Article Text

Abstract
Background: In systemic sclerosis (SSc) reduced capillary density decreases blood flow and leads to tissue ischaemia and fingertip ulcers. Nail fold videocapillaroscopy (NVC) is a diagnostic and follow-up parameter useful to evaluate the severity, activity and the stage of SSc microvascular damage. Autologous haemopoietic stem cell transplantation (HSCT) is a new treatment for patients with severe diffuse cutaneous systemic sclerosis (dcSSc) refractory to conventional therapies. We aimed to evaluate the improvement of microvasculature after HSCT using NVC.
Methods: A total of 16 patients with severe dcSSc with a “late” videocapillaroscopy pattern underwent an immunesuppressive treatment: 6 were treated with HSCT and 10 with monthly pulse cyclophosphamide (CYC) 1 g for 6 months and then orally with 50 mg/day for further 6 months.
NVC was performed before and after 3 months from the beginning of each treatment and then repeated every 3 months.
Results: In all patients, before HSCT NVC showed large avascular areas and ramified capillaries and vascular architectural disorganisation (“late” pattern). At 3 months after HSCT, the NVC pattern changed from “late” into “active”, showing frequent giant capillaries (>6/mm) and haemorrhages, absence of avascular areas and angiogenesis phenomena; 1 year after HSCT, microvascular abnormalities were still in the “active” pattern. In patients treated with CYC, no NVC modifications were observed during 24 months of follow-up and the pattern always remained “late”.
Conclusions: These results indicate that HSCT with a high dose CYC regimen may foster vascular remodelling, while CYC at lower doses and with a chronic regimen does not influence the microvasculature.
Statistics from Altmetric.com
Systemic sclerosis (SSc) is a multiorgan disease characterised by widespread fibrosis, activation of immune cells, production of autoantibodies and injury to vascular as well as microvascular structures.1 It is likely that prolonged endothelial cell perturbation and activation, induced by ischaemia and reperfusion, may lead to dysfunction and irreversible loss of integrity of the microvascular system. In vivo, these changes can be detected by nail fold videocapillaroscopy (NVC), which shows a variety of morphological modifications including enlarged capillaries, bushy capillary formations, microhaemorrhages and a variable loss of capillaries with or without avascular areas.2 NVC is a non-invasive technique useful for diagnosis of SSc and also allowing for follow-up of microvascular modifications, usually classified into “early”, “active” and “late” patterns.3–7
Cyclophosphamide (CYC), administered orally and intravenously, has been shown to improve skin thickening, stabilise pulmonary function and increase survival in non-randomised trials.8 9 However, according to recent randomised trials, the beneficial effect of CYC seems to be limited.10 In fact, the first randomised controlled trial (RCT) on pulse CYC in pulmonary fibrosis in SSc clearly shows that CYC is moderately helpful in stabilising lung function: only a statistical trend of FVC to amelioration has been demonstrated while other primary (diffusion capacity for carbon monoxide (DLCO), total lung capacity (TLC) and forced expiratory volume in 1 s (FEV1)) and secondary (high-resolution computed tomography (HRCT), dyspnoea score ) outcome measures did not reach statistical significance.11
When CYC (2 mg/kg) was previously used in a blinded RCT vs placebo for 12 months, the same results were obtained11 and the authors assessed that CYC had a modest beneficial effect on lung function, dyspnoea, skin thickening and quality of life.12
In the last decade autologous haemopoietic stem cell transplantation (HSCT) has emerged as a new treatment for patients affected by severe diffuse cutaneous SSc (dcSSc).13 The rationale for the use of HSCT is mainly based on the capacity to significantly reduce autoaggressive lymphocytes.14–16 The aim of our work was to investigate in an observational study the effect of HSCT on microvascular modifications assessed by NVC in patients with dcSSc refractory to conventional treatments.
MATERIALS AND METHODS
Patients
A total of 16 patients with SSc were treated intensively with CYC under 2 different regimens: 6 treated with HSCT (mean age 48.5 years (range 36–64 years), mean disease duration of 28 months (18–48 months)) and 10 with monthly pulses (mean age 47.2 years (range 28–61 years), mean disease duration of 32 months (12–42)). Before treatment all patients showed a NVC “late” pattern, indicating a rapid progression of microvascular involvement.
The 10 patients treated with monthly pulses received intravenous CYC (1 g) for 6 months. Blood cell count, renal and liver function were controlled every month before each CYC infusion and blood cells count was repeated at nadir (about 14 days after the therapy). After 6 months of intravenous treatment, CYC was administered orally to all patients for 6 months (100 mg/daily).
The other six patients were treated with HSCT: a mobilisation regimen with CYC 4 g/m2 (administered over 2 days), followed by recombinant human granulocyte colony stimulating factor (rHu G-CSF) was used. Circulating HSCs were collected through one or more leukapheresis processes during the haematological recovery: CD34+ cells were positively selected by immunomagnetic selection (CliniMacs, Miltenyi Biotec, Bergisch Gladbach, Germany) and cryopreserved until the day of transplantation. The conditioning regimens were CYC (100 mg/kg) and N,N'N'-triethylenethiophosphoramide (thioTEPA) (10 mg/kg) for the first patient and only CYC (200 mg/kg) for the other three patients, respectively. Intravenous rabbit anti-thymocyte globulin (ATG) (Thymoglobulin, Genzyme, Cambridge, Massachusetts, USA) was administered in all these patients (total dose 7.5 mg/kg) and was stopped in only one patient after the first administration (2,5 mg/kg) because of capillary leak syndrome. Cryopreserved purified CD34+ cells were thawed and infused during after the completion of the conditioning regimen. No side effects were observed during hospitaliazation.
Before HSCT and at 3, 6, 12 and 24 months after, patients were assessed by physical examination, laboratory tests and instrumental examination in order to evaluate their internal organ involvement.17
NVC
NVC was performed before and at 3 months from the beginning of the treatment and then repeated every 6 months in order to evaluate the evolution of scleroderma NVC patterns.
Each patient was acclimatised for 30 min at a comfortable temperature prior to capillaroscopy. NVC was performed using an optical probe videocapillaroscope equipped with 100× and 200 × contact lenses and connected to image analyse software (Videocap; DS MediGroup, Milan, Italy). Images (pixel dimensions 762 horizontal × 582 vertical) were also observed on a high-resolution colour monitor (14 inches) and printed on a digital PAL video printer (print format 84.5×110 mm , 256 colours; Hitachi, Tokyo Japan). The same operator, without knowledge of the patient’s clinical diagnosis, disease severity or treatment, performed NVC in a blind manner and classified the images. The images were read independently by three investigators completely blinded to clinical and treatment status, and an inter-reader reliability coefficient generated.
After a drop of immersion oil was placed on the nail fold bed to improve the image resolution, the nail folds of all 10 fingers were examined in each patient. According to previous classifications, the following parameters were considered: presence of enlarged and giant capillaries, haemorragies, loss of capillaries, disorganisation of the vascular array and ramified/bushy capillaries.
On the basis of the NVC abnormalities, patients with SSc were distributed into a NVC pattern, classified as a scleroderma NVC pattern.7 The patterns included:
Early: few (fewer than four altered capillaries per mm) enlarged/giant capillaries, few capillary haemorrhages, relatively well preserved capillary distribution, no evident loss of capillaries.
Active: frequent (more than six altered capillaries per mm) giant capillaries, frequent capillary haemorrhages, moderate loss of capillaries, mild (between four and six altered capillaries per mm) disorganisation of the capillary architecture, absent or mild ramified capillaries.
Late: irregular enlargement of the capillaries, few or absent giant capillaries and haemorrhages, severe loss of capillaries with large avascular areas, disorganisation of the normal capillary array and ramified/bushy capillaries.
A semiquantitative rating scale to score these changes was adopted, (0, no changes; 1, fewer than four alterations; 2, four to six alterations; 3, more than six alterations per mm): for each subject, the mean score for each of these parameters was obtained from the analysis of the second, third, fourth and fifth fingers of both hands, using the scoring system described.7 Fingers affected by local trauma were not analysed.
Statistics
Data were analysed using SPSS V. 10.0 for Windows (SPSS, Chicago, Illinois, USA). Descriptive statistics were expressed as mean (1SD).
Normal distribution of each examined parameter was verified by the Kolmogorov–Smirnoff test. The statistical significance of the differences between means of two groups was evaluated by the Student t test for unpaired data. A p level of ⩽0.05 was considered statistically significant.
The effect size, a standard way to determine the degree of improvement of a particular therapy, was also calculated for each NVC parameter. The effect size is calculated as the ratio of the treatment effect (mean differences in treatment group minus differences in control group) to the pooled standard deviation of these differences. This calculation entails the use of means, for baseline and final data (or baseline and change during study), with a measure of variability such as SD. By convention, an effect size <0.2 is usually considered as trivial, >0.2–0.5 as small, >0.5–0.8 as moderate, >0.8–1.2 as important and >1.2 as very important.
RESULTS
DLCO was reduced in all patients treated with HSCT (mean value 48% of predicted), and only two patients had restrictive syndrome at lung function test. Bibasilar lung fibrosis was detected with HRCT in two patients, while in the other four patients “ground glass” areas were found without any alteration of lung function tests. In two patients, mild to moderate pulmonary hypertension, evaluated with cardiac echocolourdoppler, was present. In all patients the left ventricular ejection fraction was normal and no significant arrhytmias were registered by Holter electrocardiogram (ECG). Creatinine clearance was normal and no proteinuria was observed.
In seven patients treated with CYC, HRCT showed areas of “ground glass” and in three patients a mild fibrosis. No pulmonary hypertension, cardiac and kidney involvement was present in this group.
No serious side effects were observed during either treatment.
In patients treated with HSCT, a stabilisation of lung function and a mild improvement of DLCO was detected (mean value 59% after 2 years); in two patients pulmonary pressure progressively decreased to borderline values and dyspnoea was present only at exertion but no longer during ordinary activities.
In the group treated with CYC, no significant modifications of lung function and HRCT were observed.
Modified Rodnan Skin Score (mRSS) significantly improved in patients treated with HSCT (p = 0.02 after 12 months, p = 0.00 after 24 months), while in the CYC group no statistically significant modifications were observed (p = 0.367 after 12 months and p = 0.425 after 24 months).When compared between the two groups, mRSS became statistically significant in patients treated with HSCT after 1 year (p = 0.007), reaching p = 0.001 at 2 years.
Disability, evaluated with the Scleroderma Health Assessment Questionnaire (SHAQ), improved in patients treated with HSCT after 12 months (p = 0.035) and was confirmed at 24 months (p = 0.030); in patients treated with CYC, SHAQ did not change during follow-up.
Nail fold videocapillaroscopy
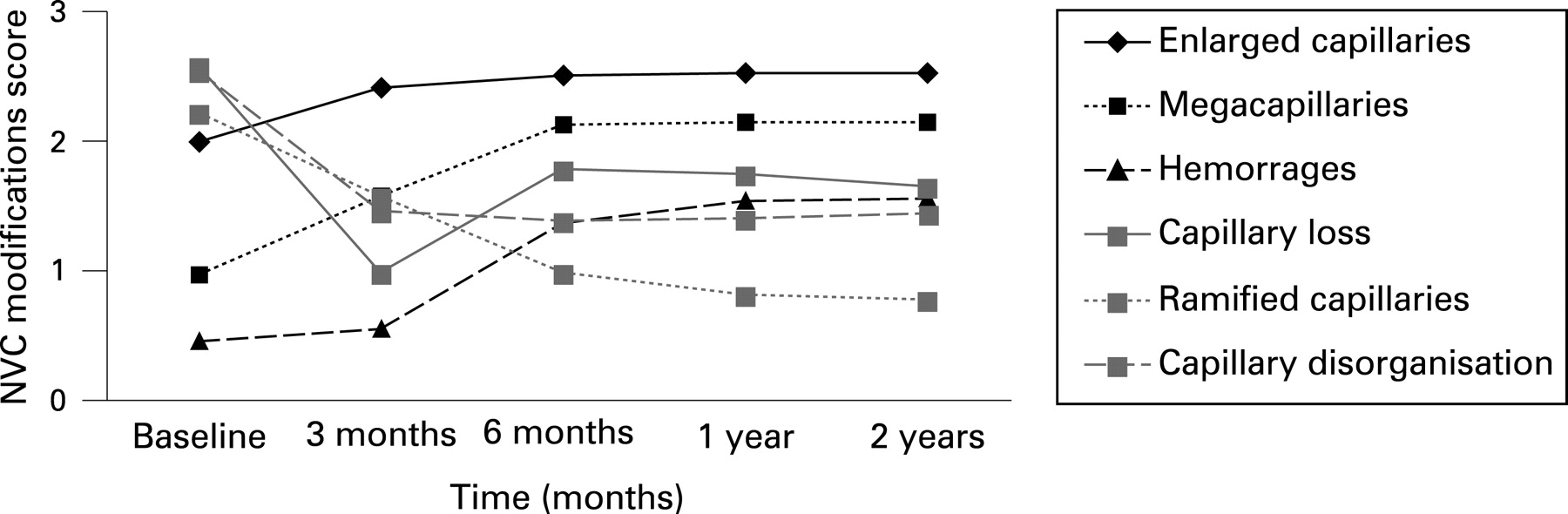
Capillaroscopic changes during the treatment in patients treated with HSCT are reported in fig 1.

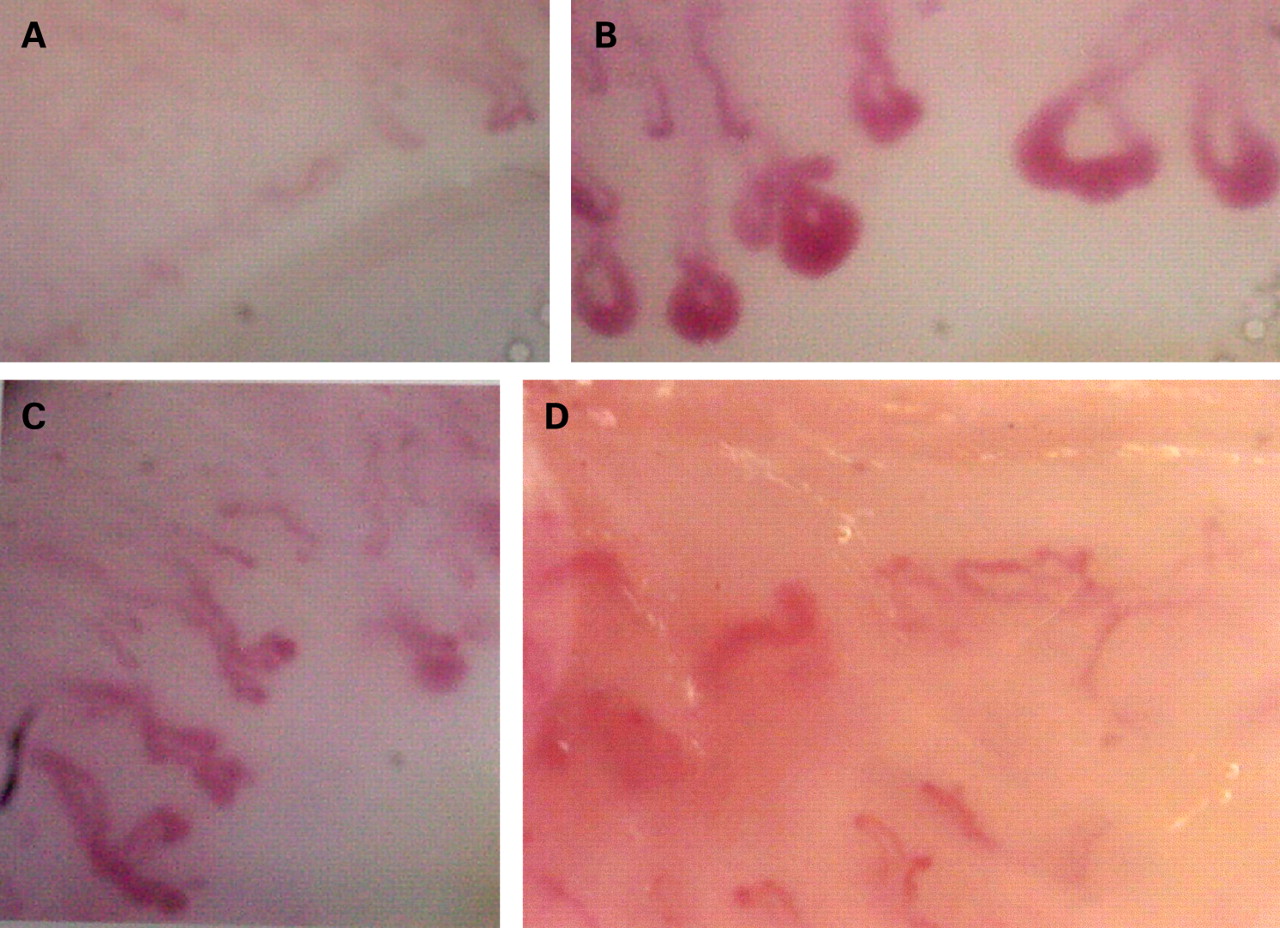
Prior to HSCT, NVC showed few giant capillaries, severe loss of capillaries with large avascular areas, ramified capillaries and vascular architectural disorganisation in all patients. These morphological modifications were classified as a “late” SSc pattern (fig 2A).

{kind=link}
{kind=link}
In patients treated with HSCT, after 3 months frequent giant capillaries (more than 6 per mm) and haemorrages, absence of avascular areas and disorganisation of the normal capillary array with ramified/bushy capillaries (suggesting angiogenesis phenomena) were observed. These alterations were classified as an “active” SSc pattern (fig 2B). The active pattern was unmodified also at 6, 12 and 24 months.
In patients treated with CYC, no significant NVC modifications at 3, 6, 12 and 24 months were seen (fig 2C,D).
A semiquantitative analysis of the most relevant NVC alterations (enlarged capillaries, giant capillaries and haemorrhagies, loss of capillaries, ramified capillaries and capillary disorganisation) of these two groups of patients is shown in table 1.
After 2 years the number of enlarged and giant capillaries and haemorrages showed a stastistically significant increase in patients treated with HSCT, while this was unchanged in patients treated with CYC (see table 1). Effect size, for retrospective studies, indicated a significant difference between the two groups for each NVC parameter: 1.78 for enlarged capillaries, 0.83 for giant capillaries and 2.80 for haemorrages.
A statistically significant reduction of loss of capillaries, ramified capillaries and capillary disorganisation was found in patients treated with HSCT only, while in the group treated with CYC no significant modifications were observed (see table 1). These NVC parameters, after 2 years of follow-up, were still significantly different from those seen in the CYC group (p = 0.000). Effect size demonstrated a very important difference between the two groups: 2.52 for capillary loss, 3.01 for ramified capillaries and 2.34 for capillary disorganisation.
DISCUSSION
The present results, even on a limited number of patients, confirm that refractory dcSSc may be successfully treated with HSCT, in agreement with previous observations.13–16 Indeed, the data obtained with NVC clearly demonstrate that HSCT can improve the microvascular derangement.
Usually, the three major NVC patterns reflect the evolution of SSc microangiopathy. Their recognition may be useful in assessing microvascular damage in individual patients at a single point and longitudinally in time. In healthy subjects, capillary loops and capillary distribution do not change with time, and the same pattern is usually maintained.2
In SSc, NVC patterns may change with time. NVC abnormalities such as enlarged and giant capillaries are the first sign of SSc microangiopathy that changes progressively in patients with longer disease duration. By contrast, capillary rarefaction and ramifications are rare in the early stage of SSc but are common in patients with longer SSc duration. Indeed, NVC patterns correlate with the duration of Raynaud phenomenon and reflect the evolution of the disease process.2
In our cases, we obtained a reversal from a “late” pattern, characterised by avascular areas, to an earlier “active” pattern in which giant capillaries, frequent capillary haemorrhages and moderate loss of capillaries are usually observed. This shows that, with HSCT, a recovery of the microvasculature may be obtained even in patients with advanced disease. Remodelling of collagen following allogenic HSCT has been also described in SSc.18 In our patients, angiogenetic phoenomena were detected after HSCT, suggesting that this therapeutic procedure was successful in blocking deterioration of the microvessels and also was partially able to restore the previous vessel structure. It is still not clear if these results were achieved through the immunosuppressive effect of the conditioning regimen and its effect on local perivascular inflammatory infiltrate or by the impact of the whole procedure on angiogenesis. It has also been reported that G-CSF, when used to mobilise stem cells from the bone marrow, promotes neovascularisation by releasing vascular epithelial growth factor (VEGF) from neutrophils.19 This may provide some results on the vasculopathy; however, in SSc, a reduction of angiogenesis has been demonstrated, despite the striking increase of VEGF expression.20 21 A normalisation of the bone marrow niche including endothelial precursor cells, known to be reduced in SSc,22 could also play a role in vascular remodelling.
NVC is a useful tool for the diagnosis of SSc, in particular in the early phase.7 It is a practical tool directly showing the modifications of microvasculature, but it has not yet been used in trials to demonstrate the modifications of microvessels. In a few other reports NVC has been used to demonstrate modifications of the microvasculature under treatment. In particular, in an observational study on few patients evaluated with NVC, bosentan did not show any effect on vascular structure despite the beneficial effect on digital vasculopaty.23
Further studies are necessary to address this point and clarify if the microvasculature in patients with SSc may benefit from high doses of CYC or from the reinfusion of CD34+ cells.
REFERENCES
Footnotes
Competing interests: None declared.
Ethics approval: Ethics approval was obtained.