Article Text

Abstract
Axial spondyloarthritis (axSpA) encompasses both radiographic and non-radiographic axSpA. It is a chronic inflammatory disease with a predilection for involving the axial skeleton. The most common presenting symptoms are chronic back pain and spinal stiffness but peripheral and extra-musculoskeletal manifestations occur also frequently. The diagnosis of axSpA relies on the recognition of a clinical pattern of the disease, based on clinical, laboratory and imaging features. The Assessment in SpondyloArthritis international Society classification criteria for axSpA are valid and well implemented for research purposes. Sustained disease activity, measured by validated tools such as the Ankylosing Spondylitis Disease Activity Score, leads to irreversible structural damage and poor functioning and therefore should be abrogated. As part of the management algorithm, non-steroidal anti-inflammatory drugs remain as the first line of pharmacological treatment besides physiotherapy. As a second line, tumour necrosis factor inhibitor and interleukin-17 inhibitor are available but recently Janus kinase inhibitors have also shown efficacy in improving symptoms of the disease.
- spondylitis
- ankylosing
- epidemiology
- outcome assessment
- health care
Statistics from Altmetric.com
Introduction
Spondyloarthritis (SpA) is a chronic inflammatory disease that either involves predominantly the axial (ie, the sacroiliac joints (SIJ) and the spine; axial SpA (axSpA)) or the peripheral skeleton (ie, joints of the limbs; peripheral SpA (pSpA)).1 The prototype of axSpA is radiographic axSpA (r-axSpA), also known as ankylosing spondylitis and historically described according to the modified New York classification criteria (mNY).2 The hallmark feature of r-axSpA is commonly referred to as ‘radiographic sacroiliitis’. The term, however, is misplaced because sacroiliitis implies inflammation, but only structural damage, rather than inflammation, is visible on radiographs.
By the time that structural abnormalities become apparent on pelvic radiographs, patients typically had already symptoms, such as pain, for several years. Efforts to reduce the diagnostic delay of axSpA led to the recognition of patients presenting with a clinical phenotype similar to r-axSpA except for the absence of definite damage visible on pelvic radiographs. Unlike radiographs, MRI allows direct visualisation of inflammation.3 In the mid-1990s, MRI demonstrated that these patients have inflammation on the SIJ often predating radiographic damage for years.4
This evidence led the Assessment in SpondyloArthritis international Society (ASAS) to coin the term ‘axial spondyloarthritis’ to refer to the entire spectrum of the disease, covering both patients who have already developed definite radiographic damage in the SIJ (r-axSpA) and patients without such damage (non-radiographic axSpA (nr-axSpA)).5 6 Patients with nr-axSpA represent early forms of axSpA, in a disease continuum, in which some, but not all, eventually progress to r-axSpA. For the purpose of diagnosis, in clinical practice, the distinction between r-axSpA and nr-axSpA is less relevant, and preference should be given to the term axSpA to refer to all patients.7
Epidemiology
AxSpA usually starts in the third decade of life with a male to female ratio of 2:1 for r-axSpA, and with an equal sex distribution among patients with nr-axSpA. The percentage of patients with nr-axSpA is increasing over time, which is partly due to its better recognition8 (figure 1).
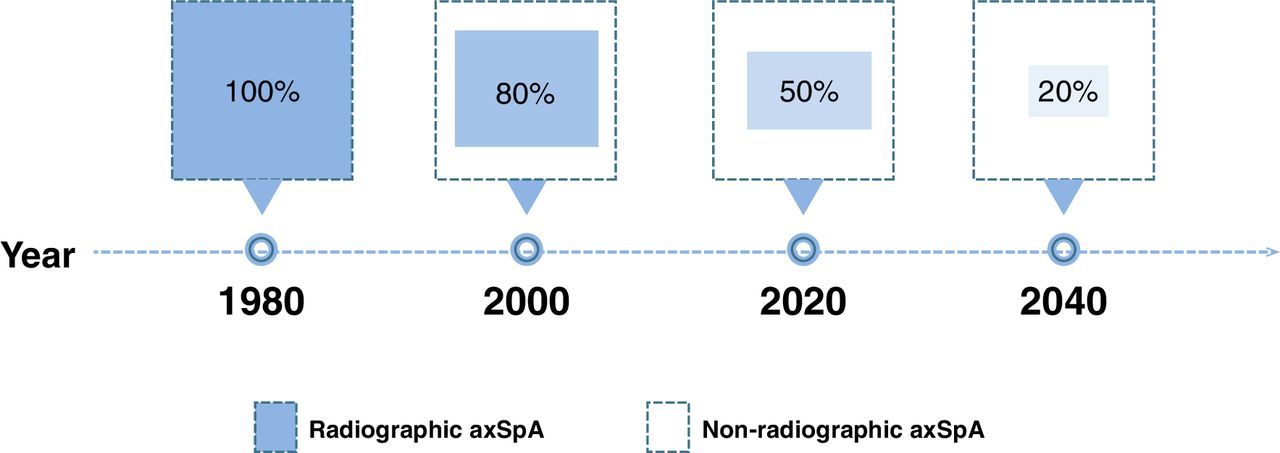
Distribution of axial spondyloarthitis subtypes over time. The graph represents an estimation of the prevalence ratio between non-radiographic and radiographic axial spondyloarthritis, showing the estimated percentage of patients with radiographic axial spondyloarthritis for each period at the time of diagnosis. Adapted from Benavent et al. Clin Rheumatol. 2021 Feb;40(2):501–512. axSpA, axial spondyloarthritis.
Most data on the prevalence of axSpA pertain to r-axSpA with a prevalence ranging widely from 0.1% to 1.4%. Differences in study design can explain some variability; however, it is well-known that the prevalence of the disease is highly affected by the background prevalence of the human leucocyte antigen (HLA)-B27, its major genetic association.9
Populations with high background prevalence of HLA-B27 show higher rates of axSpA, such as in Northern Europe and among the native peoples of the circumpolar arctic and subarctic regions of Eurasia and North America.10 In contrast, the near absence of axSpA in southern Africa and the low rates in Japan is linked to low HLA-B27 prevalence. AxSpA prevalence (including both r-axSpA and nr-axSpA) varies between 0.3% and 1.4%,11 12 and the estimates for the entire group of SpA (including axSpA and pSpA) from 0.3% to 1.9%, making it at least as prevalent as rheumatoid arthritis.13
Pathogenesis
The primary pathophysiology in axSpA occurs in the entheses and in the subchondral bone.14 15 Although synovitis may also occur, it is a secondary process originating from signals in the enthesis.14 Entheseal and bone pathology occurs in individuals with a specific genetic background. Genetic studies estimate a heritability greater than 90%. The most important genetic risk factor is HLA-B27, but other major histocompatibility complex (MHC) variants are also involved.16 Two non-MHC genetic loci have also been associated with axSpA, the endoplasmic reticulum aminopetidase (ERAP) and the interleukin-23 (IL-23) receptor.17 Polymorphisms on these loci have functional consequences and associate with disease manifestations.18 19 Of note, ERAP1 associates with axSpA only in HLA-B27-positive cases, indicating the relevance of peptide presentation by HLA-B27.20
Entheses are load-bearing structures with a specific immune microenvironment that, in susceptible individuals, may be activated by mechanical and microbial triggers.14 There is increasing evidence of the importance of mechanical stress in the onset and progression of axSpA.21 22 In addition, damage to the skin, induced by psoriasis, and to the intestinal mucosa by inflammatory bowel disease (IBD), facilitate exposure to pathogens. This mechanism may happen even in asymptomatic patients. In fact, subclinical gut inflammation has been linked to earlier disease onset and worse prognosis.23 Dysbiosis is thought to be of relevance in the link between the intestine and SpA pathogenesis15 (figure 2).

Pathogenesis scheme for axial spondyloarthritis. A schematic presentation of the various aspects that play a role in the pathogenesis of axial SpA. BMP, bone morphogenetic protein; EMM, extra-musculoskeletal manifestation; ERAP, endoplasmic reticulum aminopetidase; HLA, human leucocyte antigen; IL, interleukin; ILC, innate lymphoid cell; SpA, spondyloarthritis; TNF, tumour necrosis factor.
Axial inflammation, bone destruction and new bone formation are key events in the pathophysiology of axSpA. Even though, it is yet to be fully clarified the mechanisms that govern their interplay, several studies using bone biopsies, animal models and imaging had already yielded important insights. Subchondral bone marrow oedema (BME) visible on MRI is the earliest detectable change in biopsy specimens.24 25 BME is then replaced by an inflammatory granulation tissue, containing also adipocytes and fat vacuoles, that erodes the subchondral bone plate, but also has bone-forming capabilities.26 Fatty lesions on MRI are thought to be the imaging translation of this repair tissue.27
Thus, inflammation can lead either to bone destruction or to bone formation. One hypothesis defends that bone destruction, driven by the contact between osteoblasts and osteoclasts (by receptor activator of NF-κB–receptor activator of NF-κB ligand interactions), prevails with sustained inflammation, while bone formation implies that inflammation subsides and the absence of osteoclasts.28 In axSpA, inflammation is thought to fluctuate, which allows repair and an anabolic response driven by bone morphogenic proteins and Wnt proteins.14 Several clinical studies corroborate the observation that inflammation leads to subsequent new bone in axSpA.28–35 Whether or not a repair mechanism (fatty lesions) mediate this effect, remains an open question.36
Tumour necrosis factor (TNF)-α and IL-23/IL-17 are, thus far, identified as the major pro-inflammatory cytokine pathways in axSpA.14 The pivotal role of TNF-α in the pathogenesis of axSpA is supported by the success of TNF inhibitors (TNFi) in controlling the symptoms of the disease,37 More recently, IL-17-inihibitors (IL-17i) have also proved effective in axSpA, but not IL-23-inhibitors (IL-23i).38 These results offer important clues on the role of the IL-23/IL-17 pathway in SpA. IL-17 is produced by T helper 17 (TH17) cells in response to IL-23, in a later stage of their differentiation. The inefficacy to IL-23i in controlling axial manifestations suggests, however, an uncoupling between the two cytokines. The fact that IL-17 secretion might take place in the absence of IL-23 and that cell types other than TH17, such as the type 3 innate lymphoid cells, produce IL-17 independently of IL-23 supports this claim.38
Both TNF-α and IL-17 induce bone destruction and cause a downregulation of osteoblast function when osteoblasts and osteoclasts interact. In absence of osteoclasts, as in axSpA, however, these cytokines lead to bone formation,39 suggesting their inhibition can, potentially, interfere with the disease progression.
Clinical, laboratory and imaging features
The most common, and often presenting, symptom of axSpA is chronic (lasting >3 months) almost daily back pain (CBP), which is frequently accompanied by morning stiffness. Pain and stiffness usually involve the lower spine and the buttocks, but any level of the spine can be affected. CBP in axSpA typically has an insidious onset and has inflammatory characteristics: it is worse in the second part of the night and in the morning, it is relieved with activity and worsened by rest and usually improved by non-steroidal anti-inflammatory drugs (NSAIDs). Several criteria have been proposed to define inflammatory back pain (IBP).40 41 Though typical, not all axSpA patients have IBP. In fact, up to one third of patients present with mechanical back pain,42 also diseases other than axSpA may present with IBP.43 In axSpA, axial inflammation (synovitis and enthesitis) leads to irreversible structural damage and both can limit the mobility of the spine.44 However, limited spine mobility is usually a late disease manifestation and, although a characteristic feature of axSpA, it may also occur in patients with CBP from diseases other than axSpA.45
In addition to CBP, patients with axSpA can present peripheral manifestations. Arthritis and enthesitis are the most common peripheral manifestations in axSpA, each occurring in approximately 30% of the patients.46 Peripheral arthritis, presenting as a swollen and painful joint, is usually an asymmetrical monoarthritis/oligoarthritis, and involves predominantly the lower extremities. Peripheral enthesitis usually manifests with pain, stiffness and/or tenderness. The most common affected entheses are at the insertion of the Achilles tendon and the plantar fascia. However, axial enthesitis (eg, at the insertion of the anterior longitudinal ligament) together with synovitis of the axial joints (costovertebral, costosternal and manubriosternal joints), can also be involved causing chest/back pain. Dactylitis (sausage digit), which is a swelling of a finger or toe as the consequence of a combination of synovitis, tenosynovitis and enthesitis is a typical feature of axSpA but it occurs in <10% of the patients.46
Patients with axSpA may present concomitant extra-musculoskeletal manifestations (EMMs), that is, uveitis, IBD and psoriasis. Uveitis is associated with HLA-B27 positivity,47 and is the most frequent EMM, occurring in approximately 25% of the patients.46 Uveitis presents typically as unilateral acute anterior uveitis (AAU), and frequently alternates from one eye to the other. Psoriasis (10%) and IBD (5%–10%), including both ulcerative colitis and Crohn’s disease, are less frequent EMM of axSpA.46 48 In severe cases, patients might present with constitutional symptoms, such as low-grade fever and weight loss. Heart (eg, aortic valve insufficiency), lung (restrictive lung disease) and kidney (eg, IgA nephropathy) involvement can also occur in axSpA.
Different laboratory and imaging features are found in axSpA. The presence of HLA-B27, tested in peripheral blood samples, is positive in 70%–90% of patients. Inflammation can be quantified by measuring the levels of the C reactive protein (CRP) or the erythrocyte sedimentation rate (ESR). However, up to 60% of patients with axSpA have symptoms despite normal acute phase reactants.49 Inflammatory lesions of the axial skeleton can be seen with MRI of the SIJ and the spine. The ASAS group define active sacroiliitis as the presence of BME on MRI in subchondral bone highly suggestive of SpA.50 On the MRI of the spine, the presence of ≥5 corner inflammatory lesions discriminates well between axSpA and no axSpA.51 Radiographs can detect structural abnormalities (sclerosis, erosions, joint space narrowing/widening or ankylosis) that occur in the SIJ and in the spine. The mNY grading system is traditionally used to quantify structural damage in the SIJ,2 with a score of 0 (normal), 1 (suspicious changes), 2 (minimal abnormalities), 3 (unequivocal abnormalities) and 4 (total ankylosis) given to each joint. Definite structural changes (radiographic ‘sacroiliitis’) are defined as bilateral grade ≥2 or unilateral grade ≥3. Structural lesions can also be seen with MRI both in SIJ and in the spine (eg, erosions, sclerosis and fatty lesions). Definitions of each lesion have been published.52 53
There are gender differences in the presentation of axSpA. Male patients are more likely to be HLA-B27 positive,54 a feature associated with imaging abnormalities typical of r-axSpA and with a higher likelihood of AAU.47 55 Female patients, on the other hand, are less likely to show inflammation and structural damage on imaging studies, and to be positive for HLA-B27.54 A lower prevalence of HLA-B27 is associated with a higher likelihood of peripheral features and EMM (especially psoriasis) in axSpA.56–59
Diagnosis
The diagnosis of axSpA relies on recognising the pattern (the ‘Gestalt’) of axSpA, taking into account all features that are present, as well as those that are absent and considering alternative diagnoses. SpA features are identified during the history taking (eg, family history, back pain characteristics, response to NSAIDs, history of enthesitis/arthritis/dactylitis or EMMs), physical examination (eg, arthritis) and in laboratory (eg, CRP and HLA-B27) and imaging (eg, MRI-SIJ) exams. Early diagnosis allows early treatment aiming at reducing the disease burden and improving long-term prognosis. However, the SpA-pattern is sometimes difficult to recognise, especially in early disease and in absence of objective findings leading to uncertainty. In clinical practice, clinicians may use diagnostic algorithms for guidance42 (figure 3).

ASAS adaptation of the Berlin algorithm. ASAS, Assessment in SpondyloArthritis international Society; HLA, human leucocyte antigen; SIJ, sacroiliac joints; SpA, spondyloarthritis. SpA features: inflammatory back pain, alternating buttock pain, good response to non-steroidal anti-inflammatory drugs, peripheral arthritis, enthesis, dactylitis, psoriasis, inflammatory bowel disease, uveitis, elevated acute phase reactants, preceding infection, family history. Adapted from van den Berg et al.42
Diagnostic algorithms are based on probability rules. The probability of the disease is calculated considering each feature’s ability to discriminate between axSpA and no axSpA. Positive and negative likelihood ratios (LR+ and LR−) are easy ways to quantify diagnostic value (table 1).
Diagnostic value of SpA features
The higher the LR+ the more likely a diagnosis of axSpA if the feature is positive. Conversely, the lower the LR− the less likely the diagnosis if the feature is negative. The LR+ of present features and the LR− of absent features are multiplied to get the LR-product.60 Clinicians may follow the diagram in figure 2 to guide their diagnostic reasoning. Importantly, the diagram assumes that the patient comes from a population with a 5% prevalence of axSpA (ie, patients with CBP in general practice).4
It should be kept in mind that some features, especially peripheral features and EMM, absent at presentation may occur later on.58 On the other hand, a negative MRI of the SIJ for the presence of BME is unlikely to become positive within 1 year.61 Thus, usually repeating the scan does not help in the diagnosis. Also, important to note that the diagnostic value of family history of axSpA is low when the HLA-B27 status is already known.62 Moreover, IBP is an important feature for referring patients with suspicion of axSpA to the rheumatologist but does not add much diagnostic utility thereafter.63
Conventional radiography of the SIJ is usually used as the first imaging modality to identify the involvement of SIJ, mostly because of feasibility reasons. However, on top of the exposure to radiation, this method has major limitations. Damage in the SIJ only becomes visible in pelvic radiographs several years after the start of the symptoms.64 In addition, the interpretation of radiographs of the SIJ is often challenging even among experienced readers.65 MRI of the SIJ is recommended if the diagnosis cannot be made based on clinical features and conventional radiographs, but yet the clinical suspicion of axSpA remains high (figure 4).

Imaging findings in non-radiographic axial spondyloarthritis. Clinical case: a female patient, 40 years old, complaining of back pain during the last 6 months with inflammatory characteristics (worsening with rest improving with exercise and awaking at second half of night) and morning stiffness of 1 hour. (A) On the pelvis radiograph, no changes are observed; (B) on MRI (fat suppressed sequence) of sacroilliac joints, deep bone marrow oedema suggestive of axial spondyloarthritis on the left sacroiliac bone (both at the sacral margin and iliac bone) is shown.
The presence of BME on MRI of the SIJ fulfilling the ASAS definition increases the likelihood of a diagnosis of axSpA, especially if structural changes are also present. However, clinicians should bear in mind that BME is less specific for axSpA than initially thought.66 BME can also occur in patients with non-specific back pain, osteitis condensans, healthy individuals, postpartum women, recreational runners and athletes (although deep (extensive) lesions are exclusively found in axSpA patients).3 67 Too much reliance on positive imaging findings can easily lead to overdiagnosis and overtreatment.68 Likewise, the absence of inflammation on MRI does not, per se, rules out axSpA. Recent data suggest that in addition to the ‘classical’ axSpA phenotype, dominated by imaging findings, some axSpA patients, mostly women, have a high likelihood of peripheral features co-occurring with CBP but without axial imaging findings.69
MRI of the spine has little diagnostic value on its own, and there is conflicting data on the value of combining MRI of the spine with SIJ for diagnosis.70 Also, abnormalities on spine radiographs do not always occur and when they do it is often too late in the disease course to be of use in early diagnosis. Other imaging modalities, such as skeletal scintigraphy, ultrasonography of the SIJ and positron emission tomography are not recommended for the diagnosis of axSpA.71 The role of (low-dose) CT for diagnosis is yet to be defined.
A major delay of 5–7 years remains between the start of CBP and the diagnosis of axSpA. Despite a similar age of onset, the diagnostic delay is larger in women (mean 8.8 years) than in men (6.5 years).72 Differences in disease presentation, as described above, and physician bias may render the recognition of the SpA-pattern in women more difficult.57 73 In addition, in both genders, too much reliance on the presence of radiographic changes can further delay the diagnosis of axSpA among patients with CBP in primary care. Several referral strategies have been proposed over the years.74 More recently, ASAS has endorsed a screening method for early referral.75 Patients with CBP starting before 45 years of age should be referred to the rheumatologist if ≥1 SpA feature (see next section) is present. The method is flexible to local conditions, such as limited availability of imaging and HLA-B27 typing (which are not mandatory) and can therefore be applied widely.
Classification criteria
Given the limitations of the existing classification criteria in including earlier stages of the disease, the ASAS axSpA criteria were established in 2009 and later implemented in most studies.5 6 76 The ASAS axSpA criteria are applicable to the entire spectrum of the disease (nr-axSpA and r-axSpA) and incorporate MRI of the SIJ.50 The criteria are meant to be applied in patients with CBP and an onset before age 45 years old and have a diagnosis of axSpA. They have two possible entry arms: the ‘imaging arm’ (presence of sacroiliitis on radiography or MRI) and the ‘clinical arm’ (presence of HLA-B27). To classify as axSpA, patients must additionally have at least one (or two, in case of the clinical arm) typical characteristics of SpA, so-called SpA features: IBP, arthritis, enthesitis, dactylitis, uveitis, IBD, psoriasis, good response to NSAIDs, family history of SpA, presence of HLA-B27 and elevated CRP. Their implementation allowed the inclusion in clinical trials of patients covering the entire spectrum of the disease, especially those at an earlier stage, thus representing one of the major advances in the last decade.77 These criteria have shown to perform well against the rheumatologist’s diagnosis, with an overall sensitivity of 82% and specificity of 89%.78
However, the ASAS classification criteria for axSpA are not without criticism. They may lead to overdiagnosis in case they are misused for making a diagnosis. But this is a conceptual error, because similar to all classification criteria, the ASAS criteria should not be used to diagnose patients but to classify patients already diagnosed with axSpA (as described above) in order to be included in a study.79 On the other hand, some experts argue that all features are given the same weight despite not having the same value (LR+ and LR−).80 The main reason for assigning them the same weight was simplicity, favouring implementation. Nevertheless, ASAS in collaboration with SPondyloArthritis Research and Treatment Network is currently conducting a large prospective study, which will re-evaluate the criteria in an international cohort to provide further insight.
Monitoring
Numerous tools are now available to monitor axSpA. As the disease affects deep anatomical structures, it is difficult to make a proper assessment by physical examination. Therefore, most of the tools used in axSpA are based on laboratory or imaging findings and patient-reported outcomes.81 82 Multiple patient-reported outcomes have been developed and validated to determine the disease status and impact. The use of one or the other depends on the disease domain to be explored and the setting (ie, clinical practice or research).83
To assess disease activity in clinical practice, the use of composite indices is preferred.84 Currently, it is recommended to use the Ankylosing Spondylitis Disease Activity Score (ASDAS), which consists of four questions answered by the patient (axial pain, peripheral pain-inflammation, morning stiffness duration and global disease activity) and CRP value in mg/L (using 2 if below the threshold or <2 mg/L).85–87 According to ASDAS, clinicians may classify disease activity as inactive (<1.3), low activity (<2.1), high activity (<3.5) and very high activity (>3.5).86 In addition, clinically important improvement is considered if a decrease between two assessments of at least 1.1 is achieved, and major improvement if the decrease is 2.0. A flare of the disease is defined as an increase in the ASDAS ≥0.9 compared with the previous assessment.88 Additionally, the Bath Ankylosing Spondylitis Disease Activity Index is also available as a valid alternative, preferably in combination with CRP. This is an older index composed of six questions that assesses the first three items of the ASDAS plus fatigue, enthesitis and severity of morning stiffness, ranging between 0 (no disease activity) and 10 (very high disease activity).83 In the past, this index has been used extensively, however, the ASDAS has shown better psychometric properties and it is currently recommended as the preferred index in clinical practice.89 For clinical trials, the instruments to assess disease activity recommended within the ASAS-Outcome Measures in Rheumatology (OMERACT) core set are usually employed.76 Additionally, the ASAS clinical response criteria (ASAS20, ASAS40, ASAS5/6, ASAS partial remission) are commonly used in recent trials.90 The ASAS-OMERACT core set already exists for at least two decades and is currently in an update process.91
It is common for axSpA to affect physical function and spinal mobility. To assess physical function, the Bath Ankylosing Spondylitis Functional Index is recommended, an index composed of 10 questions, with a total score between 0 (good physical function) and 10 (poor physical function).92 To determine mobility impairment, usually the Bath Ankylosing Spondylitis Metrology Index is employed that encompasses several measurements of the axial skeleton.82 93 Recently, the ASAS Health Index has been developed and validated to assess overall functioning and quality of life in patients with axSpA. This index, freely available in 15 languages, encloses 17 items addressing functional limitation in daily activities. A lower score indicates a better health status.94
The CRP and the ESR are the used laboratory parameters to monitor activity in axSpA. These parameters are raised in only 40% of patients with axSpA and therefore, per se, they are only useful in a minority of patients to monitor disease activity.49 As mentioned, MRI can detect inflammatory signs in the SIJs and spine. However, their routine use in clinical practice to monitor axSpA is not recommended, as its additional value compared with more feasible tools remains to be elucidated.71 For research studies, different scores have been developed to quantify inflammation in the SIJ and in the spine, which are frequently used to evaluate treatment response.95–97
If disease activity persists, it results in irreversible structural damage.31 44 The recommended tool for evaluating damage is conventional radiography of the SIJ and spine, but there is no consensus on how to use it for monitoring in clinical practice.71 For research, the modified Stoke Ankylosing Spondylitis Spinal Score is employed for most studies, with a total score ranging from 0 to 72.3 First results of scoring low-dose CT scans of the spine show a promising increase in sensitivity to change.
Burden of the disease
Axial SpA usually begins in the third decade of life, which is a very active period in occupational, social and economic spheres.98 Two thirds of active employed population with axSpA have work-related issues, leading to substantial direct and indirect costs to the society.99 As a consequence, axSpA is associated with a high burden of the disease, which is comparable in patients with r-axSpA and nr-axSpA.100 Older age, lower level of education, longer disease duration, higher disease activity (objective signs of inflammation), reduced physical functioning and employment in more physically demanding jobs are the major determinants of disease burden in axSpA.22 29–31
Management
The primary goal of treatment is to maximise health-related quality of life through control of symptoms and inflammation, prevention of progressive structural damage and preservation/normalisation of function and social participation.101 102 Treatment should be guided through tight control according to a specific target, usually aiming at achieving sustained remission and, if not possible, low disease activity, employing the ASDAS as preferred instrument.89 Importantly, the treatment in axSpA should be based on shared decisions between patients and rheumatologists and includes non-pharmacological and pharmacological therapies (figure 5).

Recommendations to manage axial spondyloarthritis. bDMARDs, biolgical disease-modifying anti-rheumatic drugs; COX-2, cyclooxygenase-2; csDMARDs, conventional synthetic disease-modifying anti-rheumatic drugs; IL-17i, IL-17 inhibitors; JAKi, Janus kinase inhibitors; NSAIDs, non-steroidal anti-inflammatory drugs; r-axSpA, radiographic axial spondyloarthritis; TNFi, tumour necrosis factor inhibitors; tNSAIDs, traditional non-steroidal anti-inflammatory drugs; tsDMARDs, targeted synthetic disease-modifying anti-rheumatic drugs Adapted from van der Heijde et al.101
Non-pharmacological therapies such as physical exercise and physiotherapy are recommended throughout the disease course.101 Recent evidence has evaluated the paradoxical effect of exercise in axSpA.103 On one hand, physical exercise is the cornerstone of treatment as it reduces disease activity and improves spinal function and quality of life. On the other hand, mechanical stress could contribute to inflammation and new bone formation at the entheseal and articular sites.21 Further studies should address this possible paradox, but for the moment it is advisable to encourage patients to regular exercise.
Different types of pharmacological treatment are available for treating axial manifestations of axSpA ((figure 6)).

Evolution of pharmacological drugs available to treat axial spondyloarthritis. The figure shows the date (year) for first time approval of a new type of drug by regulatory agencies (European Medicines Agency or Food and Drug Administration) for radiographic axial spondyloarthritis. bDMARDs, biolgical disease-modifying anti-rheumatic drugs; COX2-inh: cyclooxygenase-2 inhibitor; IL-17i, IL-17 inhibitors; JAKi, Janus kinase inhibitors; NSAIDs, non-steroidal anti-inflammatory drugs; TNFi, tumour necrosis factor inhibitors; tNSAIDs, traditional non-steroidal anti-inflammatory drugs; tsDMARDs: targeted synthetic disease-modifying anti-rheumatic drugs.
The first line are NSAIDs. Both traditional NSAIDs and cyclooxygenase-2 (COX-2)-selective inhibitors in full dose are efficacious in reducing the symptoms and signs of the disease.104 However, drug pharmacokinetics, concomitant manifestations, comorbidities, pregnancy and potential adverse effects must be taken into account.105 106 In patients with concomitant IBD in remission, the use of COX-2 inhibitors for a maximum period of 2 weeks may be preferred over traditional NSAIDs.107 Usually, clinical response to full-dose NSAID is observed within 2 weeks. In case of insufficient response after this period, a second NSAID is recommended. To date, there is insufficient evidence to conclude whether switching between traditional NSAIDs and COX-2 inhibitors is more effective than treatment with a second NSAID of the same class.108 A recent study suggested that switching NSAID classes may be more effective but further studies are needed to confirm these data.109
Biological disease-modifying antirheumatic drugs (bDMARD) are indicated as second-line treatment for axial manifestations. Currently, there are two classes of bDMARDs available: TNFi and IL-17i. bDMARDs are indicated if the target is not achieved after 4 weeks receiving at least two different NSAIDs.110 In addition, patients must have at least one of the following three characteristics to be eligible: an elevated CRP value, inflammation on MRI or radiographic evidence of sacroiliitis.101 TNFi for axSpA are classified into fusion protein (etanercept111 112) and monoclonal antibodies (adalimumab,113 114 certolizumab pegol,115 golimumab116 117 and infliximab118). Among the IL-17i, secukinumab119 120 and ixekizumab121–123 are available. All bDMARDs except infliximab (intravenous) are for subcutaneous administration. Overall, their efficacy in r-axSpA and nr-axSpA is comparable. All above-mentioned bDMARDs are approved by the European Medicines Agency (EMA) and Food and Drug Administration (FDA) for r-axSpA. For nr-axSpA, certolizumab is the only TNFi approved by FDA and EMA, while adalimumab, etanercept and golimumab are only approved by the EMA; infliximab is not approved by any regulator due to lack of data. Secukinumab and ixekizumab are approved for nr-axSpA by both agencies. Another IL-17i under investigation is bimekizumab.124 Both TNFi and IL-17i relief symptoms and signs of the disease, with a good safety profile, but no evidence of superiority of one over the other is available. However, given the greater experience with TNFi, current practice is to start with a TNFi. Furthermore, in case of concomitant uveitis or IBD, a monoclonal antibody TNFi is recommended.101
Other bDMARDs are not effective in treating patients with axSpA. These treatments include abatacept,125 126 IL-6 inhibitors127 128 and IL-12/IL-23 inhibitors.129 In patients with previous TNFi exposure, rituximab does not seem to be effective either. Similarly, there is also no evidence that conventional synthetic DMARDs such as methotrexate, sulfasalazine, leflunomide or hydroxychloroquine are effective for improving axial manifestations and therefore their use is not indicated in patients with purely axial disease.108 Sulfasalazine may be considered in patients with peripheral arthritis. Local injection of glucocorticoids in peripheral (or more rarely in SIJ) may be considered too but the use of long-term treatment with glucocorticoids is not recommended for axSpA.
Recently, targeted synthetic DMARDs (tsDMARDs) against Janus kinase inhibitor (JAKi) have shown to improve axial manifestations in patients with r-axSpA. An advantage of these new therapies is that they are orally administrated. Upadacitinib has been recently approved as the first JAKi for patients with r-axSpA but no data on nr-axSpA are available yet.130 Other tsDMARDs including tofacitinib131 and filgotinib132 have shown to be efficacious in phase II studies. Further approval for new JAKi and for nr-axSpA are expected.
Approximately 60% to 65% of patients achieve clinical response after a first bDMARD.133 Some characteristics (male sex, no smoking, shorter disease duration, elevated CRP and inflammatory lesions on MRI) are associated with a better response (evidence available only for TNFi).37 It is therefore advisable to encourage patients to stop smoking.101 If the clinical response is sustained over time, tapering bDMARD (evidence available only for TNFi) can be considered to minimise side effects and costs. Tapering may be successful but stopping usually result in flares in a large proportion of patients.134 The main factor determining the success of tapering is longer time in remission or low disease activity prior to dose reduction. However, discontinuation of bDMARDs is not recommended, as this leads to disease flare in most patients.135 Nevertheless, if for any reason, such as surgery or pregnancy, discontinuation is temporarily required, evidence supports that the likelihood of achieving a similar response after restarting is very high.136
In case the first bDMARD fails, it is recommended to switch to a second bDMARD, either TNFi or IL-17i. No strategy (switching target or cycling) is preferred but so far, most studies included patients who switched either from a first TNFi to a second/third TNFi or from a TNFi to an IL-17i.119 122 137 Further evidence is required to determine which is the best strategy. In addition, the place of JAKi in the management algorithm needs to be defined.
The effect of different therapies on structural damage progression (assessed by spinal radiographs) in axSpA is controversial. Initial studies showed that continuous administration of NSAIDs could slow the progression of structural damage, especially in patients with syndesmophytes and elevated CRP.138 139 However, another trial has not confirmed these data.140 With TNFi, the opposite was true: pivotal studies did not show inhibition of structural damage while later studies suggest they might have a protective effect, mainly after long-term treatment by controlling disease activity.141–143 But this remains an open question.144 Finally, recent trials with TNFi and IL-17i have shown that only a minority of patients progress in the short term.119 122 However, to date, there is no head-to-head study to compare the results between the different drugs. Future studies are expected to clarify the effect of the different therapies on the progression of structural damage. But in the meantime, causal inference analysis using observational data may contribute to a better understanding of whether disease modification is possible in axSpA.145
Finally, when managing patients with axSpA, it is relevant to consider the ASAS Quality Standards.146 These comprehend an initial and thereafter annual review of all aspects of the disease. This includes assessment of the patients in terms of current disease management, and any further support they may need in the future, in order to maximise health, participation in society and life satisfaction. Focus should not only be on clinical symptoms and severity of disease but also on comorbidities such as cardiovascular risk management or osteoporosis, employment, psychological factors and lifestyle including physical activity. Ideally, this review is performed by a multidisciplinary team under the supervision of a rheumatologist (figure 7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
ASAS quality standards to improve the quality of health and care services for patients with axial spondyloarthritis. Adapted from Kiltz et al.147 ASAS, Assessment in SpondyloArthritis international Society; axSpA, axial spondyloarthritis; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; CRP, C reactive protein; LDL, low disease activity.
Research agenda
In recent years, enormous advances in the understanding and management of axSpA occurred but still relevant unmet needs are to be resolved.147 In the future, further efforts should be made in identifying the disease at an early stage. This starts with increasing the awareness of primary care physicians and other specialists treating patients with CBP. The optimisation of the use of imaging and other biomarkers for early diagnosis is likely to also play a role. A better understanding of the overlap and differences between axSpA and other phenotypes of SpA such as pSpA and psoriatic arthritis should be clarified.
Efforts to further improve the standardisation of instruments to monitor the disease and treatment response are required. In clinical practice, the implementation of more recent developed instruments such as the ASDAS is needed. In addition, the employment of mobile devices to manage the disease should be explored. For research, the updated ASAS-OMERACT core set will consider the new advances.
The development of new drugs against known and new targets is also required to successfully treat those patients who fail to current available drugs. In this sense, the management recommendations should be updated in order to incorporate new drugs, especially JAKi.
Search strategy and selection criteria
Data for this review were identified by searches of MEDLINE, PubMed and references from relevant articles using the search terms “spondyloarthritis” or “ankylosing spondylitis”, and “pathogenesis” or “diagnosis” or “classification” or “treatment” or “management” or “burden” or “work”. Articles published in English until February 2021 were included. We largely selected publications in the past 4 years, but did not exclude commonly referenced and highly regarded older publications. We also searched the reference lists of articles identified by the search strategy and selected those we judged relevant.
Ethics statements
Patient consent for publication
References
Footnotes
VN-C and AS are joint first authors.
Handling editor Josef S Smolen
Contributors All authors were involved in drafting the article or revising it critically for important intellectual content. All authors reviewed the published evidence and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests VN-C has received research grants/honoraria from AbbVie, Janssen, Lilly, Novartis, Pfizer and UCB. AS has received consulting/speaking fees from MSD, UCB, Novartis. BE-Z has received consultancy, research grants and speaker's honoraria from: AbbVie, Amgen, BMS, Eva, Hekma, Janssen, Lilly, MSD, New Bridge, Novartis, Pfizer, Roche, Sanofi‐Aventis and Servier. DvdH reports personal fees from AbbVie, Amgen, Astellas, AstraZeneca, BMS, Boehringer ingelheim, Celgene, Cyxone, Daiichi, Eisai, Eli lilly, Galapagos, Gilead, GlaxosmithKline, Janssen, Merck, Novartis, Pfizer, Regeneron, Roche, Sanofi, Takeda and UCB Pharma, and is Director of imaging Rheumatology BV.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Commissioned; externally peer reviewed.