Article Text

Abstract
Objective To prospectively analyse the risk for disease relapses in patients with rheumatoid arthritis (RA) in sustained remission, either continuing, tapering or stopping disease-modifying antirheumatic drugs (DMARDs) in a prospective randomised controlled trial.
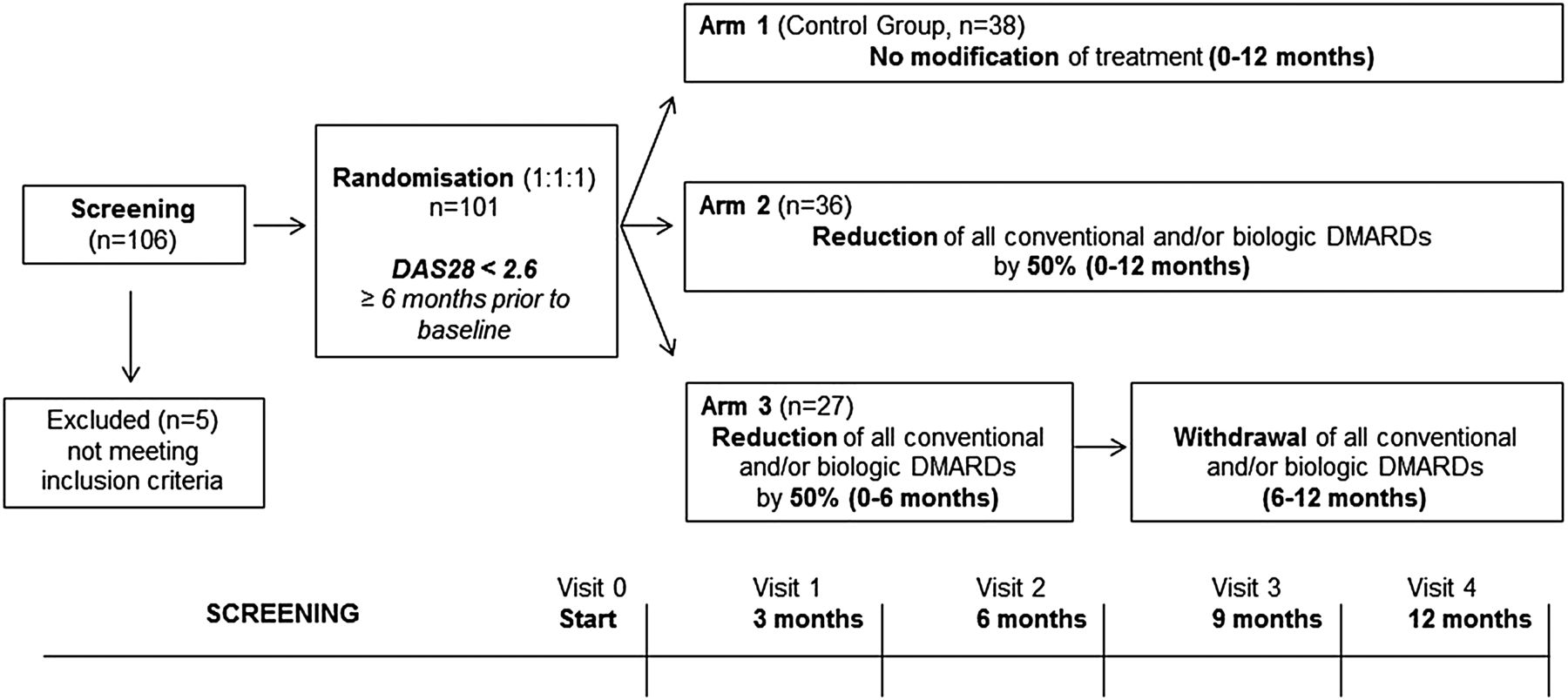
Methods Reduction of Therapy in patients with Rheumatoid arthritis in Ongoing remission is a multicentre, randomised controlled, parallel-group phase 3 trial evaluating the effects of tapering and stopping all conventional and/or biological DMARDs in patients with RA in stable remission. Patients (disease activity score 28 (DAS28)<2.6 for least 6 months) were randomised into three arms, either continuing DMARDs (arm 1), tapering DMARDs by 50% (arm 2) or stopping DMARDs after 6 months tapering (arm 3). The primary endpoint was sustained remission during 12 months.
Results In this interim analysis, the first 101 patients who completed the study were analysed. At baseline, all patients fulfilled DAS28 remission and 70% also American College of Rheumatology- European League Against Rheumatism Boolean remission. 82.2% of the patients received methotrexate, 40.6% biological DMARDs and 9.9% other DMARDs. Overall, 67 patients (66.3%) remained in remission for 12 months, whereas 34 patients (33.7%) relapsed. The incidence of relapses was related to study arms (p=0.007; arm 1: 15.8%; arm 2: 38.9%; arm 3: 51.9%). Multivariate logistic regression identified anticitrullinated protein antibodies (ACPA) positivity (p=0.038) and treatment reduction (in comparison to continuation) as predictors for relapse (arm 2: p=0.012; arm 3: p=0.003).
Conclusions This randomised controlled study testing three different treatment strategies in patients with RA in sustained remission demonstrated that more than half of the patients maintain in remission after tapering or stopping conventional and biological DMARD treatment. Relapses occurred particularly in the first 6 months after treatment reduction and were associated with the presence of ACPA.
Trial registration number 2009-015740-42.
- Rheumatoid Arthritis
- Disease Activity
- Treatment
- DMARDs (synthetic)
- DMARDs (biologic)
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA) is an inflammatory joint disease characterised by synovitis, joint destruction and impaired physical function.1 Diagnosis of RA affords the fast initiation and consequent continuation of disease-modifying antirheumatic drugs (DMARDs) treatment. These drugs mitigate or even abrogate the clinical symptoms of RA and prevent damage. Remission of disease is the primary goal in the treatment of RA.2 Several factors have substantially improved the outcome of patients with RA during the last years. Hence, (i) RA is diagnosed earlier, allowing faster treatment initiation; (ii) better monitoring of disease activity has allowed a more flexible treatment adaptation to reach remission; and (iii) biological DMARDs permit the successful treatment of patients with RA failing on conventional drugs.
Based on these developments, an increasing number of patients reach clinical disease remission. A recent survey from the NOR-DMARD study shows doubling of remission rates in the last decade.3 Furthermore, many of these patients maintain remission over two subsequent visits.4 Due to these changes, new challenges for both physicians and patients arise: patients inquire whether continuation of DMARDs is still necessary or whether treatment can be tapered or even stopped. Paucity of prospective clinical studies, specifically addressing this topic, however, makes it challenging to answer this question. The potential side effects of antirheumatic drugs and their high costs make such considerations even more important. Furthermore, a state of sustained remission implies the dilemma whether disease is actually cured or just effectively suppressed by treatment. Unfortunately, these two states can hardly be distinguished by the currently available clinical tools, which have been successfully developed for monitoring disease activity.
Virtually no prospective randomised controlled trials with the primary aim to taper or stop treatment in patients in sustained disease remission have been carried out. The only prospective randomised controlled trials with relapse of disease after treatment tapering as a primary endpoint go back decades.5 ,6 Later trials were either not randomized7–12 or were post hoc analyses in randomised clinical trial aiming to achieve remission.13–15 Nonetheless, these studies have substantially widened our horizon in the management of RA, suggesting that tapering of antirheumatic treatment may be a feasible strategy in some patients. Also, EULAR guidelines mention the possibility of tapering of biological DMARD therapy once remission is sustained.16
To study the potential to taper or stop DMARD therapy, we setup a prospective randomised controlled study, enrolling patients with RA in sustained remission to three different treatment arms, based on continuation, tapering or stopping of DMARD therapy. The primary endpoint of this Reduction of Therapy in patients with Rheumatoid arthritis in Ongoing remission (RETRO) study was the maintenance of remission for 12 months. In addition, we searched for potential predictors for relapses in patients tapering or stopping DMARD treatment.
Methods
Study objective and inclusion criteria
RETRO is an investigator-initiated, phase 3, multicentre, randomised, open, prospective, controlled, parallel-group study (EudraCT number 2009-015740-42). The primary objective was to evaluate the possibility of tapering or stopping antirheumatic therapy in patients fulfilling the American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) 2010 classification criteria for RA17 and having achieved stable remission. To be enrolled, patients had to have RA for at least 12 months and sustained clinical remission with a disease activity score 28 (DAS28) based on erythrocyte sedimentation rate (ESR) of <2.6 for at least 6 months.18 Remission had to be documented at least at three sequential visits covering a screening period of 6 months. In addition, patients had to receive stable treatment with antirheumatic drugs, such as conventional DMARDs (methotrexate, leflunomide, hydroxychloroquine and sulfasalazine) and/or biological DMARDs (infliximab, adalimumab, etanercept, golimumab, certolizumab, tocilizumab) without alteration in dose for at least 6 months. Patients receiving rituximab or abatacept or those with steroids of >5 mg/day within 12 months prior to screening were excluded from the study.
Patients and treatment
Patients meeting the inclusion criteria and consenting to the study were randomised into three different trial arms: arm 1 (continuation) kept existing conventional and/or biological DMARD regimen at full dose for 12 months. Arm 2 (tapering) reduced the dose of all conventional and/or biological DMARDs by 50% for the next 12 months. Arm 3 (stop) reduced their dose by 50% for the first 6 months before entirely stopping all DMARDs (figure 1). Tapering of conventional DMARDs and tocilizumab was done by reducing their respective doses by 50% without changing application intervals. Tapering of tumour necrosis factor (TNF) inhibitors was accomplished by doubling the time between applications. If stable doses of low-dose glucocorticoids (≤5 mg/day) were used at baseline, they were also reduced like conventional DMARDs. Non-steroidal anti-inflammatory drugs could be taken on demand before and after inclusion into the study. Relapse of disease was defined as leaving DAS28 remission corresponding to a DAS28-ESR score of >2.6. In case of relapse, all patients randomised to the reduction groups were re-exposed to their original full-dose treatment regimen and entered the observational phase of the study. This strategy was predefined in the study protocol.
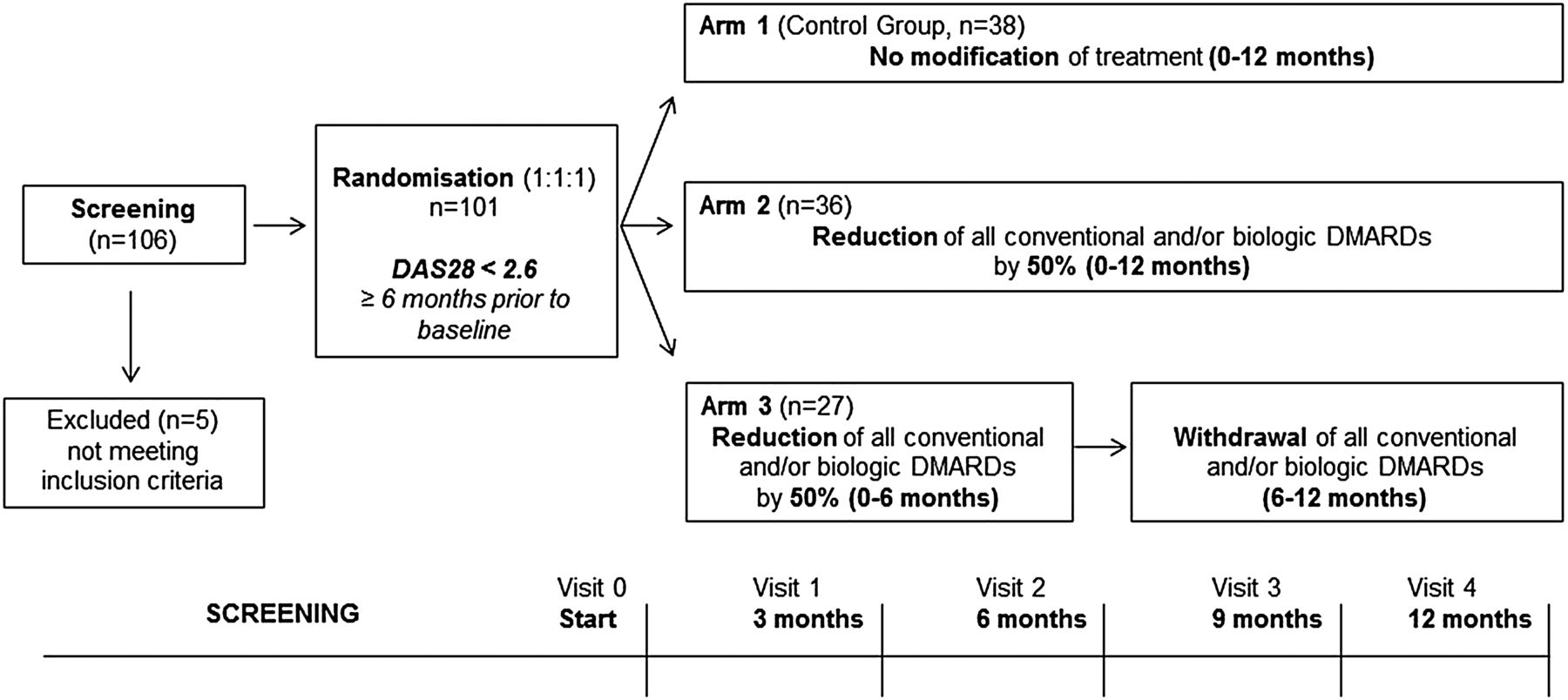
Design of the study. Prospective randomised controlled trial with three treatment arms. In total, 106 patients with rheumatoid arthritis were screened, 101 patients with a disease activity score 28 (DAS28) of <2.6, indicating disease remission were randomised into the three study arms (continuation, tapering, stopping) and were followed for 1 year with regular visits every 3 months. DMARDs, disease-modifying antirheumatic drug.
From May 2010 until May 2013, 101 patients at 11 different centres were randomised and completed the study. Also, 2 of the 101 patients fulfilling the inclusion criteria showed a slightly elevated DAS28 score (2.68 and 2.71) due to upper respiratory tract infection and associated elevation of ESR. Since no increased disease activity of arthritis was found, these two patients were also randomised.
Efficacy assessments
Primary efficacy parameter was disease activity, which was assessed at baseline and after months 3, 6, 9 and 12 using the DAS28-ESR by designated doctors at each centre. Additionally, fulfilment of the ACR/EULAR Boolean remission criteria was assessed at each visit.19 Assessment of physical function was done using the disability index of the health assessment questionnaire (HAQ-DI).20 With respect to demographic and additional disease-specific parameters, age, sex and body mass index, as well as disease duration, duration of remission, rheumatoid factor (RF) and anticitrullinated protein antibodies (ACPA) status, were assessed at baseline. Furthermore, antirheumatic therapy and any other concomitant treatment were recorded at each visit.
Statistical analysis
We performed an interim analysis of the first 101 patients who completed the 12-month study period. Patients were allocated to treatment arms in a 1:1:1 ratio according to a randomisation plan using randomly permuted blocks (number of blocks: 1) generated by the statistician. According to an a priori sample size calculation, the total study population would be 318. In descriptive analyses, treatment arms as well as patients in sustained remission versus those relapsing were analysed for demographic and disease-related parameters. Descriptive results are stated in medians and IQRs as well as arithmetic means and SDs. Corresponding inferential comparisons of subgroups were calculated using Kruskal–Wallis or Mann–Whitney U tests for numerical variables and exact χ2 tests for nominal characteristics. A multivariate logistic regression model using ‘enter’ method was used in order to predict the occurrence of disease relapses from the following set of baseline characteristics including an intercept term: age, gender, duration of disease, duration of remission, RF status, ACPA status, ACR/EULAR remission status, biological DMARD use and allocation to study arms 2 or 3 (in comparison to reference arm 1). Kaplan–Meier plots were used to illustrate relapses over the 12 months of the study with respect to (i) allocation to study arms, (ii) fulfilment of ACR/EULAR Boolean remission, (iii) ACPA positivity and (iv) treatment with biological DMARDs. SPSS software V.21 was used for calculation of results, whereas p values ≤0.05 were considered statistically significant.
Results
Baseline characteristics of the patients
Table 1 summarises the baseline characteristics of the patients. In brief, 61.4% of the 101 patients were women (N=62 women, N=39 men). Median (IQR) age was 57.0 (19) years while median (IQR) disease duration was 5.0 (7) years. Median duration of remission was 12.0 (12) months before study entry, with no difference between the three trial arms. Swollen and tender joints were very rare in the study population attributing to a median (IQR) swollen joint count of 0.0 (0) and tender joint count of 0.0 (0), which was also reflected by more than two-thirds of the patients fulfilling the ACR/EULAR remission criteria (77.2%; N=78). Importantly, there were no differences in baseline DAS28 scores or the number of patients fulfilling ACR/EULAR remission criteria between the three arms. Also, baseline functional status, measured by HAQ-DI, was generally low and not significantly different among the different treatment arms. The majority of patients were receiving methotrexate (82.2%), whereas 9.9% were treated with other conventional DMARDs. Biological DMARDs were used by 40.6% of the patients with TNF inhibitors as the leading agents (75.6%).
Baseline characteristics of the patients
Prevalence of disease relapses after continuation, tapering or stopping treatment
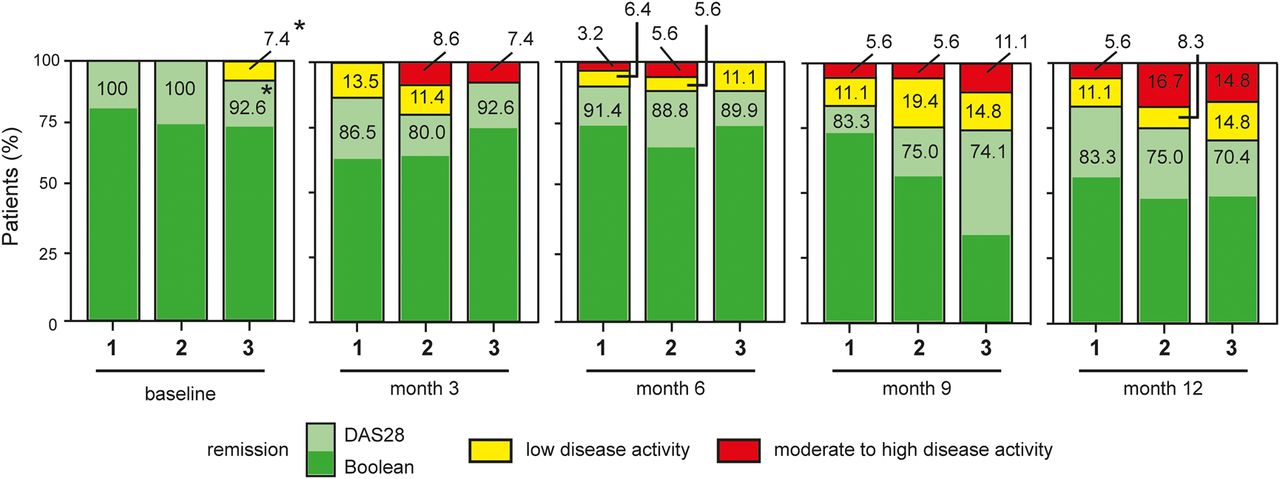
In total, 67 of the 101 patients (66.3%) remained in remission over the entire follow-up period of 12 months, whereas 34 patients (33.7%) relapsed (figure 2A). Prevalence of disease relapse was as low as 15.8% with continuation of antirheumatic therapy (arm 1) but higher when tapering treatment (arm 2: 38.9%; χ2(1)=5.0, p=0.036) or when stopping it (arm 3: 51.9%; χ2(1)=9.6, p=0.003). Overall, 44.4% (N=28) of patients in the two reduction arms relapsed. No significant differences regarding the incidence of relapses between the tapering and stopping regimen arms were found (χ2=1.050, p=0.443). The majority of relapses (N=19) occurred within the first 6 months during the tapering phase (arm 2: N=9 out of 14; arm 3: N=10 out of 14) of the study. Figure 3 shows the development of DAS28 values over 12 months of study period.

Kaplan–Meier curves for maintenance of remission. Curves indicate loss of remission over 12 months in patients with rheumatoid arthritis in relation to different parameters. (A) Treatment arms (blue: continuing; green: tapering; yellow: stopping). (B) American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) remission fulfilled (green) or not fulfilled (blue) at baseline. (C) Anticitrullinated protein antibody (ACPA) status (green: positive; blue: negative). (D) Use of biological disease-modifying antirheumatic drugs (DMARDs) therapy (green: use of biological DMARDs; blue: no biological DMARDs). The y-axis indicates the percentage of patients with rheumatoid arthritis in sustained remission (100% at baseline), and the x-axis indicates time.

{kind=link}
{kind=link}
{kind=link}
Development of disease activity score 28 (DAS28)-erythrocyte sedimentation rate. Bars indicate percentage of patients in remission (green), low-disease activity (yellow) and moderate-to-high-disease activity (red) in the three study arms (arm 1: continuing; arm 2: tapering; arm 3: stopping) at baseline and months 3, 6, 9 and 12. Remission is defined by DAS28 of <2.6, low-disease activity between 2.61 and 3.2 and moderate-to-high-disease activity represents a DAS28 score of >3.21. *Two patients had a DAS28 slightly above 2.6 due to respiratory infection without any clinical signs of activity of arthritis.
Baseline characteristics of patients remaining in remission or relapsing
Descriptive baseline characteristics of total population and ACPA-positive patients who remained in remission or experienced a relapse of disease are depicted in table 2. Age, disease duration and duration of remission at baseline were very similar between the remission and the relapse group. Although ESR levels and DAS28 scores showed a tendency for higher baseline values in patients who relapsed, other single and composite clinical activity measures, such as tender and swollen joint counts, C-reactive protein level and ACR/EULAR remission status, were virtually identical in the two groups, suggesting no major impact of residual disease activity on subsequent relapses. With respect to ACPA status, >70% of the patients with relapsing disease showed ACPA positivity, whereas this number was lower (53%) in patients remaining in continuous remission. Furthermore, relapsing patients were preferentially women (73.5%), whereas sex distribution in the remission group was similar (55.2% women). Interestingly, significantly more ACPA-positive patients who flared were women (50.0% women vs 83.3%, p=0.013).
Baseline characteristics of patients sustaining remission or relapsing
Predictors for disease relapse
We next performed a multivariate logistic regression model to define predictors for disease relapse in patients with RA in remission. In a model containing demographic variables (age, sex), autoantibody status (RF, ACPA), remission status (ACR/EULAR Boolean remission) and other disease-specific variables (disease duration, remission duration, biological DMARD exposure), only ACPA positivity (Wald χ2=4.3, p=0.038, OR=5.23) and treatment reduction in comparison to continuation as reference (arm 2: Wald χ2=6.3, p=0.012, OR=5.74, arm 3: Wald χ2=8.8, p=0.003, OR=8.78) were identified as predictors for subsequent relapse of disease (table 3). Female sex showed a tendency for prediction of relapses though not being statistically significant (Wald χ2=2.9, p=0.089). The remaining characteristics including fulfilment of Boolean remission criteria did not significantly contribute to prediction quality of the model. Overall correct case classification rate of the model was 71.6%. A post hoc power analysis of the current findings for the weakest significant predictor in multivariate logistic regression (ie, ACPA) suggests a power of 80.3% upon end of the trial. Similar results were generated with an alternative multivariate logistic regression model where Boolean remission criteria were replaced by baseline ESR since there was no additive value for this parameter in the first model (see online supplementary table S3).
Results of multivariate logistic regression for prediction of relapse
The role of ACPA in disease relapse is also shown in online supplementary figure S1, indicating that remission patients with negative ACPA showed rather low prevalence for relapse independent whether treatment was continued, tapered or stopped. In contrast, ACPA-positive patients in remission showed a gradual increase of relapse rates with respect to study arm allocation, suggesting significance for arm 3 (χ2(1)=6.45, p=0.018) in a bivariate setting comparing loss of remission to ACPA status.
Discussion
RETRO addresses a novel and growing challenge in RA: due to better treatment, more patients experience disease remission, raising the question whether medication has to be continued lifelong or can be tapered or stopped. Although remission describes a state with no or very minor disease, it cannot be seen as homogeneous state. Most importantly, remission covers two fundamentally different situations, effective suppression of inflammation and cure, which are hardly distinguishable but differ in their likelihood for disease relapse when treatment is stopped. To answer this important question, strategy studies on tapering and stopping antirheumatic therapies in remission patients are of seminal importance.21–24
Tapering and stopping DMARDs becomes an increasing issue for patients and physicians the longer the remission lasts. In the RETRO cohort, mean duration of remission was clearly >1 year, suggesting highly stable remission. Nonetheless, 15% of the patients continuing full-dose DMARDs lost their remission state, indicating that even ‘stable’ remission is not an entirely fixed condition. The fraction of patients with a DAS28 of >3.2, however, was only 5.6%. This situation has to be seen in light of the strict inclusion of the patients requiring stable DAS28 remission of at least 6 months. The overall relapse rate in patients with RA in remission after tapering or stopping antirheumatic treatment was significantly higher (44%) than in patients continuing therapy. Although higher relapse rates were expected, data also showed that more than half of the patients with RA could successfully taper or stop their treatment. Two-thirds of relapses occurred within the first 6 months, suggesting that appropriate dosing of the DMARD mono therapy or combination therapy was seminal for maintaining remission.
No randomised controlled trials with the primary aim to taper and stop antirheumatic treatment in patients with RA in remission have been carried out to date. RETRO was designed to improve decision making in sustained remission of RA by defining relapse rates and finding predictors for relapse. Thereby, RETRO was applied in all patients with RA irrespective of their previous treatment and tapering was done with all DMARDs used by the individual patient. The later, in the year 2013, published EULAR recommendations for the treatment of RA proposed that tapering of DMARDs should follow a sequential order with glucocorticoids first, followed by biological and then conventional DMARDs.16 However, this part of the recommendations is not based on randomised controlled studies comparing different strategies of tapering and stopping these drugs. In fact, such studies are essentially needed to improve these recommendations. Our approach tapering all drugs by 50% was chosen because it is pragmatic, reflects patients’ demands and attributes to the principal question of patients and physicians whether RA is only suppressed by drug therapy or whether it is actually cured.
Previous observational studies addressing tapering and stopping DMARDs have focused on withdrawal of TNF inhibitors7–11 ,13–15 or have studied the subpopulation of patients with early arthritis.13–15 ,24 ,25 Tanaka and colleagues withdrew the TNF inhibitor infliximab in patients with established RA in low-disease activity.9 Of the 81% of patients in clinical remission at baseline, 47% remained in remission after 1 year. Despite this very different approach (i) focusing on a selected therapy, (ii) leaving the patients on methotrexate treatment and (iii) using low-disease activity rather than remission as the key outcome parameter, relapse rates are stunningly similar. Furthermore, data from the BeSt and Leiden Early Arthritis Clinic cohorts suggested that drug-free remission is preferentially seen in the absence of ACPA.25–27 Indeed, ACPA were the main factor determining the risk for relapse in our study. ACPA precede the onset of RA,28 are associated with more severe disease29 and trigger pathological changes even in the absence of RA.30–32 Hence, the presence of ACPA in patients with RA in remission may indicate an underlying autoimmune process hampering successful treatment withdrawal.
Several other factors can be considered as predictors for disease relapse. One of the factors is remission quality: in this cohort, 77.2% of patients fulfilled ACR/EULAR Boolean remission criteria, indicating deep remission in the majority of patients. ‘Deep’ remission, however, was not predictive for remaining in remission after treatment tapering in our study. In the specific case of TNF inhibitor withdrawal, however, remission depth may affect disease relapses, as Tanaka and colleagues have suggested.8 Hence, data from the HONOR study investigating withdrawal of adalimumab indicated that patients with a lower DAS28 (≤1.98) remained in low-disease activity more frequently than patients with a higher baseline DAS28 (1.98–2.6).8 Interestingly, also longer disease duration and the use of biological DMARDs, suggestive of a more resistant phenotype of RA, did not predict a higher relapse rate in our study.
Strengths of the study are its real-life setting with applicability to the vast majority of patients with RA, its design as a prospective randomised controlled trial and its rigorous focus on patients in stable remission. One limitation is the lack of radiographic data, which leaves the possibility that residual disease activity could induce structural damage, although we think that such effects, if existent, are at best small. Furthermore, the lack of blinding to the study arms could have influenced outcomes, but has not been feasible in such context. Also, despite baseline characteristics being very evenly distributed, small differences in disease duration and methotrexate use were found between the study arms, but none of them was consistently present between the continuation and the two tapering arms. Finally, we cannot exclude that additional patients experience disease relapses after 12 months.
In summary, the RETRO study gives a new perspective in managing patients with RA having reached stable disease remission. It suggests that tapering and even stopping antirheumatic treatment is feasible and permits more than half of the patients to maintain remission over 1 year. Nonetheless, caution should be undertaken in patients with ACPA showing a higher risk for relapse.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
Contributors JH, MR, AK, BM, H-PT, SK, MF, MF, KM, WO, MS-H, JW, FS, MR, H-ML, HN, RA, WD and JH collected and analysed the data. SF, AJH, JR and GS designed the study. ME performed statistical analyses. JH, JR and GS wrote the manuscript.
Funding This study was supported by the Deutsche Forschungsgemeinschaft (SPP1468-IMMUNOBONE), the Bundesministerium für Bildung und Forschung (BMBF; project METARTHROS), the Marie Curie project OSTEOIMMUNE, the TEAM and MASTERSWITCH projects of the European Union and the IMI funded project BTCure.
Competing interests None.
Patient consent Obtained.
Ethics approval Ethic committee of the Friedrich-Alexander-University of Erlangen-Nuremberg and local ethic committees of the external centres as well as the Paul Ehrlich Institute (PEI) and was conducted according to the ethical principles of the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.