Article Text

Abstract
Objective: To evaluate the efficacy and safety of adalimumab plus methotrexate (MTX) given for up to 4 years in patients with active, longstanding rheumatoid arthritis.
Methods: Patients responding inadequately to MTX were entered into a 24 week, controlled study (ARMADA) with adalimumab plus MTX or placebo plus MTX, and some were enrolled in a subsequent open label extension. The efficacy and safety of treatment were evaluated. Additional analyses were made for those patients whose corticosteroid and/or MTX dosages were adjusted during the extension.
Results: Of 271 patients in the original ARMADA trial, 262 received at least one dose of adalimumab and were evaluated. At the time of analysis, 162/262 (62%) patients had remained in the study and received treatment for a mean of 3.4 years. Withdrawals were for lack of efficacy (8%), adverse events (12%), and other reasons (18%). In 147 patients who completed 4 years’ treatment, efficacy achieved at 6 months was maintained. At 4 years, 78%, 57%, and 31% had achieved ACR20/50/70; 43% achieved clinical remission (DAS28 <2.6); and 22% had no physical function abnormalities (HAQ = 0). Results were similar for 196 patients who received treatment for 2–4 years. Efficacy was maintained in many patients when dosages were decreased (corticosteroids (51/81 (63%) patients), MTX (92/217 (42%)), or both (25/217 (12%))). Serious adverse events were comparable during open label treatment and the controlled phase. Serious infections occurring during open label treatment and the blinded period were similar (2.03 v 2.30 events per 100 patient-years, respectively).
Conclusions: Adalimumab plus MTX sustained clinical response and remission in patients with RA during 4 years. The safety profile during the first 6 months was similar to that after 4 years’ follow up. Reduction of corticosteroid and/or MTX dosages did not adversely affect long term efficacy.
- ACR, American College of Rheumatology
- AEs, adverse events
- CI, confidence interval
- CRP, C reactive protein
- DAS28, 28 joint count Disease Activity Score
- DMARDs, disease modifying antirheumatic drugs
- HAQ, Health Assessment Questionnaire
- LOE, lack of efficacy
- MTX, methotrexate
- PPD, purified protein derivative
- RA, rheumatoid arthritis
- SIR, standardised incidence ratio
- SJC, swollen joint count
- TJC, tender joint count
- TNF, tumour necrosis factor
- rheumatoid arthritis
- adalimumab
- treatment
- tumour necrosis factor antagonists
- open label extension studies
Statistics from Altmetric.com
- ACR, American College of Rheumatology
- AEs, adverse events
- CI, confidence interval
- CRP, C reactive protein
- DAS28, 28 joint count Disease Activity Score
- DMARDs, disease modifying antirheumatic drugs
- HAQ, Health Assessment Questionnaire
- LOE, lack of efficacy
- MTX, methotrexate
- PPD, purified protein derivative
- RA, rheumatoid arthritis
- SIR, standardised incidence ratio
- SJC, swollen joint count
- TJC, tender joint count
- TNF, tumour necrosis factor
- rheumatoid arthritis
- adalimumab
- treatment
- tumour necrosis factor antagonists
- open label extension studies
Although the pathophysiology of rheumatoid arthritis (RA) is not completely understood, tumour necrosis factor (TNF), a proinflammatory cytokine, appears to have a key role in its aetiology.1,2 Use of TNF antagonists in combination with methotrexate (MTX) has emerged as a highly effective and targeted therapeutic strategy that directly alters the biological processes underlying RA synovial inflammation and progressive structural destruction.3,4 Adalimumab, an anti-TNF monoclonal antibody that consists entirely of human amino acid sequences, has been extensively studied in clinical trials. The ARMADA trial, a 6 month, placebo controlled, phase II/III study, demonstrated significant reductions in signs and symptoms of RA, improvement in physical function, and the safety of adalimumab plus MTX v placebo plus MTX.5 Significant clinical improvements were achieved in the patients who had received adalimumab 40 mg every other week with MTX. The American College of Rheumatology (ACR) response rates for the group receiving adalimumab plus MTX were ACR20 for 67%, ACR50 for 55%, and ACR70 for 27%, as compared with 15%, 8%, and 5%, respectively, for patients who had received placebo (MTX monotherapy)(p<0.001).5
Further trials confirmed and extended these findings to demonstrate the efficacy and safety of adalimumab in combination with standard antirheumatic treatments6 or when used as monotherapy,7 and provided evidence of inhibition of joint damage after 1 year’s treatment with adalimumab plus MTX.8 Randomised controlled trials spanning 6 months to 2 years have been conducted with the TNF antagonists, infliximab9–,11 and etanercept.12–,14 These trials have shown efficacy and safety outcomes comparable to those found for adalimumab. However, limited information is available on the long term efficacy and safety of adalimumab for patients treated for more than 3 years.15,16 Long term extension studies are essential to confirm that the efficacy and safety of TNF antagonists seen in short term studies are sustained over longer periods.
The objectives of this long term, open label extension study of the ARMADA trial were (a) to assess the sustained efficacy of adalimumab in combination with MTX; (b) to confirm the long term safety and tolerability of this regimen; and (c) to determine if clinical efficacy was maintained in patients whose corticosteroid and/or MTX dosages were reduced.
PATIENTS AND METHODS
Patients
Patients were eligible to enrol in the randomised, controlled ARMADA trial if they were aged ⩾18 years, met ACR criteria for the diagnosis of RA,17 and had at least nine tender joints (of 68 evaluated) and six swollen joints (of 66 evaluated).5 Patients were required to have been treated with MTX for a minimum of 6 months before screening and to have been receiving a stable weekly dose of 12.5–25 mg for at least 4 weeks before screening. Patients intolerant of higher doses of MTX were enrolled with dosages of 10 mg/week.5
Treatment
During the 6 month, blinded ARMADA trial, patients were randomised to receive either placebo or adalimumab at dosages of 20 mg, 40 mg, or 80 mg subcutaneously every other week. MTX and corticosteroid doses and routes of administration were required to remain unchanged (up to 25 mg MTX a week and 10 mg of oral prednisone equivalent a day). Once patients completed the 24 week, blinded portion of the trial, all patients (including those originally receiving placebo) were permitted to enter an open label extension study and receive the standard adalimumab dose of 40 mg every other week in combination with MTX. In addition, patients, whether they had received adalimumab or placebo, who had failed to achieve clinical improvement (<ACR20) at or after 16 weeks in the blinded trial could enter the open label extension at that time. After having completed the blinded period and having participated in the extension trial for at least 6 months, patients were allowed to reduce their dosages of corticosteroids and/or MTX at the discretion of the principal investigators. These reductions were neither suggested nor required by the study protocol. Tapering was conducted according to standard medical practice for controlling disease activity.
Efficacy assessments
Efficacy outcomes were regularly evaluated and assessed as observed data. Patients who dropped out before a given time point were not considered in the calculation for that time point in this open label extension study, whereas in the randomised trial (ARMADA), patients who withdrew any time before week 24 were deemed non-responders. Treatment time was calculated beginning with the first subcutaneous injection of adalimumab at any dose, excluding the time receiving placebo. Baseline values for the patient group analysed in this study reflect the values at entry of patients randomised to either placebo or adalimumab in the controlled period of the trial. Consequently, changes from baseline in any efficacy variable were measured v this baseline. Improvements in signs and symptoms of RA were evaluated using the ACR20/50/70 criteria for clinical improvement.18 Additional clinical evaluations were based on the 28 joint count Disease Activity Score (DAS28) using the C reactive protein (CRP) based formula, useful for continual assessments of efficacy.19 A DAS28 cut off value of <2.6 was used to define clinical remission based on published sensitivity and specificity analyses in clinical settings.20 Physical function was evaluated by measuring changes in the disability index of the Health Assessment Questionnaire (HAQ).21
Safety assessments
Patients were monitored for adverse events (AEs) during the entire study, from signed informed consent through last visit. Assessments of drug safety and tolerability were based on records of AEs. Safety appraisal focused on the types and frequencies of common and serious AEs, comparing the blinded and open label extension periods of the ARMADA trial. A serious AE was defined according to the Medical Dictionary for Regulatory Activities as an AE that was fatal or life-threatening; required prolonged inpatient hospitalisation; resulted in persistent or significant disability, congenital anomaly, birth defect, miscarriage or elective abortion; or required medical/surgical intervention to prevent another serious outcome.
Statistical analysis
Patients who had remained in the study and had completed visit reports within prespecified time frames since study entry were analysed. Patients who dropped out before a given time point were not considered in the calculation for that time point. The number of patients available for analysis at any time point was driven by prospectively scheduled study visits, which explains how more patients were available at later time points (for example, 199 at 18 months, compared with 176 at 12 months). A 30 day window (⩽15 days before or after the prescribed study visit) was used to capture visits at 6 and 12 months since study entry (monthly visits), and a 90 day window (⩽45 days before or after the prescribed study visit) was used at 18 months and beyond (visits every 3 months). A paired t test was employed to detect statistically significant differences in disease activity and functional outcomes from baseline in patients available for analysis at 4 years.
AEs were analysed and reported as events per 100 patient-years. Standardised incidence ratios (SIRs) and 95% confidence intervals (CIs) for those ratios, were calculated as the observed-to-expected cancer incidence rates in the American population as reported by the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) registry.22 Changes in dosage of MTX or corticosteroids were evaluated exclusively for patients who had been in the extension study for at least 6 months and had become eligible for discretionary dose tapering. Efficacy outcomes were evaluated in the categories of “reduced dosing,” “no change”, or “increased dosing” of corticosteroids (adjusted to the prednisone equivalent) and MTX from entry visit in the blinded ARMADA trial to the last visit in either the ARMADA or the extension trial. Changes in average dosing were assessed statistically using Wilcoxon’s signed rank test.
RESULTS
Patient disposition
A total of 271 patients were randomised into the ARMADA trial, and 161 patients completed 24 weeks. All patients completing week 24, including those in the placebo arm, as well as any patient who failed to meet or maintain an ACR20 response at week 16, were eligible to roll over into an open label extension study.5 Ninety two patients who did not achieve an ACR20 at week 16 elected to enter the open label extension between weeks 16 and 24. In addition, 18 patients, nine of whom had received placebo, withdrew from the study before week 16 and were not eligible to enter the extension study. This study evaluated a total of 262 of the 271 patients originally randomised in the ARMADA trial who had received adalimumab either during the 24 week blinded period or during the open label continuation period. All patients received the standard 40 mg every other week dosing during the open label period, except five patients whose adalimumab dosing was increased to weekly, plus MTX, starting at year 3.
Of the 262 patients originally enrolled in this study, 228 (87%), 207 (79%), 186 (71%), and 168 (64%) remained in the study after 1, 2, 3, and 4 years of treatment, respectively (fig 1⇓). Among the 100 patients (38%) who withdrew from the study, 22 (8%) withdrew for lack of efficacy (LOE), 30 (12%) for AEs, and 48 (18%) for other reasons, including protocol violation, withdrawal of consent, or lost to follow up. About one third of all withdrawals (n = 33) took place in the first year of treatment (3.4% LOE, 4.6% AE, 4.6% other; n = 262). In the remaining years, the rates were: year 2 (n = 225): 1.3% LOE, 1.8% AE, 5.8% other; year 3 (n = 198): 3% LOE, 3.5% AE, 4% other; and year 4 (n = 177): 1.7% LOE, 1.7% AE, 4.6% other.

The retention rate of patients treated with adalimumab for up to 4 years (Kaplan-Meier analysis).
The overall exposure time to adalimumab in combination with MTX used for the safety evaluation was 886 patient-years (as of 31 August 31 2004). The mean (SD) time receiving treatment was 41 (19) months, with a minimum of 1 and maximum of 59 months. At the time of this analysis, 162 (62%) patients continued to receive treatment. The numbers of patients available for all efficacy assessments were: 221 (84%) patients for 6 months, 176 (67%) for 1 year, 196 (75%) for 2 years, 176 (67%) for 3 years, and 147 (56%) for 4 years.
Demographic and baseline characteristics
The mean age of all 262 patients treated with adalimumab and evaluated in this study was 55 years, and the majority were women (76%) (table 1⇓). The mean duration of disease was 12.4 years. Baseline mean total joint count (TJC), swollen joint count (SJC), and HAQ values were all indicative of significant disease activity, which occurred despite previous use of various antirheumatic drugs. At the time of enrolment, the majority of patients (74%) had been treated previously with two or three traditional disease modifying antirheumatic drugs (DMARDs), including MTX, and 25% had received four or more (average three DMARDs). The demographic and baseline disease characteristics (TJC, SJC, HAQ, CRP, and DAS28) of the subgroup of 147 patients who had reached 4 years of treatment were comparable to those of the larger group of 262 patients who had received adalimumab at any point during the double blind, randomised ARMADA trial or its open label extension (table 1⇓).
Demographic and baseline disease characteristics of patients with RA who received adalimumab at any time during the blinded period or open label extension of the ARMADA study (n = 262)
Long term efficacy
In the 147 patients who had completed 4 years of continuous treatment, 78%, 57%, and 31% achieved ACR20, ACR50, and ACR70 responses, respectively; and 43% achieved clinical remission based on the DAS28 cut off point for remission (DAS28 <2.6). These patients showed a statistically significant reduction of mean TJC by more than 70%, while mean SJC and DAS28 score had decreased by 40–60% compared with baseline values. The mean HAQ was 0.7 among these patients, indicative of a significantly improved physical functioning status v baseline (table 2⇓).
Efficacy assessments of patients with RA in the ARMADA trial/open label extension who completed 4 years of continuous treatment with adalimumab
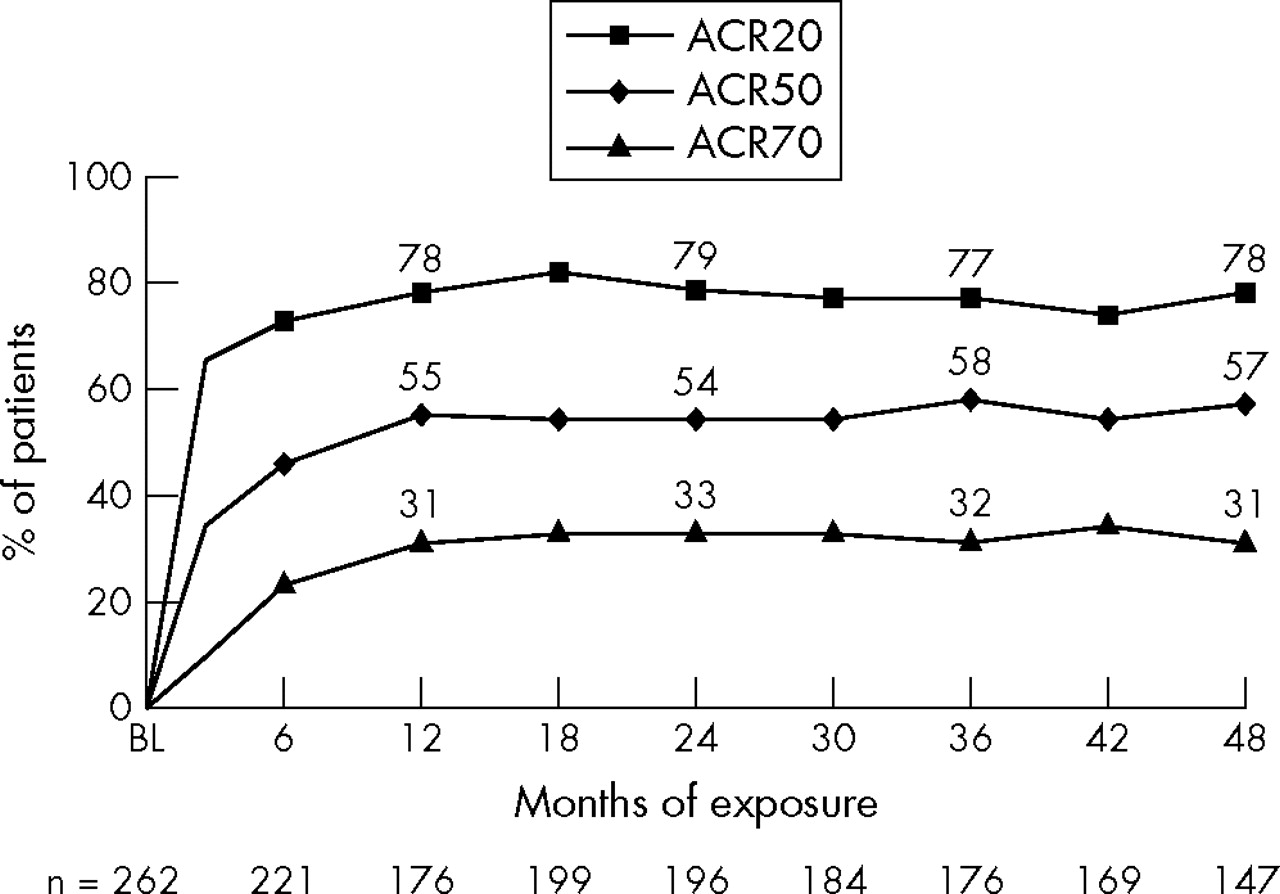
Similarly, results for the 196 patients who had 2–4 years’ treatment with adalimumab confirmed that clinical benefits achieved during the first 6 months of treatment, either in the blinded period of the ARMADA trial for patients receiving the active drug or in the first 6 months of the open label trial for patients originally receiving placebo, were sustained with adalimumab treatment throughout the continuation study. Figure 2⇓ shows the ACR response criteria of patients receiving continuous adalimumab treatment at different time points (excluding withdrawals), confirming that, at year 1, a majority of them had already experienced ACR20 improvement, while more than half of the patients achieved an ACR50 response, and approximately one third had achieved an ACR70 response rate.
{kind=link}
{kind=link}
Time course of ACR responses in patients with RA treated with adalimumab and MTX in the ARMADA trial/open label extension.
The percentages of patients who had achieved clinical remission using the DAS28 <2.6 criterion19,23 were 32% at 6 months and 43% at 4 years. At 2 years, almost a third of patients had achieved at least a 70% improvement in signs and symptoms (ACR70), and about a quarter had shown no signs of involvement in any joint (TJC = 0, SJC = 0). In addition, throughout 4 years, 80–82% of patients had achieved a clinically meaningful improvement in their HAQ scores (⩾–0.22),24 and 14–24% of patients had reached and sustained a completely normal physical function status while receiving adalimumab treatment, assessed by a HAQ score of 0 (table 3⇓).
No (%) patients with RA during the ARMADA trial and open label extension with no signs of joint involvement (TJC = 0, SJC = 0), normal CRP (<8 mg/l), ACR70 response, clinical remission based on DAS28 <2.6, clinically meaningful improvements in HAQ score (HAQ reduction ⩾–0.22), and normal functional status (HAQ = 0)
Overall control of RA disease activity was further demonstrated by other measures. The reduction in mean DAS28 scores confirmed that the control of disease activity achieved in the first 6 months of treatment was sustained through 4 years in those patients who continued adalimumab treatment. Mean DAS28 had declined from 5.8 at baseline to 3.3 at 6 months and 3.2, 3.1, 3.1, and 3.0 at years 1, 2, 3, and 4, respectively. For the 100 patients who withdrew from the study, some degree of improvement in DAS28—with values declining from 5.7 at baseline to 4.0 at their last visits—was seen. Interestingly, patients who withdrew because of lack of efficacy (n = 22) showed higher baseline disease activity (mean DAS28 = 6.3) and had achieved marginal improvement by their last visits (mean DAS28 = 5.3). Mean CRP concentrations had decreased from 27 mg/l at baseline to 6 mg/l after 1 year of continuous treatment, indicative of normalisation in this biomarker of systemic inflammation. This reduction was sustained in patients who received adalimumab from 2 through 4 years, as shown by CRP concentrations <9 mg/l. In addition, reductions in the mean TJC and SJC were seen at 6 months of treatment and sustained over time in completers. The reduction seen in TJC was from a mean of 28 at baseline to 8–10 joints at years 1 through 4. Mean SJC had declined from 17 affected joints to 5–6 joints at years 1 through 4. During the first 6 months of treatment, the mean HAQ score had decreased from 1.5 to 0.8. This improvement was sustained for up to 4 years, with a HAQ score of 0.8 at years 1 through 3, and a score of 0.7 at year 4.
Reduction of corticosteroids and MTX
Only those patients who had received adalimumab 40 mg every other week plus MTX for a minimum of 6 months in the extension period were deemed eligible for discretionary corticosteroid or MTX dosage adjustments. A total of 217 patients who had been treated for 8–59 months met this criterion and were evaluated. Of the 81 patients treated with corticosteroids and eligible for discretionary corticosteroid dosage tapering, dosages were decreased for 51 (63%), including 23 (28%) who discontinued corticosteroids altogether; unchanged for 29 (36%); and increased for 1 patient (1%). The mean (SD) initial dosage of corticosteroids was 5.8 (3.1) mg/day (range 1–24), whereas the dose at the last visit was 2.7 (2.4) mg/day (range 0–10) (p<0.0001).
The mean (SD) initial MTX dosage was 16.5 (4.4) mg/week (range 2.5–25), and at the last visit was 13.8 (5.7) mg/week (range 1.25–25) (p<0.0001). Ten patients were receiving a dose of 2.5 mg/week at their respective last visits. MTX dosage reductions were seen in 92 (42%) patients, 110 (51%) remained unchanged, and 15 (7%) had had a dose increase. Further, a total of 25 (12%) patients had decreased both their corticosteroid and MTX dosages. Table 4⇓ shows that patients who reduced their corticosteroid and/or MTX dosages while receiving adalimumab treatment maintained their levels of efficacy over time (table 4⇓).
Efficacy data at last visit for patients with RA in the ARMADA trial/open label extension who were eligible for corticosteroid and/or MTX dosage adjustments*
Long term safety
The types and cumulative frequency of serious AEs per 100 patient-years seen during the blinded and open label extension trial periods combined were consistent with those reported in the blinded period of the ARMADA trial (table 5⇓). The rate of serious infections was slightly lower throughout the entire study than in the blinded period alone (table 5⇓). A tuberculin purified protein derivative (PPD) skin test was performed at the screening visit for all patients. Standard chest radiographs were also taken at the screening visit and at week 24. At baseline, 11/271 (4.1%) randomised patients had positive PPD results at screening, including 9/209 (4.3%) adalimumab treated patients and 2/62 (3.2%) placebo treated patients. These patients were treated with tuberculosis prophylaxis in accordance with accepted medical practice. No cases of tuberculosis or other opportunistic infections were reported.
Rates of serious adverse events during the blinded and open label extension period of the ARMADA trial
A total of 19 cancers were seen during the study. Five were non-melanoma skin cancers (all basal cell carcinomas), and the remaining 14 spanned all other cancer sites. Four malignancies were in the gastrointestinal tract (one each in the gall bladder and pancreas, two in the colon); two in the prostate; and one each in the lung, kidney, breast, ovary, and uterus. In addition, there was one melanoma, one acute myeloid leukaemia, one chronic lymphocytic leukaemia, and no cases of lymphoma. If non-melanoma skin cancers were excluded, the SIR was 1.57 (95% CI 0.86 to 2.64). No patient developed systemic lupus erythematosus or pancytopenia. After 8 months of treatment, a 50 year old woman was diagnosed with multiple sclerosis and received treatment with interferon beta after having discontinued adalimumab treatment permanently. Another patient developed congestive heart failure. Six deaths were reported, at a rate of 0.7 per 100 patient-years. One patient each died of congestive heart failure, acute myocardial insufficiency, aortic aneurysm previously treated surgically, cerebrovascular accident, intracranial haemorrhage, and acute kidney failure, respectively. No other additional safety signals or unexpected serious AEs were reported.
DISCUSSION
The present extension study demonstrated, for the first time, that a majority of patients with longstanding RA who had continued to receive the standard treatment of adalimumab plus MTX for up to 4 years experienced significant, sustained improvements in signs and symptoms, disease activity, and functional status. The results of this study are consistent with those seen in patients treated with etanercept in combination with MTX for 3 years.15 Although MTX is considered the anchor drug of RA treatment, in some studies MTX monotherapy may lead to decreased efficacy and reduced patient compliance over time.25–,28 On the other hand, the long term efficacy and consistent safety profile observed when MTX is combined with a TNF antagonist may lead to sustained patient compliance. In randomised studies, initiation of a TNF antagonist in combination with MTX has shown the combination to be more efficacious than either MTX5,6,8,9,10,11,14,15 or TNF antagonists as monotherapy,12,29 without being necessarily more toxic.
A key finding of the ARMADA extension study is that large percentages of patients demonstrated no signs of swollen or tender joints, clinical remission (>40% based on DAS28 <2.6), and completely normal physical function over time. This study also confirms that those patients who continued to receive adalimumab plus MTX treatment for up to 4 years (about 62% of the originally randomised patients) were able to sustain the efficacy levels they achieved within the first 6 months of treatment, the end point of the blinded period of the trial. Moreover, the types and rates of AEs seen over the long term were consistent with the safety profile seen during the first 6 months of treatment. The baseline demographics and disease characteristics of patients who had continued to receive treatment for 4 years were similar to those of patients enrolled in the initial blinded period of ARMADA. In this study, patients with longstanding, moderate to severe RA who had responded initially to adalimumab treatment were able to maintain response for up to 4 years while receiving treatment, and eventually achieved additional clinical benefits over time, including clinical remission, without incurring additional safety risks. A separate analysis of disease activity in patients who withdrew for any reason from the study demonstrated consistent DAS28 improvement for patients while receiving adalimumab. Interestingly, higher baseline disease activity and marginal DAS28 improvement were seen in patients who withdrew because of lack of efficacy.
The reduction of HAQ to an average mean score of 0.7–0.8 for up to 4 years seen in this study is important for the long term prognoses of these patients. Although functional improvements achieved with TNF antagonists mostly depend on baseline joint destruction in individual patients,30 the direct correlation between physical function and radiographic progression is stronger for patients with longstanding, active RA than for patients in the early stages of the disease.31 The functional improvements seen in this study need to be complemented with studies confirming long term inhibition of radiographic progression in patients with longstanding RA.
This was an open label, observational study (that is, efficacy results reported here refer only to “completers,” or patients who had continued to receive treatment at the time of the analysis). Therefore, the clinical interpretation of these results should also take into account the patients who withdrew from the study, including 8% who withdrew because of lack of efficacy and 12% because of adverse events. The level of compliance with adalimumab treatment after a mean of 3.4 years’ treatment is consistent with two long term studies of TNF antagonists in combination with MTX.15,32 In addition, the retention rate in this extension study might have been influenced by the stringent requirements of a clinical trial and the free availability of medical evaluations, laboratory tests, and drugs.
In this study, the dosages of corticosteroids and MTX were allowed to be altered based on clinical judgment, after a defined period of time receiving adalimumab plus MTX treatment. An evaluation of these changes and their clinical impact discloses additional benefits of long term combination treatment with a TNF antagonist. Firstly, the vast majority of patients were able to reduce or maintain their dosages of concomitant corticosteroids or MTX while achieving significant efficacy improvements. Secondly, these results validate the reduction of corticosteroid and/or MTX dosages in patients responding to TNF antagonists. In particular, reduction or discontinuation of corticosteroids has important positive effects, including decreased incidence of infections, gastrointestinal ulcerations, and mental or skin abnormalities, as well as decreased risk of fractures.
A major objective of this long term, open label study of adalimumab was to evaluate long term toxicity, especially to examine the possibility that specific AEs, such as serious infections, might occur more frequently after lengthy exposure to the drug. This study of 262 patients who had received, on average, more than 3 years of continuous treatment and spanning more than 886 patient-years shows that treatment with adalimumab in combination with MTX was well tolerated. The types and frequencies of serious AEs observed were comparable to those reported in the blinded period of the initial, randomised controlled ARMADA trial5 and were similar also to rates reported in other adalimumab pivotal trials.6–,8 The rate of serious infections of 2.03/100 patient-years after 886 patient-years of treatment was similar to rates reported in the general RA population,33,34 in the ARMADA trial,5 and in other controlled trials of adalimumab and other TNF antagonists.6,7,8,9,10,11,12,13,14,15 One consideration is that the selection of patients for clinical trials, including ARMADA, excluded those with a few, selected comorbidities. No cases of tuberculosis were seen despite the inclusion of 11 patients with positive PPD results who had been prophylactically treated. In addition, the types and rates of malignancies observed in this study are consistent with those reported previously for adalimumab and other TNF antagonists5,8,9,10,11,12,15,35 and in the overall population of patients with RA.35
In conclusion, the majority of patients with active RA who entered this study of adalimumab in combination with MTX achieved substantial improvement in disease activity, including improvement in swollen and tender joint counts, global assessment of disease activity, functional status, and CRP concentration, and were able to reduce background dosages of corticosteroids and/or MTX. These improvements were sustained for 4 years, with many patients achieving clinical remission and functional normality with continuous adalimumab treatment, and demonstrating an acceptable safety profile during this period. To acquire even longer term information about drug response and tolerability, these patients with RA will continue to be followed up over time.
Acknowledgments
The ARMADA study was funded fully by Abbott Laboratories. Drs Weinblatt, Keystone, Furst, and Kavanaugh each received research funding to support this study and they also serve as consultants to Abbott Laboratories. Drs Chartash and Segurado are employees of Abbott Laboratories.
The authors thank Michael Nissen, ELS, of Abbott Laboratories for his editorial assistantce in the development of this manuscript, and Joseph Beason of Abbott Laboratories for his assistance with data acquisition/analysis.
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
Published Online First 1 December 2005