Article Text

Abstract
Background: Permanent visual loss (PVL) is the most feared complication of giant cell arteritis (GCA), and its risk factors are still unclear.
Objectives: The aim of our study was to assess the pathological features predictive of PVL on temporal artery biopsy (TAB) specimens in patients with GCA.
Methods: The slides of 391 TAB specimens from patients with GCA were reviewed by two pathologists without clinical information.
Results: A total of 29 patients (26 females and 3 males, mean age 78.3 years) presented with unilateral PVL at the onset of the disease, and 362 patients (258 females, 104 males, mean age 74.7 years), did not. The pathological features strongly predictive for PVL were the presence (p = 0.003), number (p = 0.001) and aggregates of giant cells (p = 0.001), presence of plasmocytes (p = 0.002), thickened intima (p = 0.007), neoangiogenesis (p = 0.001) and degree of arterial occlusion (p = 0.006). Presence of neutrophils, eosinophils, parietal necrosis, calcification in the arterial wall and disruption of the internal elastic membrane were similar in both groups. Total obstruction of the arterial lumen by a thrombus, intensity of the inflammatory cells infiltration and inflammation of small vessels, nerves and veins surrounding the temporal artery were not associated with blindness. In multivariate analysis, only giant cells remained significantly associated with PVL.
Conclusion: Giant cells are strongly associated with PVL, with a significant gradient between great risk and large number of giant cells. However, PVL was neither associated with the intensity of the inflammatory infiltrate, nor with the presence of arterial thrombosis.
Statistics from Altmetric.com
Giant cell arteritis (GCA) is an inflammatory vasculopathy of unknown origin that affects large-sized and medium-sized arteries with a predilection for the cranial arteries of the elderly. Patients are usually aged over 50 and present with headache, jaw claudication, visual symptoms, fever and increased sedimentation rate.1 2 Microscopic examination of temporal artery biopsy (TAB) is still the gold standard test for the diagnosis of giant cell arteritis, showing infiltration of inflammatory cells into the arterial wall, with or without giant cells and interruption of the internal elastic laminae.1 2
Permanent visual loss (PVL) is the most feared cranial ischaemic complication of GCA.3 It is often an early manifestation of the disease and PVL occurs in 10 to 20% of patients in most series.4–7 Risk factors for blindness in patients with GCA are still unclear.4 However, a population-based study showed that a history of constitutional syndrome an abnormal temporal artery on physical examination and the presence of visual complications were predictors for biopsy-proven GCA.8 Moreover, in patients with biopsy-proven GCA from the same region the presence of human leukocyte antigen (HLA)-DRB1*04 alleles and the absence of anaemia at the time of admission were the best predictors for the development of visual ischaemic complications.9 More recently, it was reported that an abnormal temporal artery on physical examination and the absence of anaemia at the time of disease diagnosis were also good predictors for any severe ischaemic manifestations of GCA in this population.10 Histopathological features of TAB in patients with and without blindness, have not been described on large series yet. The aim of this study was to assess the pathological features predictive of PVL on TAB specimens from a large series of patients with GCA.
PATIENTS, MATERIAL AND METHODS
Cases
The recruitment of patients with GCA and polymyalgia rheumatica (PMR) and the inclusion and exclusion criteria used in this study have been described previously.11 12 Every department of Internal Medicine, Rheumatology, Geriatrics, Neurology and Ophthalmology of university hospitals in France, and Departments of Internal Medicine affiliated to the French Society of Internal Medicine (SNFMI), were contacted by mail in January 1991. Only newly-diagnosed patients were included on pre-established criteria, in order to avoid at best misclassification and recall bias.
For each new patient, a questionnaire reporting his or her medical history and clinical examination data had to be completed, and a blood sample had to be taken before corticosteroid treatment or at most 48 h after its initiation. The questionnaire had to be completed directly with the patient and not from the data recorded in the medical chart.
Diagnostic criteria for patients
Pre-established diagnostic criteria were as follows. Criterion 1: age over 50. Criterion 2: erythrocyte sedimentation rate (Westergren method) above 40 mm (except for a few cases with typical symptoms, for whom TAB was positive on microscopic examination). Criterion 3: clinical response to corticosteroid therapy within 72 h (disappearance of fever and pain). Criterion 4: positive TAB. Criterion 5: clinically abnormal temporal artery (tenderness, swelling, redness, nodular artery). Criterion 6: visual disturbances (blindness, diplopia, blurred vision) including those occurring during the first week of treatment. Criterion 7: jaw claudication. Criterion 8: headache, temporal headache, facial pain or sensation of facial swelling. Criterion 9: systemic symptoms such as fever, weight loss>10% of total weight, anorexia, malaise, asthenia. Criterion 10: polymyalgia rheumatica symptoms with persistent proximal muscle pain, tenderness or morning stiffness lasting more than 1 h, involving neck, shoulders and/or pelvic girdle (more than 2 weeks duration).
All patients had to fulfil criteria 1, 2 and 3. In addition to these three criteria, (1) patients included in the positive biopsy GCA group had to have criterion 4. (2) Patients included in the negative biopsy group had to fulfil two criteria from criteria 5, 6, 7, 8 and 9. Criterion 10 could be present, or not. However, patients with pure PMR without clinical sign or symptoms of GCA have not been included in this study. Patients with a diagnosis of GCA fulfilled the American College of Rheumatology (ACR) classification criteria.13
Exclusion criteria consisted in current malignant diseases, current infectious diseases, other inflammatory or vasculitis disease notably history of rheumatoid arthritis, systemic lupus erythaematosus and polyarteritis nodosa. All patients were followed-up over a 5-year period, and the mean follow-up in this series was 4 years. The patients were classified into subgroups once the inclusion criteria were reviewed by the coordinating centre.
Pathological examination of temporal artery biopsy specimens
A copy of the initial pathological report of TAB specimens was requested, and the slides were reviewed by two senior pathologists (DC and RL) without clinical information.
Development of the pre-established form
First, 30 slides were reviewed and all the items related to cell components of the inflammatory infiltrate and the architecture of the artery wall were collected and classified into categories. Then, the so-created form was used on the first 400 biopsies, and peculiarities not initially recorded were systematically noted.
The final review of the slides was made on a revised form taking into account the peculiarities noted on the first 400 biopsies, and all slides presented in this series have been reviewed with it.
Histological and cytological items
Various histological criteria were assessed: quality of the biopsy: excellent, good, medium, poor; orientation of the arterial sections: transversal or longitudinal; number of arterial sections; number of levels performed; intensity: absent, mild, medium, numerous; location of the inflammatory infiltrate: adventitia, media, intima; extent of the inflammatory infiltrate in the arterial circumference: focal<10%, from 10% to 25%, from 25% to 50%, from 50% to 75%, all circumference; nature of the inflammatory cells (giant cells: absence or presence; quantity: rare, medium, numerous); number of giant cells on the arterial section with the greatest score; presence of polynuclear neutrophils or eosinophils; presence of plasmocytes; parietal necrosis; intimal oedema: absent, mild, medium, marked; neoangiogenesis; percentage of obstruction of the arterial lumen: less than 25%, from 25% to 50%, from 50% to 75% and more than 75% obstruction; thrombosis: acute fibrinous or organised; percentage of disruption of the internal elastic lamina: less than 25%, from 25% to 50%, from 50% to 75%, more than 75%; inflammation surrounding: the vasa vasorum, the distant small vessels, the nerves, or the veins; presence of calcification in the arterial wall. Final histopathological diagnosis was made according to McDonnell et al.14
Analysis
Pathological features of the patients with GCA with and without PVL were compared. Data analysis was performed on SAS (SAS Institute Inc, Cary, North Carolina, USA). The χ2 test or Fisher exact test when required was applied to dichotomous variables. Odds ratio with 95% CIs were computed. For ordinal variables (as well as for the count of giant cells), the Wilcoxon rank sum test was performed. A logistic regression model with stepwise selection was performed with the variables found to be significant in the univariate analysis.
RESULTS
A total of 29 patients with GCA (26 females and 3 males, mean age 78.3 years) presented with unilateral PVL at onset of GCA, whereas 362 patients with GCA (258 females, 104 males, mean age 74.7 years) did not. Female gender (90% vs 71%, p = 0.03), older age (p = 0.01), shorter delay between the onset of the symptoms and the diagnosis (p = 0.03), diplopia (14% vs 4%; p = 0.02) and abnormal temporal artery with rigidity at clinical examination (69% vs 51%, p = 0.02) were statistically significantly associated with PVL. All inflammatory markers, including erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and platelet counts were similar in both groups.
Quality of the TAB specimens, orientation of the arterial sections, number of levels: (table 1)
Quality of TAB assessed in a semiquantitative way, the number of sections and the number of levels, as well as the orientation of the biopsy (transversal or longitudinal) were similar in both groups.
Histopathological classification of TAB specimens according to McDonnell et al (table 2)
In the group of patients with GCA with PVL, all but three cases of blindness occurred in patients with a positive TAB. Among them, 22 patients had a temporal arteritis with giant cells in the inflammatory infiltrate (76%) compared to 54.7% in the group of patients without PVL. The difference was significant (p = 0.02). Therefore, 26 out of 29 patients with GCA with blindness presented with a positive biopsy (89.6%), and the risk associated with blindness for a positive biopsy compared to a negative biopsy is estimated at 4 with a confidence interval excluding 1.
Microscopic features of the inflammatory infiltrate in TAB specimens (table 3)
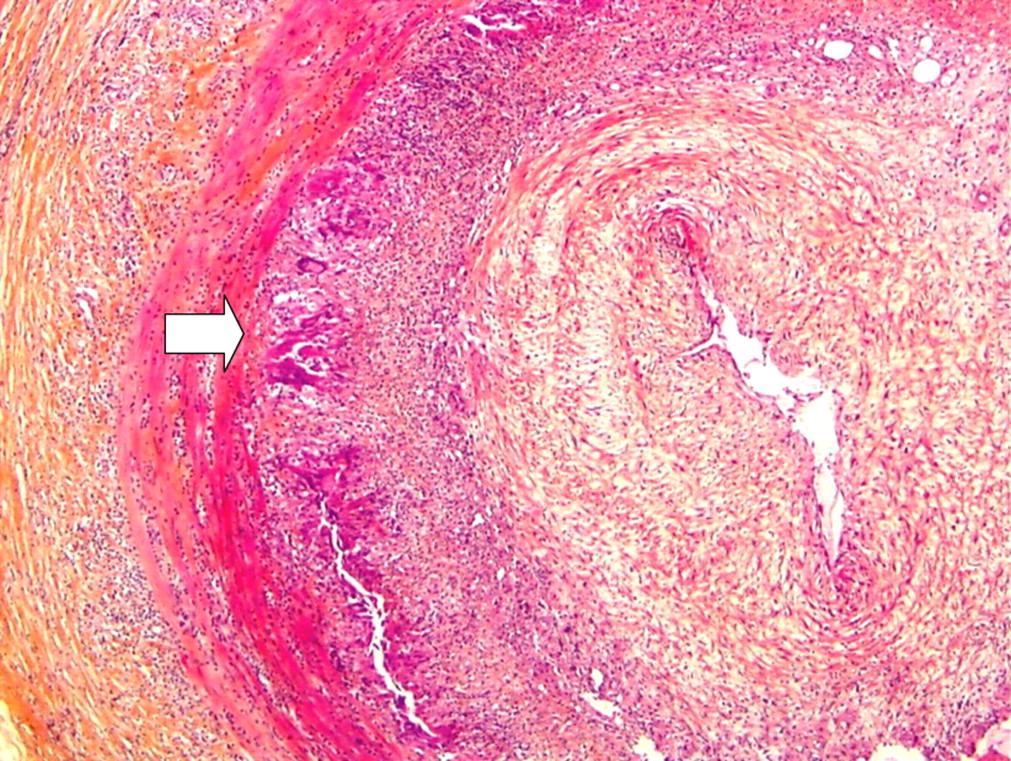
The pathological features strongly predictive of PVL were the presence (p = 0.003) and number of giant cells (p = 0.001) in the arterial wall, aggregates of giant cells (p = 0.001) (figs 1 and 2).

{kind=link}
{kind=link}
The odds ratio for blindness associated with the presence of giant cells is equal to 2.6 (95% CI 1.02 to 6.89, p = 0.027), and increases to 7.03 (95% CI 2.18 to 23.03, p<0.001) when there were numerous giant cells on the three-grade semiquantitative scale.
The presence of plasmocytes in the adventitia was also significantly associated with PVL, and the increased risk was estimated at 3 (odds ratio (OR) 3.17, 95% CI 1.13 to 8.59, p = 0.02).
PVL risk increased with the extent of inflammatory process through the circumference of the arterial wall (Wilcoxon rank sum test: 0.015). Positivity rates for neutrophils or eosinophils were similar in both groups. Risk for PVL increased neither with the intensity of the inflammatory infiltrate, nor with the location within the arterial wall. Necrosis was not associated with PVL. Inflammation surrounding the vasa vasorum, the vessels distant from the arterial wall small peripheral nerves or peripheral veins was not associated with PVL.
Lumen occlusion and pathological features of the arterial wall of TAB specimens in patients with GCA with and without PVL (table 4)
There was a strong correlation between the degree of arterial obstruction and the risk of PVL (p = 0.006, Wilcoxon rank sum test) (fig 1). The OR for PVL associated with obstruction greater than 75% as compared to obstruction lower than 25% was estimated at 5 (95% CI 1.33 to 22.48, p = 0.006). Global obstruction seemed to be mostly related to intima thickening, which is also highly correlated with PVL (p = 0.007, Wilcoxon rank sum test), and neoangiogenesis is the other feature strongly associated with PVL: OR 3.84 (95% CI 1.56 to 9.72, p<0.001).
Interestingly, thrombosis of the arterial lumen, whether organised or acute, occurred only in five patients with PVL and is not significantly associated with blindness. Prevalence of intima oedema was quite similar in patients with and without PVL, as well as calcifications located near the internal elastic lamina, which are more related to underlying arteriosclerosis.
There may be a relation between the degree of disruption of the internal elastic lamina and PVL, but its significance has to be confirmed on a larger series (p = 0.05, Wilcoxon rank sum test).
Analysis restricted to positive TAB specimens
When only patients with positive TAB were included in the analysis, results remained similar: non-significant items in the whole population remained non-significant in this subgroup, and significant items, such as giant cells assessed on a semiquantitative basis or count of giant cells, aggregates of giant cells, intima thickening, remained significantly associated with PVL.
Multivariate analysis
Pathological items significantly associated with PVL in univariate analysis were then integrated into a logistic regression model (quantity of giant cells on the semiquantitative basis, four grades; positivity of biopsy; degree of arterial obstruction; degree of intima thickening; presence of plasmocytes; inflammation extent on the arterial circumference; neoangiogenesis). The only significant item in the model was quantity of giant cells (p = 0.001), and none of the other items, including the positivity or negativity of the TAB, remained significant.
DISCUSSION
Blindness in GCA is usually due to anterior ischaemic optic neuropathy caused by ischaemic lesions of the optic nerve in relation to inflammatory involvement of the ophthalmic and posterior ciliary arteries. PVL is less frequently due to central retinal arterial occlusion and is rarely of cortical origin.3 9 15 Histopathological features of TAB specimens of patients with PVL have never been assessed on a large, prospective series. In our study, pathological features on TAB specimens were assessed by a referent pathologist without clinical information.
We found that the presence of numerous aggregates of giant cells in the inflammatory infiltrate, the presence of plasmocytes, the presence of a thickened intima with neoangiogenesis and the intensity of the arterial occlusion were significantly associated with blindness. However, when all significant items were integrated into the multivariate analysis, only giant cells assessed on a semiquantitative way emerged as associated with PVL. The positivity or negativity of the TAB, statistically significant in the univariate analysis was eliminated from the model.
There are only a few clinicopathological studies in the literature that assess histological findings and occurrence of PVL in patients with GCA:
In 1968 Bevan et al reported a series of 37 patients with GCA in which 11 patients experienced partial or complete loss of vision.16 On microscopic examination, 55% of these patients had arteritis with giant cells, 9% arteritis without giant cells and 36% healed arteritis. In the other group of 26 patients without eye involvement 65% had arteritis with giant cells, 15% arteritis without giant cells and 20% healed arteritis.16 The authors found no difference in the microscopic features of the patients with or without ocular involvement and found no pathological features predictive of ocular involvement.16
In 1994 in a series of 85 consecutive patients with GCA Schmidt and Loffler reported 37 patients who experienced anterior ischaemic optic neuropathy or central retinal artery occlusion.17 The authors did not report any association between optic nerve involvement and presence of giant cells in the inflammatory infiltrate (17 patients with GCA vs 20 patients with eye involvement and no giant cells in the inflammatory infiltrate).17
In 2005 Diaz et al reporting a series of 37 patients with GCA found a strong correlation between severity of clinical symptoms defined as visual symptoms (diplopia, blurred vision and loss of vision) and histopathological features such as necrosis (p<0.001), circumference of inflammatory involvement (p<0.001) and involvement of small vessels (p = 0.002).18 We did not find the same association in our study but Diaz et al did not assess PVL alone.18
In 2002 in a series of 31 patients Cid et al suggested that angiogenesis scores, estimated by the count of microvessels on temporal artery sections, were lower in patients presenting with ischaemic events such as amaurosis fugax, diplopia, permanent visual loss and stroke.19 In our study we only evaluated the presence of neoangiogenesis and not its intensity, but neoangiogenesis was eliminated from the logistic regression model when giant cells were taken into account.
Our results are in accordance with those of Kaiser et al who demonstrated in 1998 a correlation between the degree of intimal hyperplasia in the temporal artery specimens and cranial ischaemic complications.20 The authors compared 2 groups of 20 patients with and without luminal occlusive disease. They showed that patients with moderate and severe luminal obstruction (luminal diameter less than 65% of the internal elastic lamina diameter) on microscopic examination had significantly more frequent ocular symptoms, defined as new onset of blurred vision, amaurosis fugax and partial or complete blindness.20 Unfortunately the authors did not assess PVL in particular.
In 1997 Weyand et al reported a series of 23 patients with GCA in which 13 patients experienced ischaemic symptoms, such as jaw claudication or visual symptoms, but PVL was not individualised.21 The authors found higher concentrations of interferon (IFN)γ-mRNA in the temporal artery biopsy specimens of the 13 patients (p = 0.008). They showed that giant cells in the granulomatous infiltrate of the TAB specimens found in 14 patients were associated with the local synthesis of IFNγ-mRNA (p = 0.003) but the presence of giant cells and visual symptoms, notably PVL was not assessed.21
Interestingly, a cytosine–adenine (CA) repeat functional polymorphism in the first intron of the IFNγ gene was associated with some clinical differences between biopsy-proven GCA and isolated PMR. This was also the case for specific clinical manifestations of GCA such as visual ischaemic complications. In this regard, association between a 126 base pair allele, associated with high IFNγ production, with patients with GCA with visual ischaemic manifestations, and the inverse correlation with the 128 base pair allele (low IFNγ producer) was found.22
Our results show that patients with GCA who experienced blindness have some specific histological features with numerous giant cells, plasmocytes and thickened intima with neoangiogenesis. Giant cells seem to be the main histopathological feature associated with blindness.
In our study, blindness was not associated with the intensity of the inflammatory infiltrate, necrosis, the presence of neutrophils or eosinophils and arterial thrombosis. Thrombosis of the temporal artery is not the decisive event for the occurrence of blindness.
In conclusion, our study shows that patients with PVL have some specific pathological features, and giant cells are strongly associated with blindness. Moreover, there is a significant positive correlation between the quantity of giant cells and the risk of blindness, as shown in univariate and in multivariate analysis. Our study may suggest that GCA is a heterogenous group of diseases, and patients with giant cells may be different from patients without giant cells.
Acknowledgments
We are thankful to Ms Valérie Petigny for her careful handling of the data collection and the database.
REFERENCES
Footnotes
Competing interests: None declared.
Ethics approval: Ethics approval was obtained.