Article Text

Abstract
Objective: To describe the frequency and duration of remission in the Utrecht rheumatoid arthritis cohort of patients followed since diagnosis, and the clinical and treatment characteristics of patients with remission v those without.
Methods: In 1990 the Utrecht rheumatoid arthritis cohort study group started a clinical trial in which patients with recent onset of rheumatoid arthritis (<1 year) were randomised into four treatment groups: hydroxychloroquine (n = 169); intramuscular gold (n = 163); methotrexate (n = 166); and pyramid (n = 64). After two years, rheumatologists were allowed to prescribe any disease modifying antirheumatic drug. Remission was defined as: duration of morning stiffness ⩽15 min, mean VAS pain ⩽10 mm, Thompson joint score ⩽10, and ESR ⩽30 mm/h during at least six months. Cox regression analysis was used to determine baseline clinical, demographic, and treatment predictors of remission.
Results: Mean follow up duration was 62 months. Thirty six per cent achieved at least one period of remission. Median duration between diagnosis and the first remission period was 15 months for the intramuscular gold group, 18 months for the methotrexate and hydroxychloroquine groups, and 24 months for the pyramid group (NS). Predictors of remission were early response to initial treatment, less pain, rheumatoid factor negativity, and lower joint score at baseline.
Conclusions: After a mean follow up duration of 62 months, only 36% of the patients had fulfilled the remission criteria at least once. A good response to treatment during the first year seems to be independently associated with remission rather than initial treatment alone.
- ACR, American College of Rheumatology
- DMARD, disease modifying antirheumatic drug
- HAQ, health assessment questionnaire
- RF, rheumatoid factor
- VAS, visual analogue scale
- disease modifying antirheumatic drug
- remission
- rheumatoid arthritis
Statistics from Altmetric.com
- ACR, American College of Rheumatology
- DMARD, disease modifying antirheumatic drug
- HAQ, health assessment questionnaire
- RF, rheumatoid factor
- VAS, visual analogue scale
As it is presently not possible to cure rheumatoid arthritis, the aim of current treatment is a reduction in disease activity in the hope of achieving prolonged remission. Remission rates in various studies using the American College of Rheumatology (ACR) remission criteria1 have been estimated to be 15% during two to six years of follow up in patients with early disease,2 18% during 1131 patient–years of follow up,3 20% during five years of follow up in early disease,4 and 18% at 10 years of follow up.5 The period used in the definition of remission in these studies ranged from two3 to six months.4 Other definitions reported are the Magnusson criteria for good response6 and the definition of remission provided by Scott et al.7 The latter was used in the present study.
Even though nowadays most patients are treated with disease modifying antirheumatic drugs (DMARDs) immediately after diagnosis, many patients still do not fulfil the remission criteria, and certainly not for a prolonged period. In various studies, several clinical and demographic variables have been associated with remission, such as absence of rheumatoid factor (RF),4,8 male sex,9 fewer tender or swollen joints,4 and age of onset over 65 years.8 Functional disability—associated with disease activity early in the course of the disease and with both disease activity and radiological outcome later on10—was not found to be a predictor of remission after two or 10 years of disease.5,11 Remission might not only be dependent on baseline characteristics and initial treatment, but also on the treatment prescribed during follow up. It would therefore be of interest not only to determine baseline predictors of remission but also to evaluate treatment strategies just before remission.
In this report we describe the frequency and duration of remission among patients participating in the Utrecht rheumatoid arthritis cohort. We investigated which baseline clinical, demographic, and treatment variables were possible predictors of remission and we describe the treatment before remission.
METHODS
From 1990 to 1998 all patients with recent onset of rheumatoid arthritis (less than one year) from six rheumatology outpatient clinics in the Utrecht region of the Netherlands were asked to participate in a randomised prospective clinical trial. All patients fulfilled the 1987 ACR criteria for rheumatoid arthritis.12
Treatment
Patients were randomly assigned to the pyramid strategy group or to one of the three early DMARD strategy groups. All randomisation procedures were done by drawing sealed envelopes from blocks of 100 with equal numbers of patients for each of the four treatment groups per hospital. Patients in the pyramid group were treated with non-steroidal anti-inflammatory drugs (NSAIDs), and the administration of DMARDs was started only if NSAIDs alone were clinically not effective enough after one year of treatment. After 1994 no further patients were allocated to the pyramid group because planned interim analysis showed that clinical efficacy after one year was significantly greater for the early DMARD strategy groups than for the pyramid group,13 making it unethical in our view to withhold treatment with DMARDs from the time of diagnosis in rheumatoid arthritis.
The three early DMARD strategy groups to which patients were randomly assigned were as follows:
-
hydroxychloroquine group: treatment was started with hydroxychloroquine (400 mg/day), if necessary replaced by auranofin (6–9 mg/d);
-
intramuscular gold group: intramuscular (im) gold (50 mg/week), if necessary replaced by D-penicillamine (500–750 mg/d);
-
methotrexate group: oral methotrexate (7.5–15 mg/wk), if necessary replaced by sulphasalazine (2000–3000 mg/d).
Good response to the initially allocated DMARD was assessed one year after study start and was defined as more than 50% improvement from baseline in at least three of the following four disease indices: visual analogue scale (VAS) pain (mm), Thompson joint score (a weighted joint score including both swollen and tender joint count14,15), morning stiffness (min), and erythrocyte sedimentation rate (ESR) (mm/h). If patients met the criteria of good response, the primary DMARD was continued. Otherwise the initial DMARD was stopped and treatment with the second DMARD was given according to the protocol. This second DMARD was then continued until two years after inclusion. Dosage of DMARDs was reduced or stopped if patients were having a complete response. After two years, the policy for treatment was free. The use of NSAIDs and analgesics was allowed in all strategies. Oral glucocorticoids and intra-articular injections were avoided as far as possible.
Clinical variables were assessed by a clinician at the start of the study and every three months thereafter during the first two years, and then once every six months. The clinical variables were ESR, VAS general wellbeing, VAS pain, Thompson joint score, functional disability (health assessment questionnaire (HAQ), Dutch version16), and grip strength (based on the mean of three measurements in each hand using a vigorimeter). If clinical data were missing, the mean of the previous and subsequent scores was used. Rheumatoid factor status was determined at baseline and once every year thereafter, by either the latex fixation or the Rose-Waaler test (⩾20 IU/ml). Radiographs of hands and feet were taken at baseline and once a year and scored according to the modified Sharp/van der Heijde method.17 If no radiological data were available for the last visit, the missing score was imputed by using the slope of radiological progression of the previous years. We believe that this method is valid, because a linear progression was found in a previous report that included this cohort of patients with rheumatoid arthritis.18
Definitions of remission, flare, and improvement
Remission was defined according to our adaptation of the remission definition of Scott et al,7 which was developed to evaluate the response to DMARDs more appropriately. In the present study, patients were considered to be in remission when the duration of morning stiffness was ⩽15 minutes, VAS pain was ⩽10 mm, Thompson joint score was ⩽10, and ESR was ⩽30 mm/h. Patients had to fulfil these criteria for at least six months—that is, three subsequent visits during the first two years or two subsequent visits after two years. The design of our study committed us to include the Thompson score as a substitute for the tender and swollen joint count. Additional differences between our definition and that of Scott are that we included <10 mm of pain instead of no pain, and that the criteria had to be fulfilled for at least six months. Patients who no longer fulfilled the remission criteria during assessment were considered to have a flare at that time.
Next to remission, we calculated the number of patients with clinical improvement from baseline, using a modification of the ACR20 criteria: a reduction of at least 20% from baseline in the Thompson joint score and an improvement of at least 20% from baseline in at least two of the following four variables: patients’ assessment of pain (VAS), patients’ assessment of general wellbeing (VAS), patients’ assessment of physical function (HAQ), and ESR.
Four years of follow up
To compare clinical and radiographic changes between patients with at least one period of remission and those without remission, and to identify baseline predictors of remission, we evaluated the patients for whom four year follow up data were available. For each treatment group separately, we evaluated whether patients were responders at one year by using the similar definition for a good response as described above. After one year, the number of responders with remission during the subsequent three years was compared with number of non-responders with remission.
Statistical analyses
Differences in median duration until the first period of remission across the three treatment strategies were tested for statistical significance using the Kruskall–Wallis test (p<0.05).
After four years, mean (SD) and median changes from baseline were calculated for all variables. Differences between groups were tested by the unpaired two sided t test for normal distribution of data or the Mann–Whitney U test for non-normal distribution of data, where appropriate. Cox logistic regression analysis was used to determine baseline predictors of remission up to four years of follow up (stepwise procedure).
Differences in the number of responders with remission and the number of non-responders with remission at one year were tested for statistical significance using the χ2 test. All calculations were done using SPSS 9.0 software.
RESULTS
This study included 562 patients with rheumatoid arthritis (70% women), whose mean (SD) age was 56 (14) years at the start of the study. Baseline characteristics did not differ between the four treatment strategy groups (table 1). Mean follow up duration until the time of withdrawal or until the last follow up visit available for the total study population was 62 (24) months (range 12 to 96 months). Of the 562 patients included in the study, 144 dropped out during follow up. Causes of drop out were: death (42), moved out of the area (11), other diseases which made adherence to the cohort impossible (15), long lag time between this study and the last outpatient visit (33), in remission or with low disease activity (13), and otherwise, or reason unknown (30).
Baseline demographic characteristics, clinical characteristics, and changes in treatment over time for each of the four treatment groups
Remission, flare, and improvement
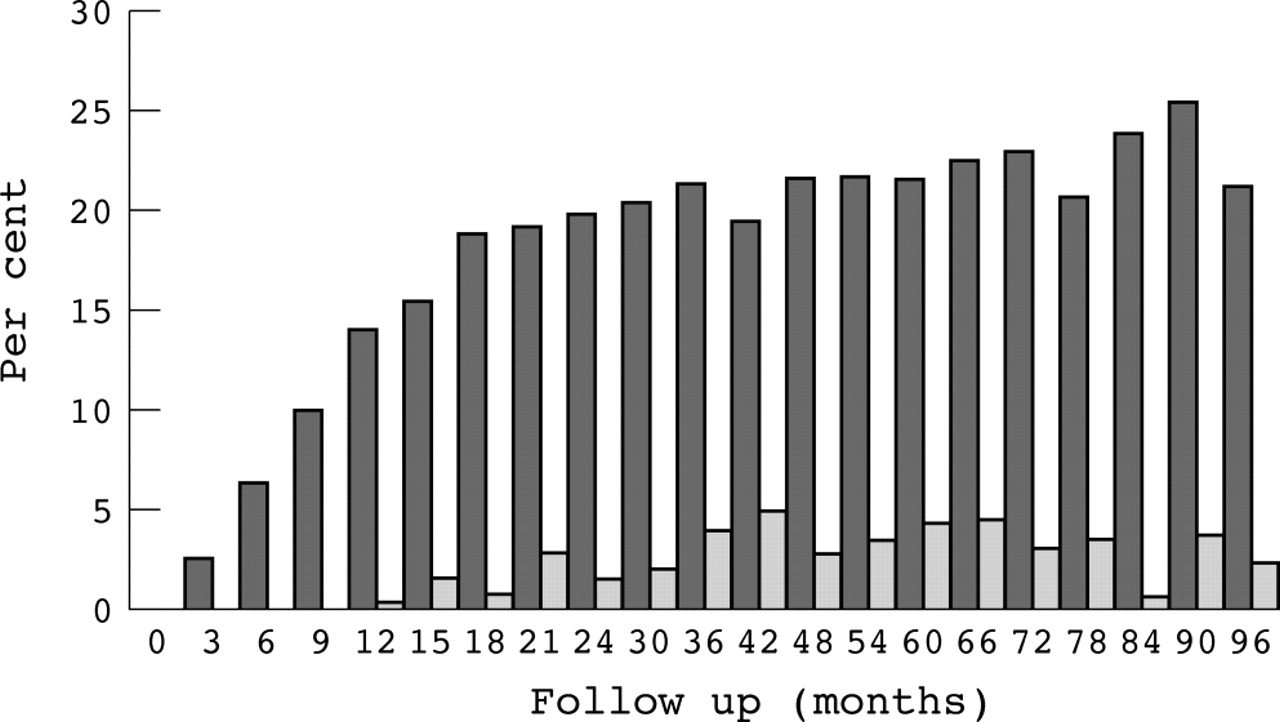
In all, 205 patients (36%) achieved at least one period of remission during follow up (57 patients had a second and eight patients a third period of remission). Mean cumulative duration of all remission periods was 25 (19) months (range 6 to 87), comprising 39 (25)% of total follow up time. Mean duration from study start until the first period of remission was 24 (19) months. Figure 1 shows the percentage of patients in remission and the percentage of patients having a flare at each assessment point. Of the 270 remission periods, 158 were followed by a flare; for 112 periods the data were the last available data at time of evaluation of this study (n = 84), or were the last data because patients dropped out of the study or for various other reasons (n = 28).
{kind=link}
Percentage of patients in remission (dark columns) and percentage with a flare (light columns) at each assessment point. Remission: duration of morning stiffness ⩽15 min, mean VAS pain ⩽10 min, Thompson joint score ⩽10, ESR ⩽30 mm/h for at least six months. Flare: not in remission at that specific assessment point.
Mean values of the following baseline characteristics were significantly worse for patients without a period of remission than for those with a period of remission: morning stiffness (120 v 94), VAS general wellbeing (53 v 42), grip strength (28 v 36), Thompson joint score (157 v 128), VAS pain (52 v 36), and HAQ (1.4 v 1.1). The percentage of patients with absent rheumatoid factor at baseline was significantly higher among patients with remission than in those without (45% v 29%). Age (56 v 57), ESR (43 v 39), and radiographic damage (3.9 v 4.8) did not differ significantly between the two groups. In addition, the area under the curve standardised to time for all clinical variables was significantly worse for the non-remission group than for the remission group (mean scores: ESR, 27 v 16; morning stiffness, 65 v 18; VAS general wellbeing, 40 v 18; grip strength, 34 v 56; Thompson joint score, 70 v 23; VAS pain, 32 v 9; functional disability, 1.30 v 0.62).
The percentage of patients in remission during follow up was not significantly different (p = 0.28) between the four treatment strategy groups: 42% in the im gold group, 36% in the methotrexate group, 31% in the hydroxychloroquine group, and 38% in the pyramid group. Although not statistically significant, the median time until the first remission period tended to differ between the four assigned treatment strategy groups (p = 0.078). Mean (SD) time until the first remission for the im gold group was 21 (17) months (median 15), v 24 (19) months for the methotrexate group (median 18), 24 (19) months for the hydroxychloroquine group (median 18), and 33 (23) months for the pyramid group (median 24).
In all, 16 patients (8%) did not receive any DMARD during the six months before their first period of remission. The numbers (%) of patients receiving each specific DMARD before remission were: im gold, 55 (27%); methotrexate, 70 (34%); hydroxychloroquine, 42 (21%); D-penicillamine, 5 (2%); sulphasalazine, 8 (4%); auranofin, 1 (<1%); azathioprine, 1 (<1%); and combinations of DMARDs, 7 (3%). In the overall study population, 99% of the patients used NSAIDs, 22% used prednisone or dexamethasone, and 57% received an intra-articular injection during follow up. In the remission group, eight patients (4%) received prednisone or dexamethasone in the period between the first visit of the remission period and the previous visit, and 19 patients (9%) received at least one intra-articular injection at the visit prior to the remission period.
Clinical improvement from baseline to one year was achieved by 64% patients in the im gold group, 71% in the methotrexate group, 59% in the hydroxychloroquine group, and 47% in the pyramid group (p = 0.005). Thereafter, a significant difference in the number of patients with clinical improvement at predefined assessment points from baseline (p<0.05) was observed between the initial four treatment groups at 15 months (73%, 75%, 59%, and 54% of the patients, respectively), 18 months (74%, 71%, 57%, and 55%), 21 months (72%, 75%, 66%, and 57%), 48 months (76%, 77%, 74%, and 56%), and 60 months (75%, 72%, 68%, and 64%). At other time points no significant differences were found in the number of patients with improvement from baseline.
Four years of follow up
Data on 425 patients with rheumatoid arthritis were available at four years (table 2). At least one period of remission was achieved in 142 patients (33%). Patients who were in remission during the first four years of their disease had a more favourable disease course with respect to all measured variables than those who were not, irrespective whether these variables were part of the remission definition or not (table 3).
Baseline characteristics of patients with remission and patients without remission during four years follow up.
Change from baseline after four years of variables either included in or not included in the definition of remission for the group of patients achieving at least one period of remission and the group without remission within four years of disease onset
Considering each treatment strategy separately, treatment responders (>50% improvement on three of four variables) at the one year follow up were compared with non-responders. Baseline values did not differ between the responder group and the non-responder group, except for age and ESR in the methotrexate group. In the group of patients who received im gold at baseline, 55% of the responders (n = 67) and 16% of the non-responders (n = 57) were in remission at some assessment point in the subsequent three years (p<0.001). In the methotrexate group these percentages were 51% of 63 patients and 13% of 60 patients (p<0.001), respectively; in the hydroxychloroquine group, they were 52% of 48 patients and 18% of 78 patients (p<0.0001), and in the pyramid group they were 67% of 15 and 19% of 37 patients (p<0.001). This indicates that despite similar baseline characteristics and similar treatment, patients are more likely to achieve remission when they were defined as responders at one year, as one would expect.
For determining predictors of remission, complete baseline data were available on 397 patients. Baseline predictors of remission were a good response to treatment, less pain, absence of rheumatoid factor, and lower joint score (table 4).
Baseline predictors of remission during four years of follow up using Cox regression analysis
DISCUSSION
In this cohort of patients with rheumatoid arthritis followed since diagnosis, we show that 36% of 562 patients achieved at least one period of remission during follow up and that patients were in remission for 39% of their follow up time. The latter percentage is slightly higher than found in the study by Eberhardt and Fex,4 where 62% of the patients received DMARDs and the patients remained in remission for approximately one third of their follow up time; however, these investigators used the ACR criteria for remission. In other studies using the ACR remission criteria, or a modified version of it, the percentage of patients in remission has ranged from 15% to 20%.2–5 The higher remission rate of 36% in our study might partly be explained by the difference in the definition of remission, along with differences in study design and duration of follow up. For reasons of protocol, we used a revised definition of remission, as proposed by Scott et al,7 in which we had to include the Thompson joint score. The Thompson joint score has, however, been proven to be of similar value to other joint counts in measuring disease activity.19
Although the patients followed in this study were participating in a randomised clinical trial during the first two years after disease onset, we believe they were representative of the general rheumatoid arthritis population attending outpatient clinics, because all patients with recent onset of disease and visiting one of the participating hospitals were asked to participate. Moreover, while the baseline values of the patients who did not wish to be randomised tended to be slightly better than in the study groups, the difference was not significant except for the laboratory variables.13
The values for the percentage of remission over time and the duration of remission relative to the follow up time suggest that remission does not persist for a prolonged period. It has been found that patients in remission who continue to receive second line drug therapy have a lower cumulative incidence of flares (22%) than patients who continue to receive placebo (38%),20 and this, together with our results, indicates that it would be better to continue treatment for a while when patients are in remission.
Interestingly, patients who received im gold at study onset had a shorter delay until the first remission period compared with methotrexate (15 v 18 months), though it is generally thought that gold is slower to act than methotrexate. An explanation might be that the percentage of patients receiving im gold who were then changed to the second DMARD because of adverse events was greater than the percentage receiving methotrexate, and that the time to change of medication was shorter for the im gold group. This has also been observed in other studies.21–23 Overall, the percentage of patients remaining in remission was much lower than the target figure for treating rheumatoid arthritis. Biological agents are now available and their initial efficacy appears very promising.24–28 However, treatment strategies with conventional DMARDs can be improved considerably (for example with higher doses of methotrexate, up to 30 mg/week, which has greater efficacy). Furthermore, conventional DMARDs probably remain the rheumatologists’ first choice because of the lack of availability of biological agents in certain countries and their high cost.
In this study, remission was more likely to occur in patients with a good response to the initial treatment strategy, in those who were initially rheumatoid factor negative, and in those with less pain and a lower joint count at baseline. In several other studies the absence of rheumatoid factor was also found to be associated with an increased probability of remission,4,8 while rheumatoid factor positivity is associated with radiological damage.29–31 Not many studies have estimated the influence of treatment as an independent predictor of remission. In a two year follow up study comparing combination therapy with single drug therapy, the combination treatment regimen was found to be the only variable predicting remission after two years.32
Although time until the first remission period tended to differ between the four assigned treatment groups at baseline, the kind of DMARD at baseline did not predict remission. We did find that the frequency of remission after one year was significantly higher among responders than among the non-responders.
Conclusions
After a mean follow up duration of 62 months, only 36% of the patients had fulfilled the remission criteria at least once. Good response to treatment, less pain, a negative rheumatoid factor test, and a lower joint count at baseline were predictors of remission, but not the allocated first drug. It thus seems that a good response to treatment during the first year is linked to the likelihood of going into remission rather than to the type of initial treatment given. This suggests that treatment should be tailored to the individual patient and that we should aim for a rapid response using aggressive treatment strategies such as higher doses of methotrexate.
REFERENCES
Footnotes
-
We would like to thank all the other participating rheumatologists of the Utrecht Rheumatoid Arthritis Cohort study group; C van Booma-Frankfort (Diakonessenhuis, Utrecht), E J ter Borg (Antonius Hospital, Nieuwegein), A H M Heurkens (Meander Medical Centre, Amersfoort), D M Hofman (Hilversum Hospital, Hilversum), A A Kruize (UMC Utrecht, Utrecht), M J van der Veen (St Jansdal, Harderwijk), and C M Verhoef (Flevo hospital, Almere), Netherlands.
This study was supported by a grant from The Dutch Arthritis Association