Article Text

Abstract
Objective: To compare patient reported measures of function, health related quality of life (QoL), and satisfaction with medication among patients with rheumatoid arthritis (RA) treated with methotrexate (MTX), etanercept, or both for up to 1 year.
Methods: In a 52 week, double blind, clinical trial, patients with active RA were randomised to receive etanercept 25 mg twice weekly, methotrexate up to 20 mg weekly, or combination therapy. The Health Assessment Questionnaire (HAQ) disability index, EuroQoL health status visual analogue scale (EQ-5D VAS), patient global assessment, and patient general health VAS were administered at baseline and weeks 2, 4, 8, 12, 16, 20, 24, 32, 40, 48, and 52. Satisfaction with the medication was compared at 52 weeks.
Results: Of 682 enrolled patients, 522 completed 52 weeks of treatment. Mean improvement from baseline in HAQ score was 0.65, 0.70, and 1.0 for MTX, etanercept, and the combination, respectively. The mean percentage and absolute improvement in the HAQ was significantly higher (p<0.01) for combination therapy than for either of the monotherapies. Combination therapy produced significantly more rapid achievement of HAQ ⩽0.5 sustained for 6 months than either of the monotherapies (p<0.01). Compared with patients receiving monotherapy, those receiving combination therapy achieved a significantly better (p<0.05) health state as measured by the EQ-5D VAS (mean (SD) 63.7 (3.2), 66.8 (3.2), 72.7 (3.1) for MTX, etanercept, and the combination, respectively). Results were similar for other assessments (p<0.01). Patients in combination and etanercept groups were significantly more likely (p<0.0001, p = 0.0009, respectively) to report satisfaction with the medication.
Conclusions: Combination therapy with etanercept and methotrexate improved function, QoL, and satisfaction with the medication significantly more than monotherapy.
- ACR, American College of Rheumatology
- AUC, area under the curve
- CI, confidence interval
- DAS, Disease Activity Score
- DMARDs, disease modifying antirheumatic drugs
- EQ-5D VAS, EuroQoL health status visual analogue scale
- GHVAS, general health assessment on a visual analogue scale
- HAQ, Health Assessment Questionnaire
- LOCF, last observation carried forward
- MTX, methotrexate
- QoL, quality of life
- PGAD, patient global assessment of disease activity
- PRO, patient reported outcome
- RA, rheumatoid arthritis
- TEMPO, Trial of Etanercept and Methotrexate with Radiographic Patient Outcomes
- rheumatoid arthritis
- etanercept
- methotrexate
- functional status
- disability
- patient outcome assessment
- quality of life
Statistics from Altmetric.com
- ACR, American College of Rheumatology
- AUC, area under the curve
- CI, confidence interval
- DAS, Disease Activity Score
- DMARDs, disease modifying antirheumatic drugs
- EQ-5D VAS, EuroQoL health status visual analogue scale
- GHVAS, general health assessment on a visual analogue scale
- HAQ, Health Assessment Questionnaire
- LOCF, last observation carried forward
- MTX, methotrexate
- QoL, quality of life
- PGAD, patient global assessment of disease activity
- PRO, patient reported outcome
- RA, rheumatoid arthritis
- TEMPO, Trial of Etanercept and Methotrexate with Radiographic Patient Outcomes
- rheumatoid arthritis
- etanercept
- methotrexate
- functional status
- disability
- patient outcome assessment
- quality of life
Clinical practice guidelines for rheumatoid arthritis (RA) recommend starting treatment with disease modifying antirheumatic drugs (DMARDs) within 3 months of diagnosis to preserve function and retard joint damage.1 Although guidelines recommend methotrexate (MTX) as standard treatment, alone or in combination with another DMARD,1 recent studies comparing the human soluble tumour necrosis factor receptor etanercept with MTX have reported significantly greater clinical improvement and fewer adverse events for etanercept treatment.2,3 Furthermore, in a double blind, randomised trial in patients with active RA despite MTX treatment, addition of etanercept to MTX improved function and disease activity measures.4
No controlled and randomised study, however, has included all three treatments (MTX, etanercept, and combination therapy) to allow direct comparison of treatment efficacy in matched patient groups. The TEMPO study (Trial of Etanercept and Methotrexate with Radiographic Patient Outcomes) was designed to compare efficacy and safety of the monotherapies with combination therapy in patients with active RA. Primary clinical and radiographic outcomes of the TEMPO study have been reported separately.5 Combination therapy was significantly more efficacious than monotherapy as measured by American College of Rheumatology (ACR) response and radiographic evidence of joint damage.
This paper reports a comprehensive set of patient reported outcomes (PROs), including satisfaction with the study medication, which were included in the TEMPO study, distinct from the objective clinical and biological measures previously reported.5 There is increasing recognition of the importance of the way patients with RA feel about their disease and treatment,6 and the Bone and Joint Decade advocates greater incorporation of patient views.7 With no cure for RA yet available, a primary goal of treatment is to restore functioning in activities of daily living and improve the health related quality of life (QoL) of patients. Even in its early stages, RA significantly impairs physical and social functioning, emotional wellbeing, and vitality. To help assess disease progression and response to treatment, clinical practice guidelines recommend using measures of functional status and quality of life.1 Thus, although traditional measures such as the ACR response and radiographic evidence of joint damage remain core clinical end points in RA outcomes studies,8 it is increasingly recognised that PRO assessments are important in defining overall therapeutic effectiveness.9 No single tool exists for measuring all relevant PROs in RA, so a combination of instruments is recommended.9 It is also useful to measure patient satisfaction with treatment, which is influenced by convenience, efficacy, and side effects.6
PATIENTS AND METHODS
The PRO analyses reported here were prospectively designed secondary assessments in a 52 week, multicentre, double blind, randomised, parallel group, outpatient study conducted between October 2000 and July 2002 in 17 European nations, Australia, and Israel. Details of the study design and primary analyses have been published elsewhere.5
Patients
The TEMPO study enrolled patients of at least 18 years of age who had active RA (ACR functional class I–III) with disease duration of 6 months to 20 years. Active disease was defined as having 10 or more swollen joints, 12 or more painful joints, and at least one of the following: erythrocyte sedimentation rate ⩾28 mm/1st h, C reactive protein ⩾20 mg/l, or morning stiffness for ⩾45 minutes. Patients were also required to have experienced an unsatisfactory response to at least one DMARD other than MTX. All enrolees were considered suitable candidates for MTX treatment, had never had an unsatisfactory response to MTX, and had not received MTX in the 6 months before enrolment.
Patients were ineligible if they had been treated with any DMARD within 4 weeks before the study baseline, or if they had ever received etanercept or another tumour necrosis factor antagonist. Patients were also excluded if they had received recent treatment with investigational, immunosuppressive, or corticosteroid drugs, or had significant concurrent disease.
Subjects gave written informed consent at enrolment. The protocol received independent ethics committee approval at each participating centre. The trial was carried out in accordance with the Declaration of Helsinki, and conformed to local regulations and principles of the International Conference on Harmonisation guidelines for Good Clinical Practice (1996 revision) in the European Community.
Treatment groups
Subjects were randomly assigned to one of three treatment groups: MTX, etanercept, or combination. Patients in the MTX group received oral MTX capsules once weekly (initially 7.5 mg, increasing over 8 weeks to a maximum of 20 mg if patients still had any painful or swollen joints) and placebo subcutaneous injections twice weekly. Patients in the etanercept group received 25 mg etanercept by subcutaneous injection twice weekly and oral placebo capsules once weekly. Patients in the combination group received 25 mg etanercept subcutaneous injections twice weekly and oral MTX capsules once weekly (dosed as in the MTX group). All patients received 5 mg folic acid supplementation twice weekly.
Outcomes
Principal PRO measures were the Health Assessment Questionnaire (HAQ) disability index and EuroQoL health status visual analogue scale (EQ-5D VAS). The HAQ disability index is derived from a questionnaire comprising eight subscales: dressing, arising, eating, walking, reaching, gripping, hygiene, and carrying out common activities.10 The disability index and individual subscale scores range from 0 (without any difficulty) to 3 (unable to do). The EQ-5D VAS measures current health state on a thermometer scale, ranging from 0 (worst state of health imaginable) to 100 (best state of health imaginable).11
Additional PRO measures were a patient global assessment of overall RA activity (PGAD) and a patient general health assessment (GHVAS). A numeric rating scale ranging from 0 (none) to 10 (extreme) was used for PGAD. For GHVAS, patients reported how they felt about their arthritis on a 10 cm horizontal VAS anchored on the left at “very well” and on the right at “extremely bad”.
Patient satisfaction with the study medication was measured using a five point scale ranging from “very satisfied” to “very unsatisfied”. Responses of “very unsatisfied”, “unsatisfied”, and “neutral” were considered to indicate patient dissatisfaction, while “satisfied” and “very satisfied” indicated patient satisfaction.
This study also assessed relationships between PROs and two clinical measures of disease activity: Disease Activity Score (DAS) and DAS28. DAS is an index of disease activity that combines the Ritchie Articular Index, total number of swollen joints, erythrocyte sedimentation rate, and GHVAS.12 DAS28 is a modified version of the DAS that includes counts of painful and swollen joints for 28 joints.13
All four PRO measures were administered at baseline and weeks 2 and 4, then every 4 weeks to week 24, then every 8 weeks to week 48, with a final follow up at week 52. Patient satisfaction was measured at baseline, weeks 2 and 12, and at the final follow up. DAS and DAS28 were calculated after study completion.
Data analysis
Analyses were conducted for all the enrolled patients; to reduce bias and loss of statistical power, missing data due to study drop-out or for other reasons were imputed using the last observation carried forward (LOCF) method.14 All PRO measures (HAQ disability index, eight HAQ subscale scores, EQ-5D VAS, GHVAS, PGAD) were compared between treatment groups using the mean change from baseline and area under the curve (AUC). When the AUC approach is used, more information about the rapidity and consistency of response can be evaluated.15,16 Additionally, the AUC approach is appropriate when within-patient measurements are highly correlated over time and when changes are larger at earlier assessments. AUC end point treatment comparisons used an analysis of covariance model that included factors for study centre, treatment, and prior MTX use, with baseline HAQ score as a covariate.
Comparisons between treatment groups were also performed using least squares means (means adjusted for potential imbalance in baseline values using a model fitted by the least squares method17) and 95% confidence intervals (CIs) for EQ-5D VAS, PGAD, and GHVAS. These comparisons used an analysis of covariance model that included baseline score as a covariate and factors for study centre, treatment, and prior MTX use.
The proportion of patients within different clinically meaningful HAQ disability index categories at week 52 was compared between treatment groups using χ2 analysis. Categories compared were percentage of patients with decrease from baseline of at least 0.22 (a clinically meaningful improvement18,19), percentage of patients with decrease from baseline of >0.8 (a major improvement), and a change of >0.5 as used in other studies.3,20 In addition, treatments were compared by percentage of patients with HAQ scores of ⩽0.5 at the end of the trial, representative of scores seen in the general population.21 Treatments were also compared by the percentage of patients with EQ-5D VAS scores above 82, representing population norms.22
Rapidity of onset of action was assessed using life table statistical analysis. Kaplan-Meier methods were used to estimate the proportion of subjects with HAQ scores of ⩽0.5, sustained for 6 months, by time since randomisation. Log rank statistics were used to compare differences in survival plots among treatment groups.
The percentage of patients satisfied with the study medication at the final follow up was compared between treatment groups using χ2 analysis. Predictors of patient satisfaction were evaluated using a logistic regression model that included treatment group, age, sex, race, and satisfaction with current (pre-trial) medication at baseline. A backward elimination stepwise process was used, and only variables with p<0.20 were retained in the final model.
Pearson correlation analysis was used to assess pairwise correlations between DAS and HAQ disability score, EQ-5D VAS, GHVAS, and PGAD over 52 weeks. Similar correlation analyses were also implemented for DAS28 scores. Significance for all comparisons was defined as p<0.05. Statistical analyses were performed using SAS version 8.2.
RESULTS
All but four of 686 patients (99%) randomised to treatment groups received the study medication and were included in these analyses, and 522 (76% of those randomised) completed 52 weeks of treatment. Most patients were white and female, and their baseline characteristics did not differ significantly between treatment groups (table 1).
Baseline patient characteristics
HAQ
Figure 1 shows that subjects receiving combination therapy achieved significantly greater improvement in functional status than those receiving MTX alone from week 2 onwards, and than those receiving etanercept alone from week 4 onwards. Better response to combination therapy was sustained for the 52 week study. AUC analysis confirmed these findings. At week 52, combination therapy yielded significantly greater functional status improvements than either of the monotherapies (fig 2).

Mean improvement from baseline of patients to 52 week follow up of patients with RA receiving MTX, etanercept, or combination therapy with MTX and etanercept, as measured by the HAQ score (LOCF analysis). *,*Significant difference between etanercept and MTX at p<0.01 and p<0.05, respectively; †significant difference between combination and MTX at p<0.01; ‡,‡significant difference between combination and etanercept at p<0.01 and p<0.05, respectively.

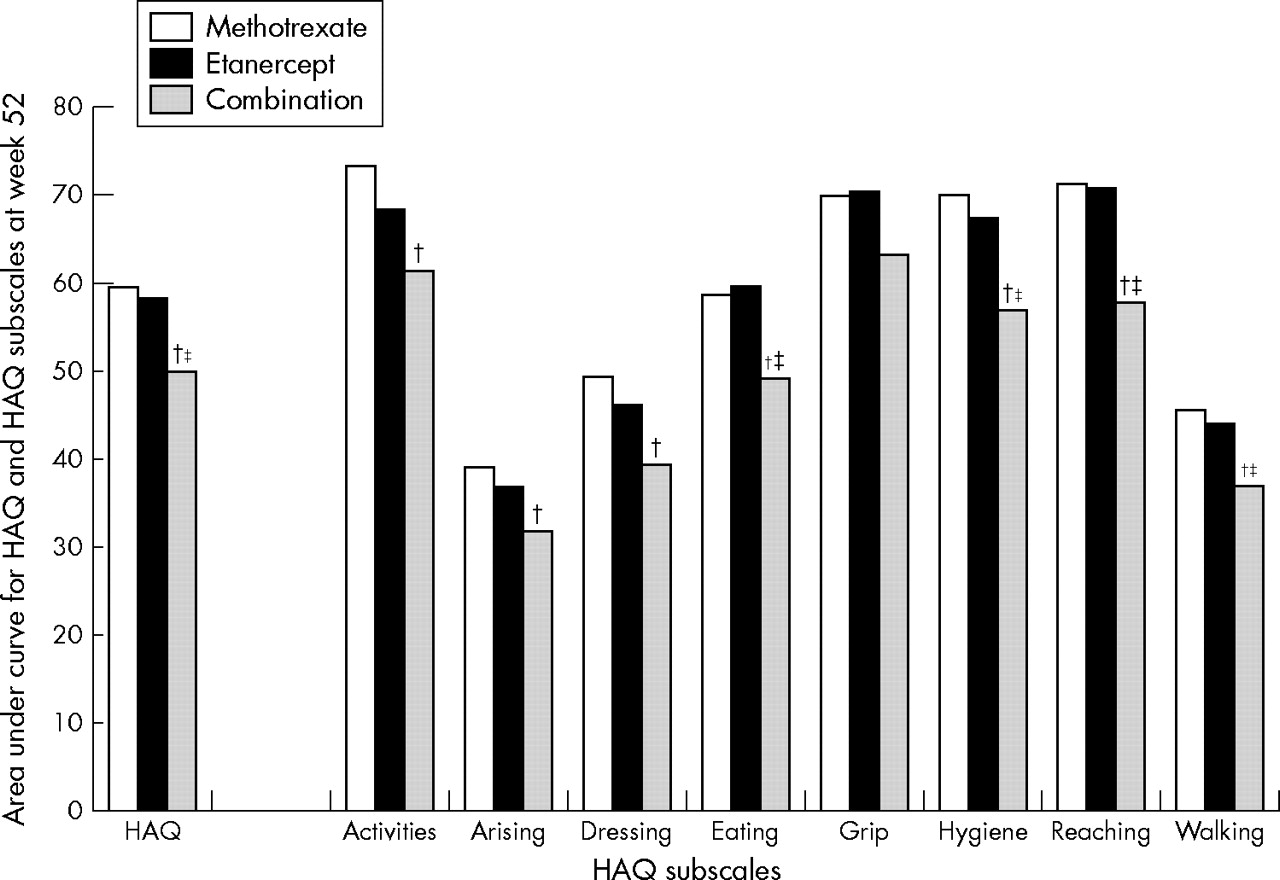
Mean improvement from baseline to 52 week follow up of patients with RA receiving MTX, etanercept, or combination therapy with MTX and etanercept, as measured by the AUC for the eight subscales of the HAQ score (LOCF analysis). †,†Significant difference between combination and MTX at p<0.01 and p<0.05, respectively; ‡,‡significant difference between combination and etanercept at p<0.01 and p<0.05, respectively.
Results for the eight HAQ subscales were consistent with those for the composite HAQ disability index. Figure 2 shows that by the final follow up patients receiving combination therapy achieved greater improvements than those receiving MTX for all HAQ subscales except grip. Significant differences were seen between combination therapy and etanercept in eating, hygiene, reach, and walking scores. No significant difference between etanercept and MTX was noted for any HAQ subscale.
Table 2 shows that by 52 weeks, combination therapy recipients were significantly more likely to attain HAQ disability index scores similar to population norms (⩽0.521) than were monotherapy recipients (p<0.05). A majority of patients in all three groups had a clinically meaningful improvement (⩾0.22), but a significantly higher proportion of combination therapy recipients than monotherapy recipients achieved this degree of improvement (p<0.05). Combination therapy and etanercept recipients were significantly more likely than MTX recipients to achieve a major HAQ disability index score improvement of >0.8 (p<0.05). However, only subjects in the combination group were significantly more likely than subjects in the MTX group to achieve an improvement of >0.5 (72% v 53%, respectively; p<0.05).
Percentage distribution of Health Assessment Questionnaire (HAQ) disability index score and EQ-5D VAS scores, by treatment group
Figure 3 shows that 27%, 26%, and 39% of patients in the MTX, etanercept, and combination groups, respectively, reached an HAQ score of ⩽0.5 and sustained it for 6 months. The overall log rank test for equality over treatment groups was highly significant (p = 0.003). Pairwise comparisons revealed that the combination treatment strategy provided significantly faster onset in achieving sustained HAQ scores of ⩽0.5 than either of the monotherapies (p = 0.002 for combination versus etanercept; p = 0.005 for combination versus methotrexate).

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier estimation of time to HAQ disability scores ⩽0.5 and sustained for 6 months.
EQ-5D VAS
Table 3 shows that EQ-5D scores improved in all three treatment groups. However, combination therapy recipients achieved significantly higher EQ-5D VAS scores (indicative of better health state) at week 52 than patients who received either of the monotherapies. By week 52, combination therapy was significantly more likely than either of the monotherapies to yield EQ-5D scores above population norms. Comparison of AUC scores also showed that combination therapy recipients had significantly greater improvement in EQ-5D VAS score than MTX patients (data not presented).
Health status at baseline and 52 weeks of patients with RA receiving MTX, etanercept or combination therapy with MTX and etanercept, as measured by least squares mean (95% CI) for EuroQol health status visual analogue scale, patient global assessment, and patient general health visual analogue scale (LOCF analyses)
Patient global assessment
Table 3 shows that combination therapy recipients reported significantly lower RA disease activity at week 52 (PGAD) than subjects receiving either of the monotherapies. Combination therapy recipients had significantly greater improvement in PGAD than MTX recipients from week 2 onwards, and than etanercept patients from week 12 onwards. Results from an AUC analysis at week 52 were similar (data not presented).
Patient general health VAS
Table 3 shows that patients who received combination therapy attained significantly lower GHVAS scores (indicating better general health) at week 52 than patients who received either of the monotherapies. Comparison of change from baseline (%) over time showed that combination therapy recipients had significantly greater improvement in GHVAS score than MTX recipients from week 2 onwards, and than etanercept patients from week 8 onwards.
Patient satisfaction with treatment
A significantly higher percentage of patients in the combination and etanercept groups were satisfied with their medication than in the MTX group (table 4). No significant difference in satisfaction with treatment was found between combination and etanercept groups. Logistic regression analysis showed that etanercept and combination therapy recipients were more than twice as likely to be satisfied with treatment as MTX recipients (table 5). There was no significant association between satisfaction with treatment at week 52 and patient sex, disease duration, or baseline satisfaction. Age and race were non-significant and were eliminated from the final model.
Patient satisfaction with RA medication by treatment group at study end point, as measured on a five point scale
Multiple logistic regression analysis of predictors of patient satisfaction with medication
Correlation between patient reported outcomes and disease activity measures
Table 6 shows that severity of disease activity correlated significantly with greater disability as measured by the HAQ disability index, and with lower health status as measured by the EQ-5D VAS, PGAD, and GHVAS. These correlations were comparable for the DAS and DAS28 indices of disease activity.
Correlation between patient reported health status measures and measures of disease activity over 52 weeks (LOCF analysis)
DISCUSSION
Combination therapy in the TEMPO study resulted in significantly greater improvements than monotherapy on all measures of PRO: functional status, QoL, and treatment satisfaction. The mean improvement in functional status among combination therapy recipients of 1.0 was significantly larger than in either MTX or etanercept groups. Kosinski et al suggested that a decrease in HAQ disability index of 0.13–0.24 may be considered clinically significant.18 This is consistent with the 0.22 unit change that Wells et al determined is perceived by patients with RA as meaningful improvement.19 The difference in HAQ disability index score at 52 weeks between combination therapy and monotherapy is therefore clinically as well as statistically significant. More importantly, by week 52, 58% of patients in the combination group achieved improvement in functional status score of >0.8, and 44% of subjects in the group had HAQ disability scores of ⩽0.5. Further, at week 52, 41% of patients in the combination group were significantly more likely to attain EQ-5D VAS scores comparable with population norms.
Patient satisfaction with medication is expected to predict drug preferences and adherence to prescription regimens,23 both of which are components of real-world treatment effectiveness. Patients in the the TEMPO study who received combination therapy or etanercept were significantly more likely than MTX recipients to report satisfaction with their medication.
Response to combination therapy diverged from the response to MTX and etanercept early in treatment and the difference was sustained for 52 weeks. Kaplan-Meier survival plots for time to occurrence of HAQ scores ⩽0.5 and sustained for 6 months confirmed the faster onset of action in the combination group than with etanercept or MTX alone. Similar trends in improvement over time were found for the EQ-5D VAS, PGAD, and GHVAS.
Additionally, these results support previous findings that PRO assessments are valid indicators of RA disease status. Table 6 shows that increasing disease activity (measured by the DAS score) is significantly correlated with greater disability as measured by the HAQ disability index, and with lower health status as measured by the EQ-5D VAS, PGAD, and GHVAS. It has been shown previously that the HAQ disability index correlates significantly with DAS scores.24
The degree of improvement in the QoL with etanercept monotherapy in the TEMPO study is consistent with previous findings. In a 26 week, double blind study comparing etanercept 10 mg or 25 mg against placebo, both etanercept doses produced significantly greater QoL improvement as assessed by the HAQ index and all HAQ subscales except grip.25,26 By 26 weeks, the HAQ index score had decreased (improved) by only 2% in the placebo group, but decreased by 39% in the etanercept 25 mg twice weekly group.25 A similar benefit was experienced by the etanercept group in the TEMPO study, with a 38% decrease from baseline in the HAQ index score at 24 weeks. On a VAS similar to the EQ-5D VAS, patients in the 26 week study receiving either of the etanercept doses reported greater QoL improvement from baseline than those reported by placebo recipients: approximately 20 points v 8 points, respectively.26 These results are comparable to EQ-5D VAS improvements in the TEMPO study, in which the mean score in the etanercept group increased by 25 points at 24 weeks and by 26 points at 52 weeks.
The finding in the TEMPO trial of no significant difference in HAQ disability index at 52 weeks between etanercept and MTX agrees with results of a previous study in patients with early RA (diagnosed no more than 3 years before study entry).27 In that study, etanercept yielded a significantly greater improvement in the HAQ eating subscale, while MTX recipients had significantly greater improvement in the dressing subscale; no significant differences were found for other subscales.
The TEMPO study included only patients judged to be appropriate candidates for MTX treatment at study enrolment, so these results may not be generalisable to different patient groups. A potential study limitation is that imputing missing PRO data by the LOCF method may introduce bias if scores change over time.14 However, analysis of the group following the protocol yields results consistent with those for the LOCF group (data not presented).
CONCLUSIONS
Combination therapy with etanercept plus MTX yielded significantly greater improvements on four PRO assessments than treatment with either agent alone. These results support findings of a previous study in which combination therapy resulted in significantly greater improvement than monotherapy with MTX on HAQ disability index and PGAD.4
Acknowledgments
We thank MA Tedeschi at Global Health Outcomes Assessment in Wyeth Research. This article was prepared with the assistance of BioMedCom Consultants Inc, Montreal, Canada.
REFERENCES
Footnotes
-
Published Online First 3 August 2005
-
Funding: Wyeth Research sponsored this trial as a post-approval commitment to the European Agency for the Evaluation of Medicinal Products. The sponsor was responsible for the collection and analysis of data. The authors and the sponsor were involved with study design, data interpretation, writing this article, and the decision to publish. The lead author and all other authors have had full access to the data and no restrictions on interpretation from the sponsor.
-
Competing interest statement: D van der Heijde has received reimbursement for symposium attendance and speaking and consulting fees from Wyeth, and has acted as an expert witness for Wyeth at an EMEA meeting for radiographic results of the TEMPO study. L Klareskog has received reimbursement for symposium attendance, speaking and consulting fees, and research funds from Wyeth. J Tornero has received reimbursement for symposium attendance, speaking fees, and research funds from Wyeth. J Melo-Gomes and C Codreanu declare no potential competing interests. A Singh, R Pedersen, B Freundlich, and S Fatenejad are employees of Wyeth and hold stock and/or stock options in Wyeth. B Freundlich has also received funds for research and staff members from Wyeth.
-
TEMPO study investigators: HD Bolosiu, Cluj-Napoca, Romania; P Bourgeois, Paris, France; J Cunha Branco, Lisbon, Portugal; J Braun, Herne, Germany; J Broell, Wien, Austria; G Bruyn, Leeuwarden, The Netherlands; J Brzezicki, Elblag, Poland; G Burmester, Berlin, Germany; B Canesi, Milano, Italy; A Cantagrel, Toulouse, France; X Chevalier, Creteil, France; H Chwalinska-Sadowska, Warszawa, Poland; L Cleland, Adelaide, Australia; C Codreanu, Bucuresti, Romania; L Coster, Linkoping, Sweden; M Cutolo, Genova, Italy; R Dahl, Uppsala, Sweden; P Dawes, Stoke-on-Trent, UK; J Dehais, Bordeaux, France; D Jan De Rooij, Nijmegen, The Netherlands; J P Devogelaer, Brussels, Belgium; D Doyle, London, UK; L Euller-Ziegler, Nice, France; F Fantini, Milano, Italy; G Ferraccioli, Udine, Italy; A Filipowicz-Sosnowska, Warszawa, Poland; S Freiseleben-Sorensen, Copenhagen, Denmark; P Geusens, Diepenbeek, Belgium; J Melo-Gomes, Lisbon, Portugal; JJ Gómez Reino, Santiago de Compostela, Spain; A Gough, Harrogate, UK; JP de Jager, Southport, Australia; M Janssen, Arnhem, Netherlands; H Julkunen, Vantaa, Finland; R Juvin, Grenoble, France; H Haentzschel, Leipzig, Germany; G Herrero-Beaumont, Madrid, Spain; W Hissink-Muller, Tilburg, Netherlands; J Kalden, Erlangen, Germany; C Kaufmann, Drammen, Norway; J Kekow, Vogelsang, Germany; L Klareskog, A Harju, Stockholm, Sweden; T Kvien, Oslo, Norway; A Laffón, Madrid, Spain; RBM Landewe, Maastricht, Netherlands; H Lang, Plauen, Germany; P Lanting, Doetinchem, Netherlands; X LeLoet, Rouen, France; B Lindell, Kalmar, Sweden; F Liote, Paris, France; R Luukkainen, Satalinna, Finland; M Malaise, Liege, Belgium; X Mariette, Le Kremlin Bicetre, France; E Martín Mola, Madrid, Spain; B Masek, Venlo, The Netherlands; Z Mencel, Kalisz, Poland; O Meyer, Paris, France; Y Molad, Petah-Tikva, Israel; C Montecucco, Pavia, Italy; R Myllykangas-Luosujarvi, Kuopio, Finland; H Nielsen, Herlev, Denmark; G Papadimitriou, Athens, Greece; K Pavelka, Prague, Czech Republic; A Perniok, Köln, Germany; F Radulescu, Bucuresti, Romania; V Rodriguez Valverde, Santander, Spain; A Rubinow, Jerusalem, Israel; P Sambrook, St Leonards, Australia; R Sanmartí, Barcelona, Spain; J Sany, Montpellier, France; A Saraux, Brest, France; M Schattenkirchner, Munchen, Germany; U Serni, Firenze, Italy; L Settas, Thessaloniki, Greece; J Sibilia, Strasbourg, France; H Stehlikova, Ceska Lipa, Czech Republic; J Szechinski, Wroclaw, Poland; J Szerla, Krakow, Poland; C Tanasescu, Bucuresti, Romania; H Tony, Wurzburg, Germany; J Tornero, Guadalajara, Spain; S Transo, Jonkoping, Sweden; F Trotta, Ferrara, Italy; T Tuomiranta, Tampere, Finland; E Veys, Gent, Belgium; G Valentini, Napoli, Italy; H van den Brink, Alkmaar, Netherlands; M van de Laar, Enschede, Netherlands; P Vitek, Zlin, Czech Republic; C Voudouris, Thessaloniki, Greece; R Westhovens, Leuven, Belgium.