Article Text

Abstract
Objective: To elaborate a clinical practice decision tree for the choice of the first disease modifying antirheumatic drug (DMARD) for untreated rheumatoid arthritis of less than six months’ duration.
Methods: Four steps were employed: (1) review of published reports on DMARD efficacy against rheumatoid arthritis; (2) inventory of the information available to guide DMARD choice; (3) selection of the most pertinent information by 12 experts using a Delphi method; and (4) choice of DMARDs in 12 clinical situations defined by items selected in step 3 (28 joint disease activity score (DAS 28): ⩽3.2; >3.2 and ⩽5.1; >5.1; rheumatoid factor status (positive/negative); structural damage (with/without)—that is, 3×2×2). Thus, multiplied by all the possible treatment pairs, 180 scenarios were obtained and presented to 36 experts, who ranked treatment choices according to the Thurstone pairwise method.
Results: Among the 77 items identified, 41 were selected as pertinent to guide the DMARD choice. They were reorganised into five domains: rheumatoid arthritis activity, factors predictive of structural damage; patient characteristics; DMARD characteristics; physician characteristics. In the majority of situations, the two top ranking DMARD choices were methotrexate and leflunomide. Etanercept was an alternative for these agents when high disease activity was associated with poor structural prognosis and rheumatoid factor positivity.
Conclusions: Starting with simple scenarios and using the pairwise method, a clinical decision tree could be devised for the choice of the first DMARD to treat very early rheumatoid arthritis.
- DAS 28, 28 joint disease activity score
- DMARD, disease modifying antirheumatic drug
- decision tree
- early rheumatoid arthritis
- DMARD choice
Statistics from Altmetric.com
Rheumatoid arthritis is the most common form of chronic inflammatory rheumatism.1,2 This disease of unknown autoimmune origin evolves by flares that usually lead to the destruction of joints, functional disability, deterioration of the quality of life, and even shortened life expectancy. Because of its frequency, its socioprofessional repercussions, and the increasing cost of its management—especially since the advent of biological agents, rheumatoid arthritis represents a real public health problem.
It has now been well established that early treatment with disease modifying antirheumatic drugs (DMARDs) should be initiated to control the inflammatory activity and slow the structural damage.3 This treatment, if it is adapted, can have a favourable impact on the evolution of the disease.4,5 Unfortunately, very little information is available on the efficacy of DMARDs in very early rheumatoid arthritis. In addition, no guidelines have established the precise information to be taken into account to help orient the clinician’s choice of the first DMARD to be prescribed for early rheumatoid arthritis. Notably, in the rare publications on this topic, disease activity was usually the only factor considered.6 Practical recommendations are also lacking on the type of DMARD to be prescribed when taking these variables into account in very early disease.
On behalf of the French Society of Rheumatology, the Working Group for Therapeutic Strategies for Rheumatoid Arthritis (Stratégies Thérapeutiques de la Polyarthrite Rhumatoïde (STPR)) decided to devise a decision tree in the form of a practical guide to the choice of the first DMARD to be prescribed for rheumatoid arthritis of less than six months’ duration.
METHODS
This endeavour was conducted in four successive steps: (1) a critical review of published reports on the efficacy of DMARDs against rheumatoid arthritis activity and structural damage; (2) an inventory as full as possible of all factors that might contribute to the optimal DMARD choice; (3) selection, among the collected items, of the most relevant to orient, in routine practice, this choice; and (4) the development of a practical decision tree, taking into account the information selected above.
The STPR Working Group is composed of 13 French Society of Rheumatology members, from 13 different rheumatology units of French university hospitals, who are experts in the management of rheumatoid arthritis, based on their research and clinical experience; 12 of them were recruited for their clinical expertise and the 13th (FG) for his methodological expertise.
We concentrated our efforts exclusively on very early rheumatoid arthritis, defined as present for less than six months, with a definitive diagnosis and still untreated with DMARD or corticosteroids, but a non-steroidal anti-inflammatory drug could have been given.
Step 1, the literature review, was conducted by the STPR experts according to evidence based medicine methodology; its detailed methodology7 and the results obtained have already been published.8 This literature review focused on recent onset rheumatoid arthritis, taking into consideration DMARD efficacy against disease activity and structural damage. In parallel, we took into account the very recent reviews on factors predictive of structural damage.9,10
During step 2, the STPR experts were asked to list all the information concerning the patient that might be considered in the choice of a first DMARD. Because it had been established a priori that the diagnosis of rheumatoid arthritis was definitive, they were asked not to retain any item having only diagnostic value. Experts were asked to propose only items available at the time of diagnosis. To constitute a definitive inventory of candidate items, the list was submitted to 132 French community rheumatologists during a continuing education course.
During step 3, only the 12 STPR expert physicians were asked to select from this inventory those items that they consider pertinent in daily practice to guide the choice of the first DMARD for very early rheumatoid arthritis. This selection was made using the Delphi method.11 From the onset, the threshold for selection for an item was set at 70% concordant opinions. These experts then organised the selected items into five domains.
During step 4, the final choice of DMARDs was made among the six candidate treatments selected as potentially effective and licensed for use in early rheumatoid arthritis: gold salts, sulfasalazine, methotrexate, hydroxychloroquine, leflunomide, and etanercept (at the time of the study, February 2004, other biological agents had not yet been indicated for first line therapy). Experts were told that the dosage was given according to the national recommendations, with the possibility of increasing it up to the maximum permitted and tolerated level. Because all possible combinations could not be tested, we arbitrarily decided to consider only monotherapies. Moreover, the experts were instructed not to consider the cost of the DMARDs. A panel of 36 experts from the 12 cities, including the 12 STRP Working Group experts and 24 practising rheumatologists (see the appendix), chose treatment options according to the Thurstone pairwise method.12 Combining the three items selected in step 3 (28 joint disease activity score (DAS 28), ⩽3.2, >3.2 and ⩽5.1 or >5.1), rheumatoid factor (positive/negative), and structural damage (with/without)—that is, 3×2×2) created 12 potential clinical situations, which were then multiplied by the 15 potential treatment pairs, yielding 180 scenarios (collected in a spiral notebook). A well trained research nurse then presented the scenarios individually to each member of the expert panel, thereby assuring that no question was missed or went unanswered. Each expert then chose the optimal first line agent out of the pair of DMARDs offered to be prescribed in each scenario presented. This study was done under the sole responsibility of the STPR working group on behalf of the French Society of Rheumatology. Financial support was given by the Club Rhumatismes et Inflammation (CRI), a non-profit organisation.
Statistical analysis
For each of the 12 clinical situations in step 4, treatment possibilities were ranked by frequency of choice. The two top ranking treatments chosen for each clinical situation were used to construct a decision tree for the selection of the first DMARD to treat early rheumatoid arthritis. This was conducted by first running a hierarchical classification procedure to identify the hierarchy of scenario variables—that is, three items selected in step 3, influencing the choice; and second, applying correspondence factor analysis to determine the most frequent associations of alternative DMARDs to treat the clinical scenarios presented. Expert panel characteristics (age, sex, period of training, position—that is, public, private or both) were introduced as supplementary variables into the correspondence factor analysis to search for association with treatment options, and analysis of variance (ANOVA) was used to search and test for their potential impact on determining choices.
All analyses were conducted using SAS® 8.2 software.
RESULTS
A summary of the literature review on the efficacy of DMARDs against rheumatoid arthritis activity and structural damage—taking into consideration the duration of the disease and the level of evidence, as recommended by Shekelle et al7—is given in table 1⇓. The published findings8 were updated in November 2003 just before starting step 4 (February 2004). No study had demonstrated with a high level of evidence the efficacy of any of the agents tested alone against rheumatoid arthritis of less than six months’ duration. Recent reviews devoted to the search for factors predictive of structural damage indicated the principal items usually identified: the initial presence of structural damage, rheumatoid factor positivity, and a raised erythrocyte sedimentation rate (ESR) or C reactive protein concentration, or both.
Efficacy of disease modifying antirheumatic drugs against rheumatoid arthritis activity and structural involvement as a function of disease duration, as assessed in November 2003
During step 2, the inventory of information that might contribute to guiding the DMARD choice identified 75 items. The 132 community rheumatologists added two and they retained 77 items.
At the end of step 3, the 36 members of the expert panel had retained only 41 (53%) of the 77 items, according to the Delphi method, as being pertinent for the orientation of the DMARD choice. The items were then organised by consensus into five domains (table 2⇓): rheumatoid arthritis activity, factors predictive of structural damage, patient characteristics, DMARD characteristics, and physician characteristics. In domains I and II, respectively, disease activity is defined by simple items that characterise the actual status of the patient’s disease, while the prognostic factors concern data that might be able to predict later structural status. To characterise disease activity, we used the DAS 28 with four variables and three levels of activity. This composite index takes into account several items selected during step 3: number of painful joints, number of swollen joints, and severity, as assessed by ESR or C reactive protein, or both. Actual structural damage (yes/no) and rheumatoid factor positivity (yes/no) were retained as factors predictive of structural damage; ESR and C reactive protein were not used because they are items included in the DAS 28.9,10 DAS 28 and factors predictive of structural damage can thus be used to construct a decision tree. Domains II, IV, and V—characteristics of patients, DMARDs, and physicians—contain items that constitute the uniqueness of these three “actors” in every medical consultation. The items included in these three domains vary widely according to the clinical situation and thus cannot be taken into account in the construction of a decision tree to be applied to all patients.
Reorganisation of the items selected by the 12 experts into five domains
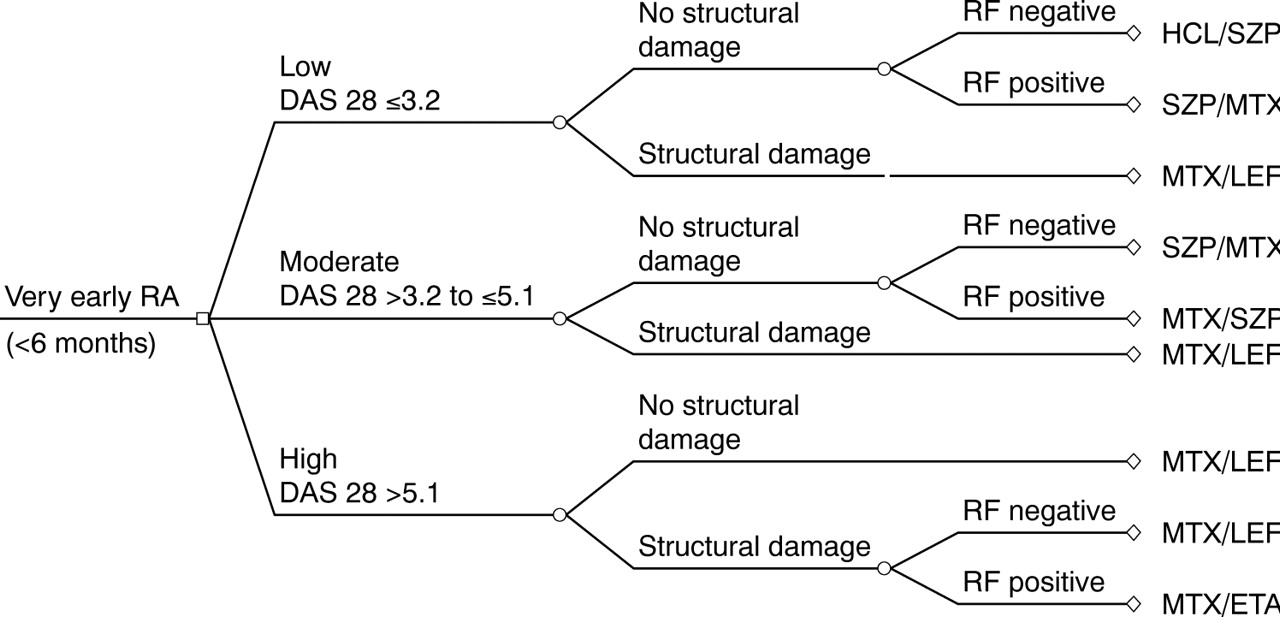
During step 4, the final choice of DMARD was made as described above; the two top ranking choices for the first DMARD are presented in table 3⇓. Pertinently, the percentages of expert preferences were very similar. Finally, the decision tree was developed for the choice of DMARD (fig 1⇓), according to the results of hierarchical classification. Schematically, in the majority of cases methotrexate and leflunomide were the first line treatments of choice. Sulfasalazine was prescribed only in the absence of structural damage, when activity was low or moderate, and hydroxychloroquine became the treatment of choice in the less severe context, when activity was low and structural damage and rheumatoid factor were absent. At the other end of the spectrum, when the clinical picture was severe—associating high disease activity, structural damage, and rheumatoid factor positivity—etanercept was the second choice, methotrexate being the first.
The two top ranking choices, expressed as percentages, of the first disease modifying antirheumatic drug selected by the 36 members of the expert panel for very early rheumatoid arthritis

{kind=link}
Decision tree for the choice of the first disease modifying antirheumatic drug for very early rheumatoid arthritis based on the expert panel’s two top ranking choices. DAS 28, 28 joint disease activity score; ETA, etanercept; HCL, hydroxychloroquine; LEF, leflunomide; MTX, methotrexate; RA, rheumatoid arthritis; RF, rheumatoid factor; SZP, sulfasalazine.
According to our multivariate analyses, none of these drug choices was influenced by the characteristics of the expert panel: sex, age, type of practice, and period of training.
DISCUSSION
This endeavour enabled us to develop guidelines, in the form of a simple decision tree, to be applied in clinical practice to select the first DMARD for the treatment of very early rheumatoid arthritis. These recommendations exclusively address untreated, definitively diagnosed rheumatoid arthritis; they do not concern the relatively frequent situation of an inflammatory rheumatism for which a diagnosis of rheumatoid arthritis cannot be confirmed. Because no published study has shown, with a high level of evidence, the efficacy of any DMARD against the activity or structural damage of rheumatoid arthritis of less than six months’ duration,8 the advice of experts is avidly awaited.
We were able to identify 77 items and retained 41 able to orient the choice of a DMARD for definitively diagnosed untreated very early rheumatoid arthritis. To the best of our knowledge, this undertaking has never been attempted before. Notably, no single expert established the entire list of these items alone. This list was then completed and retained by 132 practising rheumatologists experienced in the management of rheumatoid arthritis.
These items were easily reorganised into five domains. Domain I, disease activity, contains the principal items described in published reports on this subject: the four comprising the DAS 2813 and the seven American College of Rheumatology criteria defining rheumatoid arthritis.14 Also taken into consideration were items pertinent to the management of rheumatoid patients individually: morning stiffness and night time wakening. Domain II, which concerns the prediction of structural damage, contains the three elements identified in the greater majority of studies conducted on cohorts of patients with early rheumatoid arthritis or inflammatory rheumatisms10,15–,18: initial structural damage, rheumatoid factor status, and biological inflammatory syndrome. The presence of anti-cyclic citrulline peptide antibodies was not retained because the results were still contradictory at the time step 4 was completed. The heading “Patient characteristics” covers several expected items—that is, medical history, age, and comorbidities, in addition to others more recently identified that are gaining importance in the choice of the DMARD to be prescribed: acceptance of the regimen and its risks, willingness of the patient to submit to regular monitoring of treatment tolerance, and so on. Wolfe et al recently underlined this determinant role of the patient’s wishes in the USA.19 Concerning the characteristics of the drugs to be given, the experts did not retain direct or indirect costs, as they were instructed not to consider economic factors. Finally, among the characteristics of the treating physician, only experience was retained.
Among these five domains, we found only domains I and II—disease activity and prediction of structural damage—to be pertinent for the development of guidelines in the form of a decision tree. Indeed, the three others vary in each clinical situation and thus cannot be applied. For activity, the DAS 28 with four variables was chosen because of its properties (facility of assessing these traits) and the ability to distinguish three levels of activity.13 As regards the prognosis, the choice was much more difficult because no publications are available on community recruited patients with rheumatoid arthritis of less than six months’ duration, untreated, and followed for sufficiently long periods to advance a prediction of structural damage for each patient. Analysis of the rare cohorts satisfying these conditions showed that, in the best of cases, only 80% of the patients were correctly classified.10,15–,18 Despite these difficulties, we thought it imperative to consider factors predictive of structural damage because agents acting on this manifestation, notably biological agents, will henceforth be available.8 The results of studies on very recent onset rheumatoid arthritis allow us to hope that new prognostic markers, applicable individually to each patient, will be identified.20–,22 After considering the published data, we retained the factors predictive of structural damage most frequently cited in published reports: the initial presence of structural damage and rheumatoid factor status. The presence of a biological inflammatory syndrome was not retained because it is one of the DAS 28 variables chosen to define activity and it was inconsistently identified as a prognostic factor when the judgment criterion was structural damage.9,10
Short clinical scenarios describing disease activity and structural prognosis were presented individually to the members of the expert panel. Each scenario was intentionally not detailed, so as to correspond to a wide variety of real clinical situations. For each scenario, the expert was asked to choose between two treatments. Experts were sometimes reluctant to opt for one or other when they felt that the treatments proposed were not consistent with regard to the clinical scenario. The visiting nurse explicitly requested that they exclude the worst option, and thereby provide an answer and avoid missing data. Because experts found themselves confronted with this inconsistent treatment priority for only a limited number of scenarios, these choices were indeed counted but they ranked low among the various options and had no chance of being retained in the final decision tree.
The decision tree proposed is easy to use. It takes into consideration basic items: DAS 28, initial structural damage, and rheumatoid factor status. The therapeutic options proposed are user-friendly: for most cases, methotrexate was the first choice, followed closely by leflunomide, especially when structural damage was already present initially. It should be kept in mind that we considered only DMARD monotherapy. Furthermore, to the best of our knowledge, DMARD combinations have never been tested for treating rheumatoid arthritis of less than six months’ duration.
When activity was low without structural damage or rheumatoid factor, hydroxychloroquine was the first line treatment of choice; however, it is true that, in this scenario, the diagnosis of rheumatoid arthritis is rarely certain. Thus in the real life the choice can be difficult. On the other hand, when all the indicators were pejorative, a biological agent, etanercept, was recommended as second choice. When this decision tree was developed, that drug was the only biological agent authorised without prior methotrexate treatment in France. To the best of our knowledge this is the first time that recommendations for DMARD use in very early rheumatoid arthritis have been presented as an easy to apply decision tree. The only recommendations that have been published are those of the American College of Rheumatology which were last updated in 2002.6 The latter comprise a complete review of the objectives and means available to control rheumatoid arthritis, but they do not attribute the respective place of each of the DMARD as a function of activity and prediction of structural damage. The guidelines of the Scottish Society of Rheumatology, available on the Internet, are not presented as a decision tree.23 Smolen et al recently devised an algorithm intended to control rheumatoid arthritis as much as possible, especially at its onset.24 Methotrexate was systematically recommended at rapidly increasing doses, regardless of the disease activity or prediction of structural damage. We plan to re-evaluate these guidelines as a function of the progress made concerning DMARDs and of improved understanding of prognostic factors and even better definition of rheumatoid arthritis activity. In that way, we will consider anti-cyclic citrulline peptide antibodies as a variable. Considering the recent evidence of inducing remission,25 especially in early disease, we will modify the wording of the questions asked to the experts when we update these recommendations. Finally, we will continue to develop this decision tree for rheumatoid arthritis of longer duration.
APPENDIX
The 24 other members of the expert panel are: J Allain, B Auge, C Collanges, A Constantin, A Daragon, J F De Person, J Debrock, V Desmas, P Dieudé, S Jousse, M A Lecrosnier, M C Legouffe, A Lhose, D Loeuille, D Malaizier, Y Maugars, R Mistrih, J Morel, E Palazzo, C Piroth, F Pouyol, S Rozenberg, E Solau Gervais, and O Vittecoq.
Acknowledgments
The Clinical Epidemiology Centre, Inserm (Institut National de la Santé et de la Recherche Médicale), Health Ministry, Nancy University Hospital, helped with data analysis. A grant to finance the logistics of the study was obtained from Laboratoire Aventis, Paris, France. We thank Janet Jacobson for editorial assistance.
REFERENCES
Footnotes
Published Online First 30 June 2005