Article Text

Abstract
Question Which is the best strategy to achieve (drug-free) inactive disease in juvenile idiopathic arthritis (JIA)?
Methods In a randomised, single-blinded, study in disease-modifying anti-rheumatic drug (DMARD)-naive patients with JIA, three treatment-strategies were compared: (1) sequential DMARD-monotherapy (sulfasalazine or methotrexate (MTX)), (2) combination therapy MTX + 6 weeks prednisolone and (3) combination therapy MTX +etanercept. Treatment-to-target entailed 3-monthly DMARD/biological adjustments in case of persistent disease activity, with drug tapering to nil in case of inactive disease.
After 24 months, primary outcomes were time-to-inactive-disease and time-to-flare after DMARD discontinuation. Secondary outcomes were adapted ACRPedi30/50/70/90 scores, functional ability and adverse events.
Results 94 children (67 % girls) aged median (IQR) 9.1 (4.6–12.9) years were enrolled: 32 in arms 1 and 2, 30 in arm 3. At baseline visual analogue scale (VAS) physician was mean 49 (SD 16) mm, VAS patient 53 (22) mm, erythrocyte sedimentation rate 12.8 (14.7), active joints median 8 (5–12), limited joints 2.5 (1–4.8) and Childhood Health Assessment Questionnaire score mean 1.0 (0.6).
After 24 months, 71% (arm 1), 70% (arm 2) and 72% (arm 3) of patients had inactive disease and 45% (arm 1), 31% (arm 2) and 41% (arm 3) had drug-free inactive disease. Time-to-inactive-disease was median 9.0 (5.3–15.0) months in arm 1, 9.0 (6.0–12.8) months in arm 2 and 9.0 (6.0–12.0) months in arm 3 (p=0.30). Time-to-flare was not significantly different (overall 3.0 (3.0–6.8) months, p=0.7). Adapted ACR pedi-scores were comparably high between arms. Adverse events were similar.
Conclusion Regardless of initial specific treatments, after 24 months of treatment-to-target aimed at drug-free inactive disease, 71% of recent-onset patients with JIA had inactive disease (median onset 9 months) and 39% were drug free. Tightly controlled treatment-to-target is feasible.
Trial registration number 1574.
- juvenile idiopathic arthritis
- treatment-to-target
- treatment strategy study
- inactive disease
Statistics from Altmetric.com
Introduction
Juvenile idiopathic arthritis (JIA) is the most common autoimmune disease in children.1 In recent years, earlier introduction of conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) and the development of biological (b)DMARDs have improved the outcome for patients with JIA,2–4 but ongoing inflammation in JIA may still cause functional disability and joint damage.5 Early inactive disease may be the optimal therapeutic target.6–10 Studies in JIA support the window of opportunity hypothesis when the disease is optimally responding to treatment and chronicity may be prevented.10–14
Once inactive disease is achieved, discontinuation of treatment might be possible.15–19 Comparative drug studies have shown that initial treatment with csDMARD results in less rapid response than initial treatment including glucocorticoids or a bDMARD,10 20 but the latter two have not been directly compared. If the initial treatment is not effective, subsequent treatment adjustments should still aim at achieving the treatment target. In adults with rheumatoid arthritis, such targeted therapy has been proven effective in long-term prevention of damage progression and maintaining functional ability, even irrespective of initial treatment success.21–23 In JIA, continuous treatment-to-target therapy in a tight control setting, with treatment adjustments based on frequent evaluations of disease activity, has not yet been studied. Recent recommendations agree that treatment-to-target should be implemented in daily practice.24
The aim of the BeSt (acronym for Dutch ‘treatment strategies’) for Kids study was to investigate which of three treatment-to-target strategies, using treatment-to-target aimed at inactive disease, is most effective and safe. Here, we report the results of one of the first treat-to-target study in patients with recent-onset JIA.
Methods
Patients
Patients, 2–16 years, with new-onset (oligoarticular, juvenile psoriatic arthritis or rheumatoid factor (RF)-negative polyarticular) JIA, without previous DMARD therapy and symptom duration <18 months were eligible. RF-positive patients with JIA were excluded because monotherapy might be inappropriate for this severe category. Also the number was too low to stratify. Uveitis at enrolment was an exclusion criterion. Rest of the exclusion criteria are summarised in online supplementary file 1.
Supplemental material
Study design and medical intervention
The BeSt for Kids study is an investigator-initiated multicentre randomised study with 2 years of follow-up. To minimise the risk of bias of the open design, all outcome measurements were assessed by trained research nurses, physiotherapists and physicians who remained unaware of the allocated treatment strategy during entire study period (single-blind design). The trial was registered in the Dutch Trial Register, number 1574.
Patients were enrolled starting October 2009 to April 2014 by diagnosing paediatric rheumatologists. Randomisation was by variable block, stratified per centre and per oligoarticular or polyarticular disease, into three strategy arms: (1) initial treatment with csDMARD monotherapy (methotrexate (MTX) or sulfasalazine (SSZ) if preferred by treating physician); (2) initial treatment with MTX and 6 weeks of tapered prednisolone (‘bridging therapy’); and (3) initial treatment with MTX and etanercept. For all arms, the treatment protocol described a number of subsequent treatment steps in case patients failed to fulfil treatment targets (figure 1 and online supplementary file 2).
Supplemental material
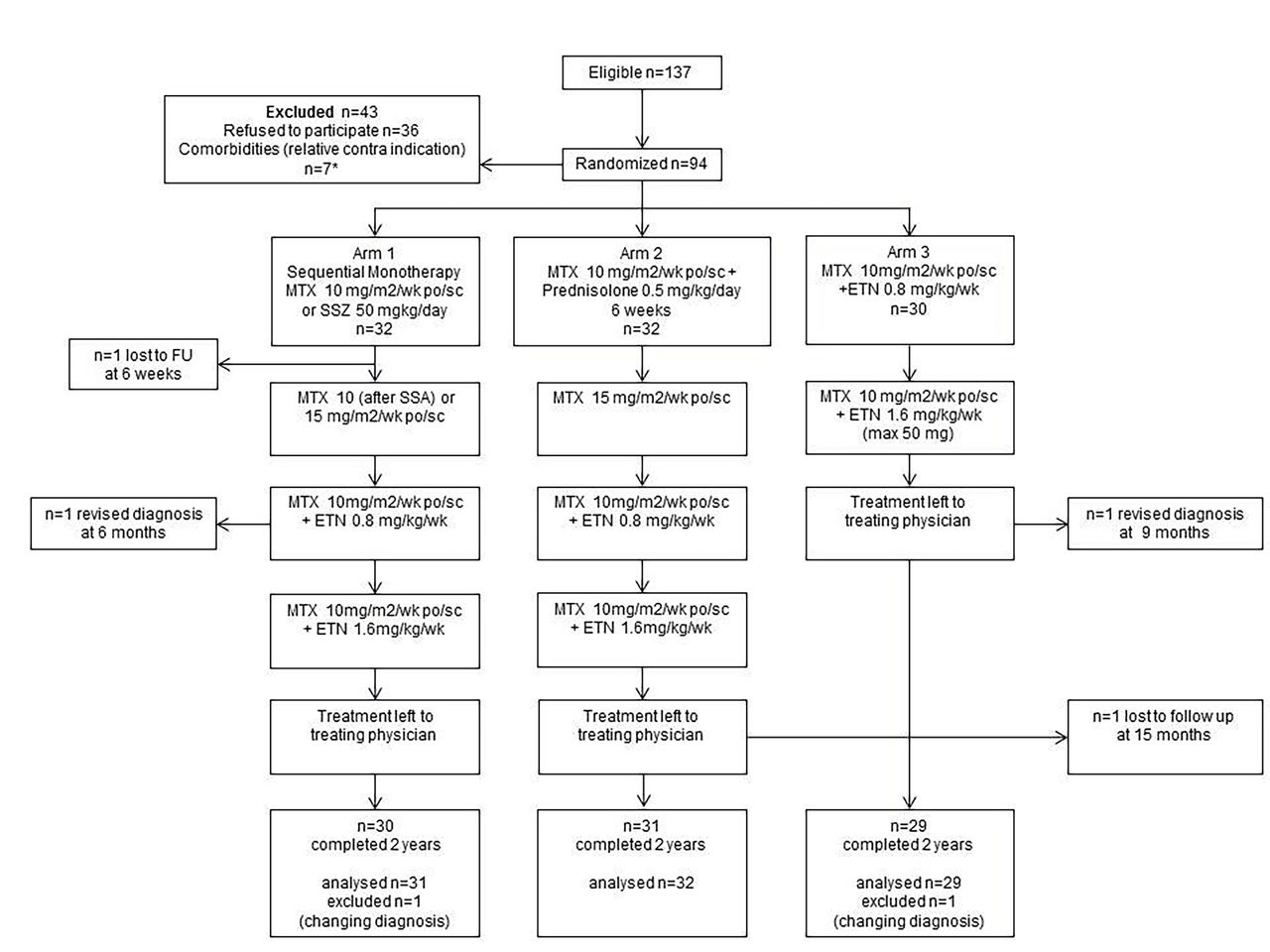
Flow diagram of the three treatment strategies compared in the BeSt for Kids study. Revised diagnosis were localised scleroderma with arthritis (arm 1) and polyarteritis nodosa (arm 3).32 See 'Patients and methods’ section for description of treatment groups. n=21 patients had ≥18 months of complaints’ duration at first consultation, n=7 had comorbidities considered (relative) contraindication for the DMARD therapy by either the paediatric rheumatologist or reason for (parents of) patients to refuse participation. These were morphea (one patient), morbid obesity (n=1), hashimoto thyreoiditis (n=1), type 1 diabetes (n=1) and previous uveitis (n=3). DMARD, disease-modifying anti-rheumatic drug; ETN,etanercept; MTX, methotrexate; po, orally; sc, subcutaneous; SSZ, sulfasalazine.
In case of side effects, the responsible drug was reduced to the lowest tolerated dose, but if it was not tolerated at all or contraindicated, patients on monotherapy proceeded to the next step in the allocated treatment group, and patients on combination therapy continued with the other drug of the combination. Additional treatment with non-steroidal anti-inflammatory drugs (NSAIDs) and intra-articular injections with glucocorticoids were permitted without a maximum and registered per strategy. All patients on MTX received folic acid 5 mg/week. The use of DMARD or oral glucocorticoids was only permitted as dictated by the protocol. All protocol violations were recorded.
After 3 months of treatment, the initial target was an adjusted ACRPedi50%, calculated as described previously25 (online supplementary file 3) and scored by a research nurse or physiotherapist who remained blinded to the allocated treatment group during the entire study period. Treatment was continued if this target was met, escalated according to protocol if not.
Supplemental material
After 6 months of treatment, the treatment target was inactive disease, defined according to Wallace 2004 criteria26 (online supplementary file 3) modified by Physicians Global Assessment<10 mm indicating no disease activity.
In all three arms, in case of inactive disease for at least three (oligoarticular disease) or six (polyarticular disease) consecutive months, DMARD(s) were tapered and stopped. In case of combination therapy, first etanercept was tapered to once per 2 weeks, only once, directly followed by 50% dose reduction, then stopped. On the same requirements, MTX or SSZ dose was reduced with 25% per week to zero. Following tapering strategies (online supplementary file 4) , in case of a disease flare, defined by recurrence of arthritis (online supplementary file 5), the last discontinued drug and/or the last effective dose was reintroduced. By protocol, prednisolone could not be restarted, and etanercept could be restarted but not discontinued for a second time.
Supplemental material
Supplemental material
Outcomes and analyses
Primary outcome measures are time-to-inactive disease and time-to-flare after tapering and stopping all DMARD therapy. Time-to-flare was defined as the time between first moment of drug-free inactive disease (DFID) and the first arthritis judged as flare by the treating physician (online supplementary file 5). Secondary outcome measures were adjusted ACRPedi30/50/70/90 scores, adverse events and functional ability. The Juvenile Disease Activity Score (JADAS)−10 score, JADAS-minimal disease activity (JADAS-MDA) and JADAS-inactive disease (JADAS-ID) were calculated as described previously (online supplementary file 6).27 28 Functional ability was determined by the Childhood Health Assessment Questionnaire (CHAQ).29 Side effects were registered through open-end interviewing at each study visit combined with incidental reports in the intervals, and routine safety laboratory tests at each study visit (complete blood count, serum liver transaminases and creatinine). Severe adverse events (SAEs) were defined as any adverse reaction resulting in any of the following outcomes: a life-threatening condition or death, significant or permanent disability, malignancy and (prolonged) hospitalisation.
Supplemental material
Sample size calculations
Percentages of time-to-inactive disease were estimated since literature in 200813 30 31 reported only on non-DMARD-naive patients with JIA.
After 3 months of therapy, an estimated difference of 10% inactive disease in arm 1 versus 60% in arm 3 could be detected with two groups of 30 patients by two-sided log-rank test (α=0.05) with power >90% assuming an HR of 8.70, a drop-out rate of 20% and 20% not treated according to initial treatment protocol. For an assumed HR of 4.11, with follow-up 2 years, a drop-out rate of 20%, a percentage not treated according to initial protocol of 20%, an alpha 0.05, a two-sided log rank test, two groups of 45 patients would be needed. The differences between arms 1 and 2 could be detected with two groups of 54, with a power of 80%, assuming a drop-out rate of 10% and no patients not treated according to initial protocol (HR=2.12). Initially 60 patients per arm was aimed for. Due to slow inclusion rate, the study protocol was amended in 2012 to include three groups of 30 patients, leaving potentially enough power to compare arm 1 versus arm 3.
Statistical methods
Multiple imputation using package mice in software package R (V.3.4.0, http://r-project.org) was used to deal with missing values with n=10 imputed data sets. Imputation variables were gender, age at inclusion, duration of symptoms, ANA positivity, diagnosis, number of affected joints and all outcome variables. In case of drug-free clinically inactive disease, often intentionally no blood was drawn causing non-random missing erythrocyte sedimentation rate (ESR), and here ‘0’ was imputed for analysis of inactive disease.
Where measured repeatedly, measurements were treated as separate variables (wide format). Student’s t-test was used to compare continuous normally distributed variables between groups. Non-parametric Kruskal-Wallis tests were used otherwise. For dichotomous variables, Pearson’s Χ2 test was used. A two-tailed probability value of <0.05 was considered statistically significant. P values were not adjusted for multiple statistical tests. Time-to-inactive disease and time-to-flare was evaluated using log-rank test. The comparison of the groups over time in reaching aACRPedi 30/50/70/90, JADAS-10 and CHAQ-score was analysed by generalised estimation equation models for continuous outcomes with time-by-strategy interaction as variable of interest. The third arm was treated as reference arm since we hypothesised that arm 3 would be superior compared with arm 1 or arm 2, based on previous results.12 21
Results
Patient characteristics
Baseline demographics and disease characteristics are summarised in table 1. Figure 1 summarises the study in a flow diagram. Ninety-four patients were randomised to one of three treatment groups: 32 patients were assigned to initial monotherapy (arm 1), 32 patients to initial combination of MTX with 6 weeks prednisolone-bridging therapy (arm 2) and 30 patients to arm 3, initial combination of MTX/etanercept. Median symptom duration was 7.5 (IQR 5–12.5) months and median duration between diagnosis and inclusion was 6 (IQR 3–14) weeks. During follow-up two patients left the study because of revised diagnosis, one patient with localised scleroderma (in arm 1) and one (arm 3) with polyarteritis nodosa.32 They were left out of further analyses. Two patients who were lost-to-follow-up, one in arm one after inclusion and one in arm 2 after 15 months, were included in the intention-to-treat (ITT) analysis.
Baseline demographic and disease characteristics*
Median time-to-inactive disease was 9.0 (5.3–15.0) months in arm 1, 9.0 (6.0–12.8) months in arm 2 and 9.0 (6.0–12.0) months in arm 3 (overall 9.0 (6.0–12.0) months (log-rank test p=0.3)). After 1 year 54% of patients in arm 1, 47% in arm 2% and 62% in arm 3 were in inactive disease (figure 2).

Clinical outcomes after 24 months: adjusted ACRPedi30/50/70/90, inactive disease, CHAQ and JADAS-10 score, based on generalised estimating equations (GEE) analyses on imputed data. Error bars indicate 95% CIs. Adjusted ACRPedi30/50/70/90=30/50/70/90% improvement according to adjusted American College of Rheumatology Pediatric response criteria. CHAQ, Dutch version of the Child Health Assessment Questionnaire; JADAS-10, juvenile arthritis disease activity score up to maximum of 10 joints; MTX, methotrexate.
During 24 months 59% (19 (3 oligo)/31 (61%) of patients in arm 1, 16 (1 oligo)/32 (50%) in arm 2 and 19 (1 oligo)/29 (65%) in arm 3) had tapered and stopped all DMARDs (DFID), after median 15.0 (IQR 12.0–18.0) months (arm 1), 19.5 (12.0–24.0) months (arm 2) and 18.0 (12.0–21.0) months (arm 3) of therapy. However, 26% (6 (one oligo) patients in arm 1, 3 in arm 2 and 5 in arm 3) subsequently had to restart treatment before the end of the study, in arm 1 median after 4.5 (3.0–9.0) months, in arm 2 after 3.0 (3.0–3.0) months and in arm 3 after 3.0 (3.0–7.5) months (overall 3.0 (3.0–6.8) months (p=0.7)). Three months later, inactive disease was regained by 10/14 (71%) (six in arm 1, one in arm 2 and three in arm 3). After 24 months, 71% (arm 1), 70% (arm 2) and 72% (arm 3) of patients had inactive disease and 45% (arm 1), 31% (arm 2) and 41% (arm 3) had DFID.
Adjusted ACRPedi30/50/70/90, JADAS-10 and CHAQ score
Adjusted ACRPedi-scores were reached in similar high percentages over time in all three arms (figure 2 and online supplementary table S1) JADAS-10 scores after 24 months improved comparably (figure 2), JADAS MDA and ID-criteria are given in online supplementary table S3. Overall, flares were characterised by a JADAS-10 of 9.7 (8.1–11.3), which improved 3 months after restart of treatment to JADAS-10 of 3.9 (1.8–6.0). In all three arms, CHAQ values improved from mean 1.0 (SD 0.6) to 0.5 (0.6).
Supplemental material
Supplemental material
Medication changes and protocol violations
Figure 3 shows all medication actually used in the study per arm (ie, including protocol violations). In arm 1, treating physicians prescribed SSZ (n=15) almost as often as MTX (n=17). By t=3 months 10/15 patients had switched from SSZ to MTX, two due to side effects, 8 because of insufficient response. After 3 months, patients who remained on SSZ had similar ACRPpedi50% scores as patients who started on MTX (data not shown). During 24 months in arm 1, nine patients in arm 1 reached inactive disease while still on monotherapy, four on initial SSZ (one flared later) and five on initial MTX (three flared later). In arm 2 (17/32), 53% of patients who started on MTX plus 6 weeks of prednisolone switched to MTX with ETN before end of year 1. Overall 17 patients (55%) in arm 1 and 23 patients (72%) in arm 2 progressed to a biological, at various time points, according to protocol. Treatment was left to treating physician due to end of protocol in four patients in arm 1, versus 15 and 18 in arms 2 and 3. In arm 3 significantly less treatment adjustments were needed to achieve first inactive disease: 0.6 (0.3–1.0) treatment steps compared with 1.4 (0.9–1.8) steps in arm 1 and 1.5 (1.0–1.9) steps in arm 2 (p=0.011). Across all arms, 10 (two in arm 1, two in arm 2, six in arm 3) patients failed to achieve inactive disease on ETN and switched to adalimumab (9) or infliximab (1). After 24 months, 5 of these 10 patients gained inactive disease on the second anti-tumour necrosis factor.
Online supplementary table 2 summarises protocol violations including outside of protocol glucocorticoid use across the three arms. Incorrect glucocorticoid treatments were given in the first months in arm 1 (three times) and in arm 2 (four times) compared with none in arm 3. Overall, treatment was not escalated according to protocol in all three arms for refusal to start or increase the dose of MTX or etanercept (Online supplementary table 2).
Supplemental material

{kind=link}
{kind=link}
{kind=link}
Treatment of patients during 2 years of follow-up. Treatment was started and when necessary adapted to reach inactive disease. Within the first year of therapy more treatment changes occurred in arms 1 and 2 compared with arm 3. When inactive disease was reached for a consecutive period of 3 months in case of oligoarticular disease, and 6 months for polyarticular disease, all disease-modifying anti-rheumatic drugs where tapered and stopped according to protocol within approximately 2 months.
Adverse events
Adverse events (AEs) were similar across the arms. AEs are summarised in table 2. AEs were mild in general and involved mostly gastrointestinal complaints, upper respiratory tract and other infections and general malaise. One patient in arm 1 while on MTX developed de novo uveitis anterior after 6 months of treatment. No patients had permanent sequelae.
Adverse events in 92 patients with juvenile idiopathic arthritis (JIA) in three treatment arms: sequential monotherapy, combination therapy methotrexate (MTX)/prednisolone and combination therapy MTX/etanercept
Discussion
This is one of the first treatment-to-target studies, tightly controlled and single-blinded, in newly diagnosed DMARD-naive patients with JIA, aiming at inactive disease. Efficacy and safety of three treatment strategies were compared that are frequently used and comparable with the Childhood Arthritis and Rheumatology Research Alliance American Consensus Treatment Plans.33 Abrogation of inflammation by treating JIA to target has recently been recommended.24 Our results show that after 24 months inactive disease was achieved by >70% of patients, irrespective of initial treatment, including tapering and stop strategies. Fifty-nine per cent achieved DFID, although early flares occurred that were successfully retreated.
After 3 months of treatment, more patients who started with MTX and etanercept (arm 3) had achieved rapid improvement as determined by aACRPedi70scores,34 but time-to-inactive disease was similar across the arms. Due to treatment adjustments in case of active disease, which were needed more often in arms 1 and 2 than in arm 3, aACRpedi improvement scores were met in similar percentages of patients over time across the arms. After 24 months of treatment-to-target JADAS-10-scores were considerably reduced and functional ability as assessed by CHAQ was lowered substantially across the arms.
Our results show higher percentages of patients achieving inactive disease than in the prospective randomised double-blinded TREAT-study10 which included only polyarticular patients with JIA (n=85) including 30%–40% RF positives. In the ACUTE-JIA study (n=59), 68% achieved inactive disease after 1 year in the infliximab arm.20 This unblinded study allowed one treatment intensification step but did not include tapering or stop strategies. In the daily practice-based ReACCh-out-cohort,35 polyarticular and oligoarticular JIA achieved inactive disease after 24 months in 71% and 86% mainly by additional glucocorticoid use.
The current study also aimed at systematically tapering and discontinuing treatment when inactive disease was achieved. DFID was achieved by 54/92 (59%) of all patients, although in 14 patients (six (one oligo) in arm 1, three in arm 2 and five in arm 3), flares occurred, requiring restart of treatment, resulting in overall 39% of patients still in DFID at the 2 years end point. Time-to-flare was similar across the arms. Overall flare rates (26%) were lower than 37%–60% mentioned in previous cohorts16 17 36 37 which may also depend on our limited total follow-up period of 24 months.
Contrary to previous studies we included oligoarticular patients (n=11) because they can have substantial disease burden and adverse outcomes,38 but used a rapid drug-tapering scheme (tapering and stopping medication after 3 months of inactive disease compared with after 6 months in polyarticular disease) as we hypothesised that DFID could be achieved earlier in patients with less inflamed joints. We could not establish this difference significantly, possibly due to low numbers. Only one oligoarticular patient out of five who achieved DFID flared. These limited results suggest that oligoarticular JIA patients could benefit from a treatment-to-target strategy.
There are several limitations to our study. First, the sample size, which may obscure differences between groups that in a larger population might have become clear. This can be explained by rarity of the disease, delays in referral (21 patients had ≥18 months symptom duration at the first consultation), comorbidities preventing DMARD use (seven patients) and reluctance of parents to enrol their children in a clinical trial. Data on the clinical course of non-participating patients receiving ‘routine care’ are currently not available. Recent retrospective studies in polyarticular JIA showed that despite achieving inactive disease for some time most patients had active disease during follow-up.5 39 40 Second, this study was performed in a single-blinded setting, with the clinical assessors remaining unaware of the treatment received. Third, there was a relatively high frequency of protocol violations or intra-articular injections. (Not allowed) glucocorticoid treatments were given in the first months in arms 1 (three times) and 2 (four times) compared with none in arm 3. These findings may indicate that the clinical efficacy of treatment in arm 3 was better, and that with less effective csDMARDs, additional glucocorticoid courses are required to achieve similar results. These protocol violations suggest that physicians at least tried to follow the treatment-to-target approach. However, in a larger number of patients across the three arms the physicians did not follow protocol for various reasons, mainly reluctance to intensify therapy based on shared decision-making.24
Based on the results from our study, we conclude that DFID is a feasible goal in treatment of children with JIA, as was recently recommended,24 resulting in >70% achieving inactive disease and 39% stopping all DMARDs after 24 months. In addition, we showed that tapering and discontinuation of treatment is a realistic goal. On the other hand, treatment-to-target resulted in a relatively high use of bDMARDs,>50% of patients in all arms. The AEs were nonetheless mostly mild, as previously reported.41 Long-term follow-up of the BeSt for Kids cohort, including radiology results, is initiated to investigate possible lasting positive results of treatment-to-target in JIA.
Supplemental material
Acknowledgments
The authors thank all participating patients and parents as well as the following physiotherapists and research nurses: Ingrid Honkoop AMC, Annette Hummelman-van Dijk SKZ. Susan Moors physiotherapist SKZ, Jacqueline Bouts, LUMC, Piroska de Boer, LUMC, Veronique van de Lugt, ARC-Reade.
References
Footnotes
Handling editor Josef S Smolen
Contributors All authors were involved in drafting the article or revising it critically for important intellectual content. All authors approved the final version to be published. HM had full access to all data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study conception and design: DMCB, CFA, RtC, LWAvS-S, MVR. Acquisition of data: PHM, DMCB, DS-M, Y-KK, JMvdB, TWK, ICJB, PWB, MVR, LWAvS-S, CFA, RtC. Analysis and interpretation of data: PHM, JMvdB, SB, DMCB, LWAvS-S, CFA, RtC. Critically revising the manuscript; DMCB, DS-M, YK-K, IB, WBvdB, WPB, TWK, MAJvR, LWAvS-S, JMvdB, CFA, RtC.
Funding This is an investigator-initiated study which received financial support from Pfizer, who had no role in study design, data collection, data analysis, data interpretation, writing of an abstract, or decision to submit a manuscript for submission.
Competing interests None declared.
Ethics approval Approval of the Medical Ethical Committee of the Leiden University Medical Center and local Ethical Committees was obtained prior to start at each study site.
Provenance and peer review Not commissioned; externally peer reviewed.
Data statement The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.