Article Text

Abstract
Objective: To investigate the temporal relationship between onset of inflammation (as measured by secretory phospholipase A2 (sPLA2) and C reactive protein (CRP)) and the presence of autoantibodies (IgM rheumatoid factor (IgM RF) and antibodies against citrullinated peptides (anti-CCP)) in the preclinical phase of rheumatoid arthritis (RA).
Methods: For 79 patients with RA who had been blood donors before the onset of disease, a median of 13 serum samples per patient was available. sPLA2 was measured in patient and matched control samples and related to previous CRP, IgM RF, and anti-CCP measurements. The temporal relationship between the increased markers of inflammation and autoantibodies was analysed with time lag analysis.
Results: IgM RF and anti-CCP concentrations were significantly associated (p<0.001) with concentrations of sPLA2, CRP, and the combination of sPLA2 and CRP at the same time point. However, we found no stronger association between the two autoantibody tests and the three inflammation measures 1, 2, and 3 years before or after a time point than for measurements at the same time, in the whole group or in subgroups of IgM RF and anti-CCP positive patients.
Conclusion: Both the acute phase response and autoantibody formation often develop years before the first symptoms of RA occur, and these phenomena are probably closely connected in time.
- anti-CCP, antibodies against citrullinated peptides
- CRP, C reactive protein
- RA, rheumatoid arthritis
- RF, rheumatoid factor, sPLA2, secretory phospholipase A2
- rheumatoid arthritis
- secretory phospholipase A2
- inflammation
- autoantibodies
Statistics from Altmetric.com
- anti-CCP, antibodies against citrullinated peptides
- CRP, C reactive protein
- RA, rheumatoid arthritis
- RF, rheumatoid factor, sPLA2, secretory phospholipase A2
The preclinical phase of rheumatoid arthritis (RA) is characterised by the presence of specific autoantibodies, such as IgM rheumatoid factor (IgM RF)1–3 and antibodies against citrullinated peptides (anti-CCP).2,3 One half of blood donors who later developed RA were found to be positive for IgM RF and/or anti-CCP at least once before the onset of RA.3 C reactive protein (CRP) levels, as a marker of the acute phase response, increase over time in patients with preclinical RA, with the highest values at the start of the symptoms. However, it remains unclear whether increased inflammation, measured by CRP, occurs before, after or simultaneously with the development of antibodies (IgM RF and/or anti-CCP) in the preclinical phase of RA.4
This issue is relevant to an understanding of the pathogenesis of RA: appearance of autoantibodies before a rise in inflammation markers might suggest an antibody driven inflammatory response. Conversely, detection of inflammation before the increase in autoantibodies would provide evidence that antibody formation only occurs after a detectable level of inflammation has been reached. In addition, evidence for a temporary concentration peak of a marker of inflammation before autoantibody formation would lend support to the possibility of an infectious process preceding the development of RA.
Therefore, in the present study secretory phospholipase A2 (sPLA2)—another sensitive marker of the acute phase response—was measured to investigate the temporal relationship between the onset of inflammation and the presence of autoantibodies in the preclinical phase of RA. In addition, this relationship was also tested using CRP and the combination of sPLA2 and CRP.
PATIENTS AND METHODS
Study subjects
Since 1984, the Sanquin Blood Bank North West Region in Amsterdam, The Netherlands, has stored serum from donated blood at −30°C. We identified 79 patients with RA registered at the Jan van Breemen Institute who donated blood, in general 2–4 times a year, before the onset of the symptoms, as described previously.3 For each RA sample, one control sample was selected, matched for sex, age, and time of blood donation. sPLA2 was measured with an in-house enzyme linked immunosorbent assay (ELISA).5 CRP, IgM RF, and anti-CCP had been determined previously.3,4 The study was approved by the local Institutional Review Board (ethics committee: Slotervaart Hospital, Jan van Breemen Institute and BovenIJ Hospital, Amsterdam, The Netherlands).
Statistical analysis
In a first analysis, the progression of the sPLA2 concentration over time in the patient and control groups, corrected for age, sex, and CRP, was estimated with random coefficient analysis. This longitudinal regression technique was used because each patient had a different number of measurements at different points in time.
In a second analysis, all patient samples were used to study the temporal relationship between the increased markers of inflammation and autoantibodies in preclinical RA with time lag analyses.6 Concentrations of IgM RF and anti-CCP, on the one hand, were associated with concentrations of (a) sPLA2; (b) CRP; and (c) the combination of sPLA2 and CRP (Z score ln_sPLA2 + Z score ln_CRP), on the other hand, at the same time point as well as at 1, 2, and 3 years before, and 1, 2, and 3 years after that time. By comparing the magnitude of the different regression coefficients, one can determine if a time lag is present. The regression coefficients were calculated by random coefficient analysis and corrected for age and sex.
Finally, the same time lag analyses were repeated in two subgroups: (a) the relationship between the increase of IgM RF and the inflammation markers over time was studied in all samples of the patients who were positive for IgM RF at least once before the onset of the symptoms; and (b) the relation between anti-CCP and the inflammation markers was analysed in all serum samples of the patients who were positive for anti-CCP at least once before the start of the symptoms.
In all analyses, the natural logs of sPLA2, CRP, IgM RF, and anti-CCP were used, because of the non-normal distribution of these variables. Random coefficient analyses were performed with MLwiN (Multilevel Models Project; Institute of Education, University of London, London, UK), a statistical program for multilevel analyses.
RESULTS
Seventy nine patients (50 (62%) female; mean age at onset of symptoms 51 years) who had been blood donors before the onset of RA were identified. A median of 13 serum samples per patient (range 1–51) was available; the median time between the first donation and the onset of the symptoms was 7.5 years (range 0.1–14.5). In total, 1078 patient sera and 1071 matched control serum samples were tested.
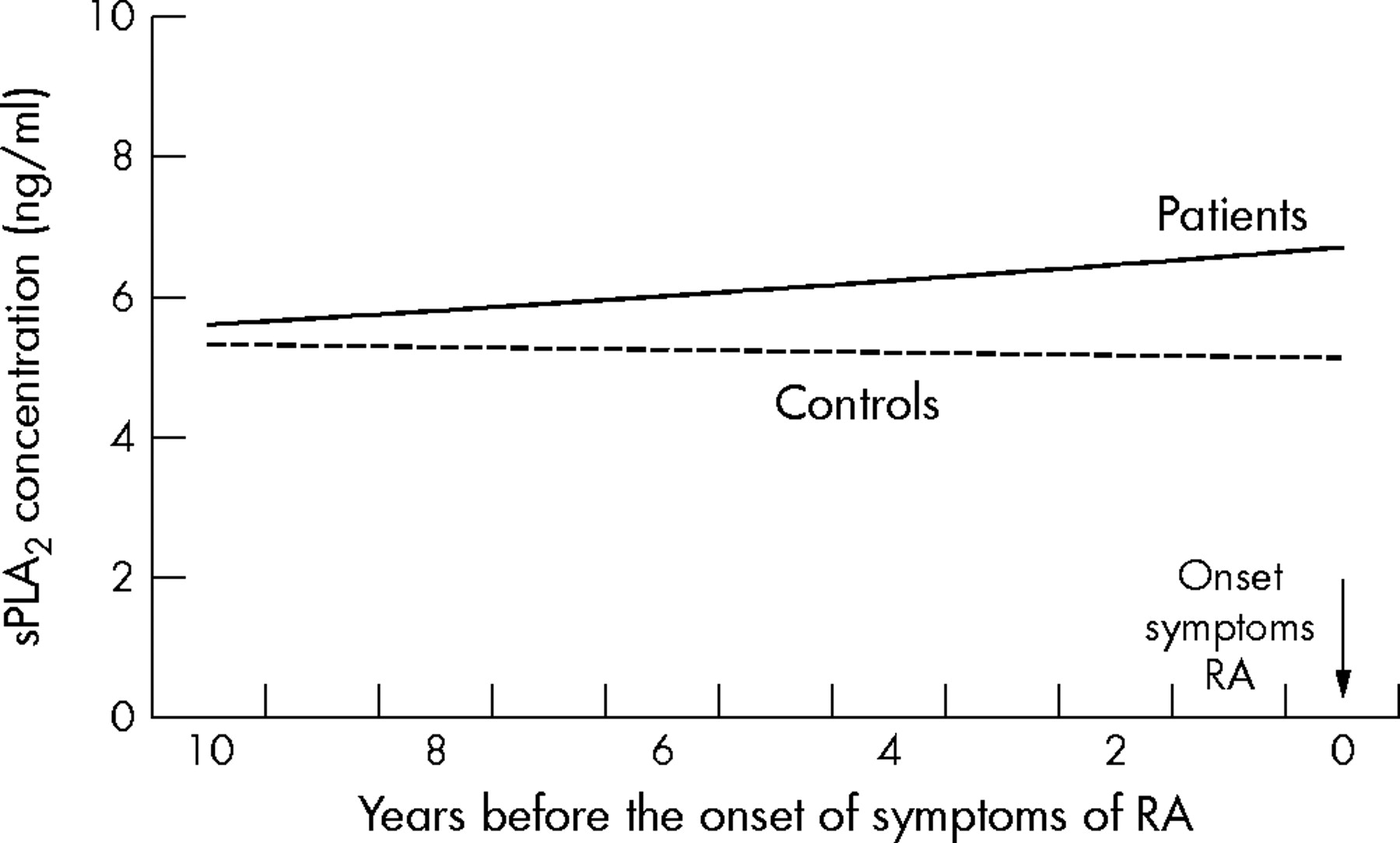
Figure 1 shows the sPLA2 levels of the patients and controls before the onset of symptoms, corrected for age, sex, and CRP. The mean sPLA2 level of the patient group increased significantly over time (p = 0.005) with the highest values at the onset of the symptoms, whereas the mean sPLA2 level of the controls remained stable (p = 0.50).

{kind=link}
Secretory phospholipase A2 (sPLA2) levels before the onset of symptoms in the preclinical phase of patients with RA and in controls.
Table 1 shows the results of the time lag analyses in the group of patients with RA. The concentrations of IgM RF and anti-CCP were significantly associated (p<0.001) with the concentrations of sPLA2, CRP, and the combination of sPLA2 and CRP at the same point in time. In the group as a whole, the association between the two autoantibody tests and the three inflammation parameters as measured 1, 2, and 3 years before as well as 1, 2, and 3 years after a point in time was no stronger than the association based on measurements at that same point in time.
Association between autoantibodies and measures of inflammation (CRP, sPLA2, and the combination of CRP and sPLA2) at different points in time
Also, in the subgroups of IgM RF positive and the anti-CCP positive patients there was no stronger association between the antibody tests and the inflammatory measures 1, 2, and 3 years before and after a point in time in comparison with the association based on measurements at that same time (data not shown).
DISCUSSION
Serum levels of sPLA2 were increased in the preclinical phase of patients with RA in comparison with levels of healthy controls, in a manner similar to CRP, as published previously.4 Both measures of inflammation were used to study the temporal relationship between the increased markers of inflammation and autoantibodies in preclinical RA. The sophisticated technique of time lag analysis, did not detect a stronger association between the antibody tests and the inflammatory measures up to 3 years before or after a point in time in comparison with measurements at the same time.
In a previous study we concluded that it remained unclear whether increased inflammation, measured by CRP, occurs before, after or simultaneously with the development of autoantibodies in preclinical RA.4 sPLA2 is also increased in preclinical RA, but the patterns over time of sPLA2 and CRP differ between individual patients. Therefore, both measures of inflammation were analysed separately and combined in a new time lag analysis in an attempt to unravel the sequence of increased inflammation and raised autoantibody concentrations in the preclinical phase of RA. Because again we did not find a time lag, it is unlikely that a time lag can be found by adding other inflammatory measures to the analysis, and the possibility of a simultaneous occurrence of these phenomena becomes more likely.
A possible explanation for missing an actually existing time lag might be that the available blood samples, although numerous, were taken too far apart in time to be able to detect a short time lag. A possibly temporary sPLA2 or CRP peak indicative of an infectious process involved in causing the RA might also have been missed because the samples were obtained too far apart. The opposite conclusion, that because there is no evidence for a time lag, the phenomena of inflammation and autoantibody formation must be intimately coupled, is likely to be true but cannot be established beyond doubt on the basis of the present data. Support for the possibility of simultaneous development comes from the observed link between local antibody production and level of inflammation in the rheumatoid synovium.7 In the somewhat different situation of B cell depletion in established RA, the relapse of active arthritis after recovery from this depletion coincides with increasing CRP levels, which are preceded by a rise in autoantibody levels.8
In conclusion, both the acute phase response and autoantibody formation often develop years before the first symptoms of RA occur, and these phenomena are probably closely connected in time.
Footnotes
-
Published Online First 3 August 2005
-
Competing interest: None.