N-linked glycosylation-sites in ACPA-IgG pre-disease.
Introduction
Rheumatoid arthritis (RA) is hallmarked by the presence of autoantibodies, such as rheumatoid factor (RF) and anti-citrullinated protein antibodies (ACPA).1–3 Several genetic risk factors such as the human leucocyte antigen class II shared epitope (HLA-SE) alleles are associated with ACPA-positive RA. Noteworthy, an association with HLA-SE can only be found in ACPA-positive disease and is mostly lost in ACPA-positive healthy individuals, indicating that HLA-SE-restricted T-helper cell activity is likely involved in the development of ACPA-positive disease and not the initial induction of auto-immunity. Presumably, these T-cells provide help to ACPA-expressing B-cells that have been activated in an earlier phase.4 5 ACPA-IgG are glycoproteins that harbour, like all IgG, N-linked glycans in the Fc-region located at Asn297.6 Remarkably, approximately 90% of ACPA-IgG molecules in sera from RA patients are also abundantly glycosylated within their variable domain (V-domain).7 Structural composition analysis revealed that these V-domain glycans are mostly biantennary complex-type glycans carrying sialic acids.7 8 To undergo N-linked glycosylation, a consensus sequence in the protein backbone is required (N-X-S/T, where X≠P).9 Previously, we have shown that N-linked glycosylation sites in ACPA-IgG V-domains are introduced during somatic hypermutation.10 Furthermore, in a cross-sectional study of indigenous North American individuals, we observed that ACPA-IgG V-domain glycosylation is largely absent in ACPA-positive subjects that did not transit to RA, while N-linked glycans were found on ACPA-positive healthy subjects that later developed RA.11
On the basis of these and other observations, we hypothesise that V-domain glycosylation conveys a selective advantage to ACPA-expressing B-cells, which potentially plays a pivotal role in disease development.10 12 To investigate and understand the presence and acquisition of ACPA V-domain glycans in the phase preceding arthritis in more depth, we now aimed to analyse the presence of V-domain glycans on ACPA-IgG in paired samples of pre-symptomatic individuals and RA patients.
Materials and methods
Patient and public involvement
Patients were involved in this study by donating blood at the Medical Biobank of Northern Sweden, when attending population surveys.
Study cohort
Individuals, diagnosed with RA later in life, were sampled prior to symptom onset (median (IQR) pre-dating time: 5.8 (5.9) years; n=201; 139 ACPA-positive and 62 ACPA-negative) and after diagnosis of RA (n=99, 94 ACPA-positive and 5 ACPA-negative as specificity control). Further, randomly selected control samples (n=43, 3 ACPA-positive and 40 ACPA-negative) were included. The RA patients fulfilled the 1987 American Rheumatism Association (ARA) classification criteria.13 Descriptive cohort information is presented in online supplementary table 1.
Supplemental material
ACPA-IgG isolation and V-domain glycan analysis
Experimental procedures for ACPA-IgG isolation, glycan release, labelling, UHPLC analysis as well as data processing and analysis are described in detail in the online supplementary materials and methods. Percentage ACPA-IgG V-domain glycosylation was calculated based on the following formula: ((GP19+GP23+GP24)/(GP4+GP8+GP14))×100.11 14
Results
ACPA-IgG V-domain glycan profiles were detected in ACPA-positive pre-symptomatic individuals and RA patients
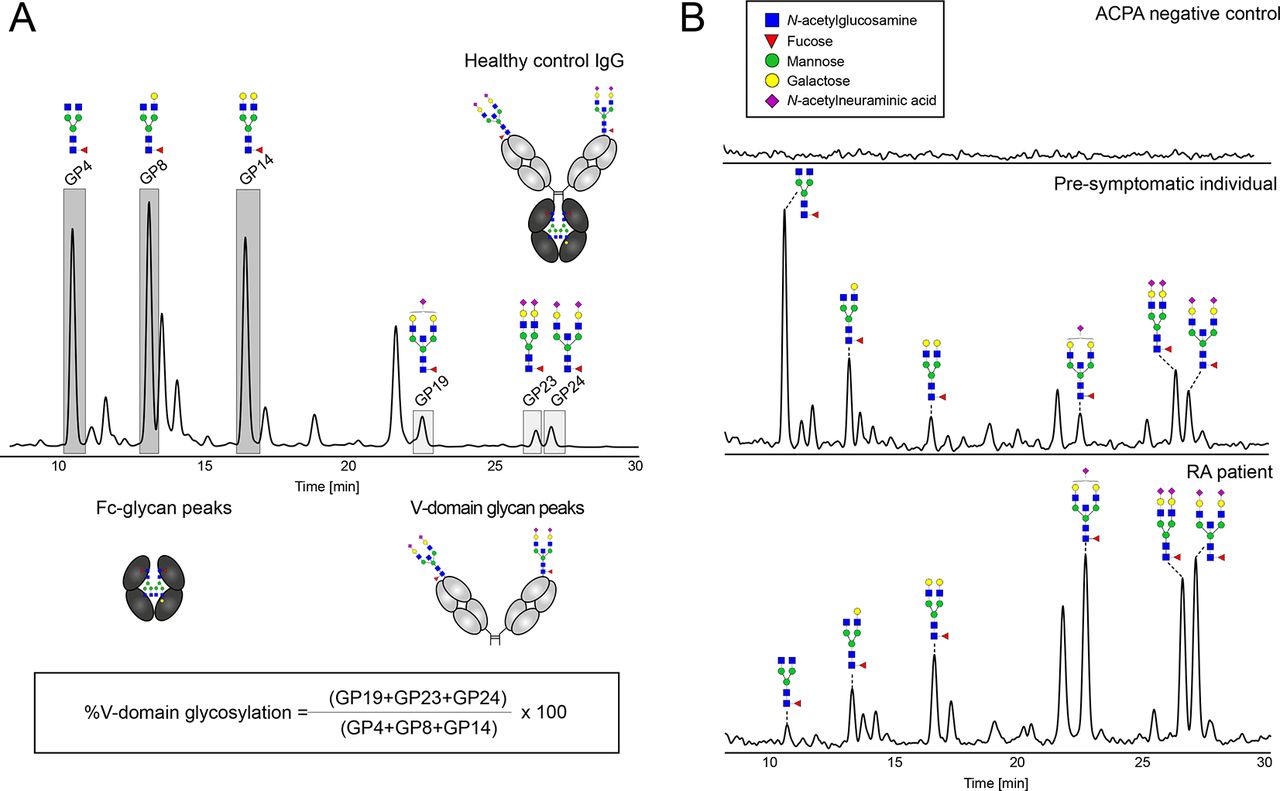
We analysed individuals who were sampled before symptom onset, after diagnosis of RA and randomly selected ACPA-positive and ACPA-negative control samples from the same population. Chromatographic glycosylation peaks (figure 1A) could be observed for captured ACPA-IgG of 94 out of 201 pre-symptomatic individuals (89 ACPA-positive), 80 out of 99 RA patients (78 ACPA-positive) and 2 out of 43 control samples (1 ACPA-positive and 1 with an anti-CCP2 antibody level <25 AU/mL). The results obtained strengthen the reliability of the method used, as from the samples displaying glycan profiles only 8 (4.5%) were derived from ACPA-negative individuals (anti-CCP2 antibody level below 25 AU/mL) compared with 168 glycan profiles (>95%) derived from samples obtained from ACPA-positive individuals (online supplementary table 2 and online supplementary figure 1). Of note, in 68 ACPA-positive samples (40.5%) no glycan profiles, including Fc-glycans (positive control), could be detected, indicating a limitation of assay sensitivity.
Supplemental material

Representative UHPLC spectra of released N-glycans. (A) UHPLC chromatogram of healthy control IgG after IgG capturing and schematic representation of Fc-domain and variable domain (V-domain) derived glycosylation peaks. The six chromatographic peaks (alignment based on Pucić et al 16) used for the calculation of %V-domain glycosylation are highlighted and the formula is visualised. (B) UHPLC spectra of released N-glycans after ACPA-IgG capturing from ACPA-IgG negative control sample (no detectable glycan peaks), ACPA-IgG positive pre-symptomatic individual (V-domain glycosylation of 55%) and ACPA-IgG positive rheumatoid arthritis sample (V-domain glycosylation of 324%). Assigned are the GP4, GP8, GP14, GP19, GP23 and GP24 chromatographic peaks of the IgG glycome based on literature.7 8 Blue square: N-acetylglucosamine, green circle: mannose, yellow circle: galactose, red triangle: fucose, pink diamond: α2,6-linked N-acetylneuraminic acid. ACPA, anti-citrullinated protein antibodies.
ACPA-IgG V-domain glycosylation rises towards symptom onset and is already present years before
To address the question when V-domain glycosylation first appears, matched paired individuals were sampled before symptom onset (between −15 and −0.5 years) as well as after diagnosis of RA (between +0.5 and+3 years) and analysed for ACPA-IgG V-domain glycosylation (figure 1A).7 The data obtained revealed that V-domain glycosylation was already present in pre-symptomatic individuals (figure 2A). Interestingly, ACPA-IgG V-domain glycosylation increased over time (p<0.001) reaching a mean of 111.4% at symptom onset, showing that, on average, more than one N-glycan is present within the V-domain of these ACPA-IgG. Likewise, also analyses of the 29 matched pairs, with detectable V-domain glycan peaks, showed an increase of ACPA-IgG V-domain glycosylation towards disease onset (p=0.043, paired t-test) (figure 2B). Furthermore, we observed that rising V-domain glycosylation levels in pre-symptomatic individuals correlated moderately with anti-CCP2 antibody levels (rs=0.504, p<0.001) (figure 2C). This correlation could not be detected anymore after disease development (figure 2D).

{kind=link}
{kind=link}
ACPA-IgG variable domain (V-domain) glycosylation levels of pre-symptomatic individuals and rheumatoid arthritis (RA) patients. (A)Percentage IgG V-domain glycosylation of healthy control IgG samples, captured ACPA-IgG from pre-symptomatic individuals and RA patients. (B) Percentage ACPA-IgG V-domain glycosylation followed over pre-dating time (−15 years before until +3 years after symptom onset) for 29 matched paired pre-symptomatic and RA samples that showed detectable V-domain glycan profiles. 0 indicates onset of RA. ACPA-IgG V-domain glycosylation increases towards disease onset (p=0.043, paired t-test). (C) Scatter plot of percentage ACPA-IgG V-domain glycosylation and anti-CCP2 antibody levels in pre-symptomatic individuals (rs=0.504, p<0.001). (D) Scatter plot of percentage ACPA-IgG V-domain glycosylation and anti-CCP2 antibody levels in RA patients (rs=0.169, p=0.133). Significant differences are indicated by ***p<0.001 and ****p<0.0001. The cut-off used for ACPA-IgG V-domain glycan peaks is defined as the average of the area under the curve (AUC) sum intensity of all blank sample peaks plus x* standard deviation (x=value defined as such that all blank and ACPA-negative healthy donor control samples fall below the cut-off). ACPA, anti-citrullinated protein antibodies
ACPA-IgG V-domain glycosylation associates with HLA-SE
To investigate possible associations of ACPA-IgG V-domain glycosylation pre-disease and cohort characteristics, we performed a logistic regression analysis using detectable ACPA-IgG V-domain glycans versus non-detectable glycan profiles as an outcome. The statistical analysis showed no association between V-domain glycosylation and ‘sex’ or ‘ever smoking’. Interestingly, an association between ACPA-IgG V-domain glycosylation and HLA-SE was observed (OR=1.97, p=0.043). This association remained significant after adjusting for anti-CCP2 antibody status, and pre-dating time (OR=2.46, p=0.023) as well as after adjusting for RF and pre-dating time (OR=2.54, p=0.015) (table 1). However, this association was non-significant after correcting for anti-CCP2 antibody levels although a clear trend remained (OR=2.06, p=0.086). In contrast, no association was found when a reciprocal analysis was performed addressing the question whether HLA-SE associates with anti-CCP2 antibody positivity pre-disease (OR=1.01, 95% CI 0.51–1.98).
Logistic regression analysis of samples from pre-symptomatic individuals with detectable versus non detectable ACPA-IgG glycan profiles
Discussion
In this study we have captured ACPA-IgG from pre-symptomatic individuals and RA patients and analysed their glycan profiles using UHPLC. The observed glycan profiles were derived from samples of ACPA-positive individuals in more than 95% of the cases. These results indicate the high reliability of the implemented methodology (online supplementary figure 1). Glycan profile detection in 8 out of 107 ACPA-negative samples may be explained by the presence of ACPA-levels slightly below the ELISA cut-off. In fact, three out of these eight subjects in whom ACPA V-domain glycans were detected, while displaying ACPA-negativity based on the ELISA cut-off, had been tested positive for reactivity towards other citrullinated-antigens, which could explain capturing by the CCP2-coated beads. A clear limitation of the present study is that not all ACPA-positive samples could be analysed for the presence of V-domain glycans as not all glycan profiles, including Fc-glycans, could be detected. This is likely due to technical constraints such as low ACPA-levels or limited sample amounts.
At present ACPA-IgG is used as one of the most relevant biomarkers in RA. However, ACPA detection in subjects at risk does not always correlate with the progression to RA.15 Our data show that N-linked V-domain glycans are a specific feature of ACPA-IgG, which can be present already years before RA onset. These results are in line with a recent study indicating that the presence of V-domain glycans could potentially be used as a biomarker to identify ACPA-subjects at risk to develop RA.11 Together our studies show that V-domain glycosylation occurs in almost all ACPA-positive subjects who will develop RA despite different ethnic and environmental backgrounds. Moreover, the current study shows that V-domain glycans appeared already up to 15 years before diagnosis (figure 2B). Furthermore, our data reveal that V-domain glycosylation increases towards disease onset, conceivably due to the generation of de novo N-glycosylation sites or the expansion of N-glycosylation site-bearing clones, and that this increase associates with higher ACPA-levels (figure 2C). These results are in line with the notion that ACPA-expressing B-cells gain a selective advantage through the generation of V-domain glycans.
Additionally, we did observe an association between ACPA-IgG V-domain glycosylation pre-disease and HLA-SE alleles. This association remains after including anti-CCP2-status into the model. Likewise, a clear, although non-significant trend remains after correcting for anti-CCP2 antibody levels.
Unfortunately, we could not study a possible correlation between V-domain glycosylation and epitope spreading of the ACPA-response as we did not have sufficient data on the citrullinated-epitope recognition profile of the samples available. Nonetheless, an association between HLA-SE status and ACPA-IgG V-domain glycosylation is intriguing as it suggests that HLA-SE predispose to the formation of N-linked glycosylation-sites in ACPA pre-disease and not to ACPA-positivity itself. This assumption is in line with findings indicating that the association between HLA-SE and ACPA-positivity is mostly lost in healthy individuals.4 5 However, although appealing, additional replication is warranted as the present study could have introduced bias due to for example, limited sample size or assay sensitivity. Nonetheless, we consider it highly relevant to perform such studies as it could provide novel insights into the role of HLA-SE-restricted T-cells on the development of ACPA-positive RA. HLA-SE T-cells might facilitate the introduction of N-linked glycosylation sites on ACPA-expressing B-cells allowing their expansion as conceivably explaining the rise in ACPA-levels pre-disease.
In summary, our data disclose that V-domain glycosylation precedes the development of ACPA-positive RA and may serve as aid to improve current algorithms predicting RA-development thereby allowing early treatment of high risk individuals. Noteworthy, our findings suggest that the action of HLA-SE could be explained by the contribution to facilitate the introduction of N-linked glycosylation sites into ACPA-IgG pre-disease.
Acknowledgments
The authors would like to thank the Department of Biobank Research at Umeå University, Västerbotten Intervention Programme, the Northern Sweden MONICA study and the County Council of Västerbotten for providing data and samples. We would like to thank Dr. Jan Wouter Drijfhout (LUMC, Leiden) for providing the CCP2 peptide.
References
Footnotes
Handling editor Prof Josef S Smolen
Correction notice This article has been corrected since it published Online First. An error has been corrected in the abstract.
Contributors TK: study concept and design, conducting experiments, aquisition of data, analysis and interpretation of the results, drafting and revising the manuscript, final approval of the manuscript. KAvS: study concept and design, conducting experiments, aquisition of data and interpretation of the results, critical revision and final approval of the manuscript. LH: study concept and design, methodology design, conducting experiments, aquisition of data, critical revision and final approval of the manuscript. AL: statistical analyses, interpretation of the results, critical revision and final approval of the manuscript. HK: statistical analyses, critical revision and final approval of the manuscript. MW: methodology design, critical revision and final approval of the manuscript. TWJH: interpretation of the results, critical revision and final approval of the manuscript. HUS: study concept and design, interpretation of the results, critical revision and final approval of the manuscript. RT: study concept and design, interpretation of the results, drafting and revising the manuscript critically, final approval of the manuscript. SR-D: study concept and design, statistical analyses, interpretation of the results, drafting and revising the manuscript critically, final approval of the manuscript. Department of Biobank Research at Umeå University: providing patient samples and data. Västerbotten Intervention Programme: providing patient samples and data. The Northern Sweden MONICA study: providing patient samples and data. The County Council of Västerbotten: providing patient samples and data. J.W. Drijfhout: providing the CCP2 peptides.
Funding This work has been financially supported by ReumaNederland (17-1-402), the IMI funded project RTCure (777357), ZonMw TOP (91214031), the Swedish Research Council (VR 2017-00650) as well as the King Gustaf V’s 80-Year Fund, the King Gustaf V’s and Queen Victoria’s Fund and the Swedish Rheumatism Association.
Competing interests HUS, TWJH and REMT are mentioned inventors on a patent on ACPA-IgG V-domain glycosylation.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.