Article Text

Abstract
Background: Resistin is a newly identified adipocytokine which has demonstrated links between obesity and insulin resistance in rodents. In humans, proinflammatory properties of resistin are superior to its insulin resistance-inducing effects.
Objectives: To assess resistin expression in synovial tissues, serum and synovial fluid from patients with rheumatoid arthritis, osteoarthritis and spondylarthropathies (SpA), and to study its relationship with inflammatory status and rheumatoid arthritis disease activity.
Methods: Resistin expression and localisation in synovial tissue was determined by immunohistochemistry and confocal microscopy. Serum and synovial fluid resistin, leptin, interleukin (IL)1β, IL6, IL8, tumour necrosis factor α, and monocyte chemoattractant protein-1 levels were measured. The clinical activity of patients with rheumatoid arthritis was assessed according to the 28 joint count Disease Activity Score (DAS28).
Results: Resistin was detected in the synovium in both rheumatoid arthritis and osteoarthritis. Staining in the sublining layer was more intensive in patients with rheumatoid arthritis compared with those with osteoarthritis. In rheumatoid arthritis, macrophages (CD68), B lymphocytes (CD20) and plasma cells (CD138) but not T lymphocytes (CD3) showed colocalisation with resistin. Synovial fluid resistin was higher in patients with rheumatoid arthritis than in those with SpA or osteoarthritis (both p<0.001). In patients with rheumatoid arthritis and SpA, serum resistin levels were higher than those with osteoarthritis (p<0.01). Increased serum resistin in patients with rheumatoid arthritis correlated with both CRP (r = 0.53, p<0.02), and DAS28 (r = 0.44, p<0.05), but not with selected (adipo) cytokines.
Conclusion: The upregulated resistin at local sites of inflammation and the link between serum resistin, inflammation and disease activity suggest a role for resistin in the pathogenesis of rheumatoid arthritis.
- DAS28, Disease Activity Score 28
- DMARDs, disease-modifying antirheumatic drugs
- SpA, spondylarthropathy
- TNF, tumour necrosis factor
Statistics from Altmetric.com
- DAS28, Disease Activity Score 28
- DMARDs, disease-modifying antirheumatic drugs
- SpA, spondylarthropathy
- TNF, tumour necrosis factor
Resistin, also known as adipocyte secreted factor or found in inflammatory zone 3, is a recently described adipocytokine that is a member of low molecular weight cystein-rich secreted peptides.1 Resistin has been previously suggested to link obesity to the insulin resistance and type II diabetes mellitus in animal models.2 It is expressed and secreted by adipose tissue, but has also been identified in several other tissues in rodents.3 In contrast with animal models, immunocompetent cells rather than adipocytes seem to be the major source of resistin in humans.4 Although several studies reported increased circulating resistin levels in human obesity and type II diabetes mellitus, these findings were not observed consistently5–7; moreover, serum resistin levels correlated better with the degree of subclinical inflammation than insulin resistance itself.
Rheumatoid arthritis represents the most common form of chronic inflammatory joint disease leading to cartilage and bone destruction. The inflammatory process causes diffuse thickening and hyperplasia of the rheumatoid arthritis synovium. It is infiltrated with numerous inflammatory cells that produce several proinflammatory cytokines including interleukin (IL)1, IL6 and tumour necrosis factor (TNF)α. The blockade of these factors has already led to the development of highly efficient biological treatments of rheumatoid arthritis.8 Resistin gene expression in peripheral blood mononuclear cells (PBMCs) was shown to be upregulated, particularly on stimulation with the aforementioned proinflammatory cytokines IL1, IL6 and TNFα.9 Moreover, it has been shown recently, that plasma resistin levels correlate significantly with inflammatory markers such as C reactive protein (CRP), IL6 and TNF receptor 2.10 These findings may provide a novel link between elevated resistin levels and associated inflammatory processes. Furthermore, elevated levels of resistin have been shown in the synovial fluid from patients with rheumatoid arthritis and also correlated strongly with inflammatory markers such as erythrocyte sedimentation rate (ESR) and CRP.11 In addition, resistin has also been found to be upregulated on TNFα stimulation and has been postulated as an important molecule triggering NF-κB activation and cytokine production in human peripheral blood mononuclear cells.12 Moreover, administration of recombinant mouse resistin into the knee joints of healthy mice induced leucocyte infiltration and hyperplasia of the synovia.12 These data support the hypothesis of resistin being an important member of the cytokine family with potent regulatory functions that might be involved in the pathogenesis of inflammatory diseases such as rheumatoid arthritis.
This study was designed to determine the difference in expression of resistin between rheumatoid arthritis and control osteoarthritis synovial tissue samples. Furthermore, serum and synovial fluid resistin levels in patients with different arthritides such as rheumatoid arthritis, spondylarthropathy (SpA) and osteoarthritis were analysed, and the hypothesis that resistin could be linked to the inflammation and/or disease activity of rheumatoid arthritis was evaluated.
PATIENTS AND METHODS
Patient characteristics
In all, 20 patients with active rheumatoid arthritis who met the 1987 revised criteria of the American College of Rheumatology,13 21 patients with knee osteoarthritis and 19 patients with different SpA (8 psoriatic arthritides and 11 ankylosing spondylitis) were included in the study. All patients were recruited from the Department of Rheumatology (Institute of Rheumatology, Prague, Czech Republic). The disease activity of patients with rheumatoid arthritis was assessed according to the 28 joint count Disease Activity Score (DAS28) using the number of swollen and tender joints, erythrocyte sedimentation rate (ESR) and patient’s global visual analogue scale (VAS).14 There were no statistical differences in terms of age, sex and body mass index (BMI) between patients with rheumatoid arthritis and those with osteoarthritis. Patients with SpA were younger than patients with osteoarthritis, and more men (n = 11) than women (n = 8) were included in the study. Patients with rheumatoid arthritis had signs of very active disease (median DAS28 = 6.0) and a wide range of disease duration (median 12 years, range 1–20 years). Most of the patients with rheumatoid arthritis (95%) and about 45% of the patients with SpA were treated with disease-modifying antirheumatic drugs (DMARDs). Only 3 of 19 patients with SpA, in contrast with 16 of 20 patients with rheumatoid arthritis, were treated with glucocorticoids. None of the patients in the study were treated with biologicals. Table 1 shows the patient details and their disease characteristics. All patients signed informed consent and the study was approved by the local ethics committee.
Characteristics of patients with rheumatoid arthritis, spondylarthropathies and osteoarthritis
Immunohistochemistry
Synovial tissue samples for immunohistochemistry were obtained from patients with rheumatoid arthritis (n = 9) and osteoarthritis (n = 6) at the time of arthroscopy or open joint surgery (Clinic of Orthopaedic Surgery, 1st Medical Faculty, Prague, Czech Republic). Sections of 5 μm thickness from formalin-fixed, paraffin-wax-embedded tissue were deparaffinised in xylene and rehydrated. Endogenous peroxidase activity was inhibited by 3% H2O2 in methanol for 30 min, followed by 15 min rinsing in tap water. Non-specific reactivity and binding was avoided by pretreatment of sections with 5% normal goat serum (Dako Cytomation, Glostrup, Denmark) and with 5% bovine fetal albumin for 2 h. The slides were incubated overnight at 4°C with rabbit anti-resistin serum (43–65)-NH2 (human; Phoenix Pharmaceuticals), diluted 1:1000 with ChemMate Antibody Diluent (Dako Cytomation), and with primary rabbit anti-resistin polyclonal antibody RD181016220 (Biovendor, Modrice, Czech Republic), diluted to 1:500 in ChemMate Antibody Diluent, respectively. The Histofine kit (Nichirei Corp., Tokyo, Japan) was used to visualise sections incubated with primary antibodies. The chromogen 3,3-diaminobenzidine (Liquid DAB+Substrate, Dako Cytomation) was applied to all sections and counterstaining was performed with Mayer’s haematoxylin. Tissue sections incubated with Rabbit Immunoglobulin Fraction (Dako Cytomation) diluted 1:1000 were used as negative controls.
Confocal laser scanning microscopy
Sections of 5 μm thickness were deparaffinised and rehydrated as described above. Double immunolabelling was performed as follows: slides were simultaneously incubated with primary mouse monoclonal antibodies CD138 clone B-B4 (Immunotech, Praha, Czech Republic), CD20cy clone L26 (Dako Cytomation), CD3 clone PC3 (Dako Cytomation), or CD68 clone KP1 (Dako Cytomation), respectively, and primary rabbit anti-resistin serum (43–65)-NH2, both diluted with ChemMate Antibody Diluent at 4°C for 1 h. Subsequently, simultaneous incubation of specimen with FITC/Cy5-conjugated secondary antibody, both diluted at 1:100 with phosphate-buffered saline (PBS) was performed at 4°C for 12 h. The slides were mounted in Mowiol (Hoechst, Frankfurt am Main, Germany), and observed in a confocal laser-scanning microscope Leica TCS SP (Leica Microsystems AG, Wetzlar, Germany). Simultaneous excitation with an argon–krypton laser at a wavelength of 448 nm for FITC and with helium–neon laser at a wavelength of 633 for Cy5 was used in the second step. Tissue sections incubated with Rabbit Immunoglobulin Fraction (Dako Cytomation) diluted 1:1000 were used as negative controls.
Microscopic analysis
All sections were analysed semiquantitatively using a Nikon Eclipse E600 microscope in a random order by two pathologists who were unaware of the clinical data. The intensity of resistin expression was scored on a four-point scale (0–3). In terms of the staining intensity, 0 represented lack of positivity, whereas a score of 1–3 represented weak, moderate and strong immunohistochemical positivity, respectively. In case of borderline staining intensity, the interobserver difference was solved by a secondary evaluation.
Ex vivo experiments
Synovial tissue samples obtained at the time of joint surgery from patients with rheumatoid arthritis (n = 3) and osteoarthritis (n = 3) were washed with sterile PBS and immediately removed into the sterile tubes supplemented with Dulbecco’s modified Eagle’s medium with 10% fetal calf serum, 10 mM HEPES, 50 IU/ml penicillin, 50 IU/ml streptomycin and 0.5 μg/ml amphotericin B. Subsequently, 100 μg samples were derived from each synovial tissue and incubated with 1.5 ml PBS at 37°C in 5% CO2 and 95% humidity. Eluates from synovial tissue samples were collected after 8 h and used for subsequent measurement of resistin synthesis.
Laboratory parameters
Blood samples were collected from all participants when they underwent therapeutical arthrocentesis. Paired samples were immediately centrifuged and both serum and synovial fluid were stored at −20°C. Serum, synovial fluid and eluate concentrations of resistin were measured by a commercially available ELISA kit according to the manufacturer’s protocol (Biovendor). CRP was measured by a the DSL-10-42100 Active US CRP ELISA according to the manufacturer’s protocol in sera from all patients (Diagnostic Systems Laboratories). In sera and synovial fluids from patients with rheumatoid arthritis we determined several other parameters such as IL1β, IL6, IL8, leptin, TNFα and monocyte chemoattractant protein (MCP)-1 using the Human Serum Adipokine (panel B) LINCOplex kit according to the manufacturer’s protocol (Linco Research).
Statistical analysis
Data were expressed as medians (SD) and analysed using the Mann Whitney U test (unpaired data) and the Wilcoxon test (paired data) for comparison of the two groups and the Kruskal–Wallis test for comparisons of the three groups using SigmaStat V.3. Linear regression was used to find a relationship between resistin and studied parameters. Spearman’s coefficient determined statistical significance. A p value <0.05 was considered statistically significant.
RESULTS
Resistin expression in synovial tissue
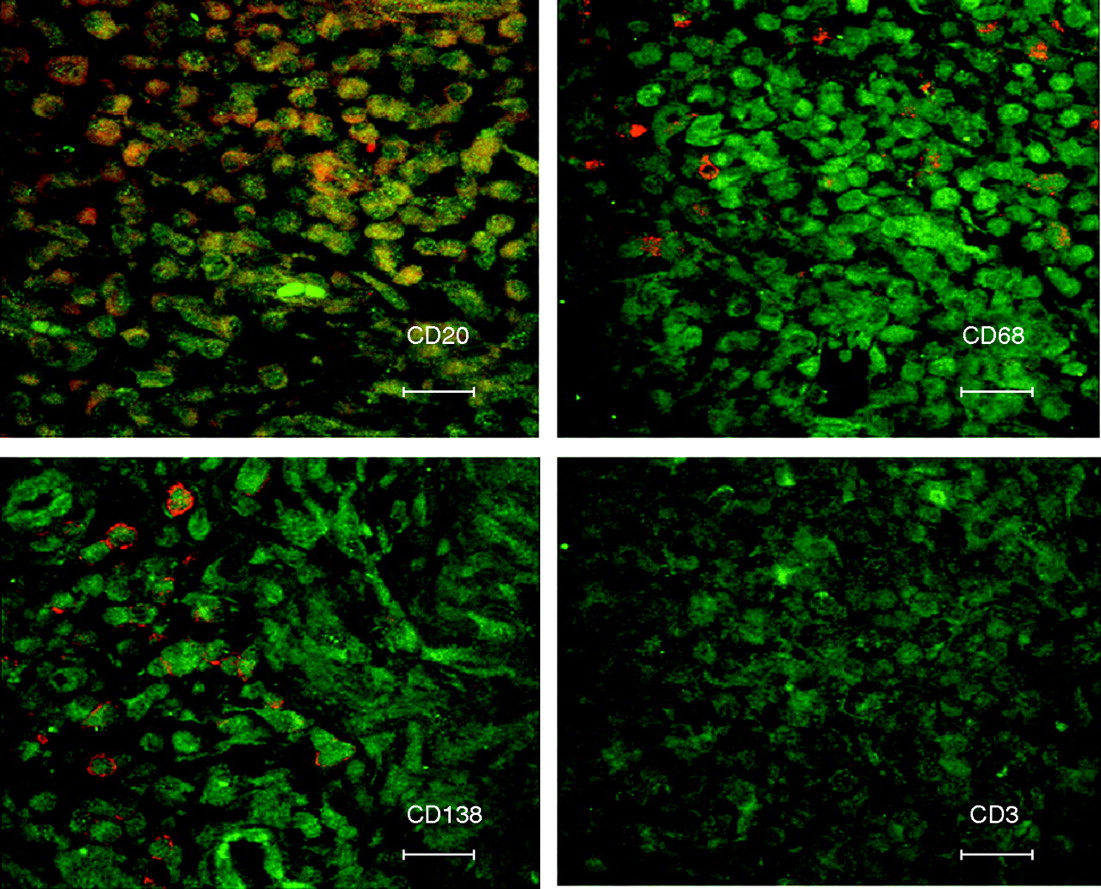
Resistin expression determined by rabbit anti-resistin serum (43–65)-NH2 (Human) (Phoenix Pharmaceuticals, Belmont, California, USA) and primary rabbit anti-resistin polyclonal antibody RD181016220 (Biovendor, Czech Republic) provided comparable results during testing (data not shown). For further staining, rabbit anti-resistin serum was used. Resistin expression was detected in both rheumatoid arthritis and osteoarthritis synovial tissues (fig 1). Synovial lining layer as well as vessel walls showed similar staining intensity both in rheumatoid arthritis and in osteoarthritis tissue samples. On the contrary, the synovial sublining layers expressed resistin with significantly higher intensity in rheumatoid arthritis than in osteoarthritis tissue samples (2.06 (0.76) vs 0.83 (0.41), p<0.01). Resistin was found in plasma cells, macrophages, B lymphocytes and some synovial fibroblasts. Immunophenotyping of all resistin-producing cells was confirmed with immunohistochemistry and confocal laser scanning using CD138 as a plasma cell marker, CD68 as monocyte/macrophage marker, CD3 as T cell marker and CD20 as B cell marker. Confocal microscopy showed a colocalisation of CD138, CD68 and CD20, but not of CD3 with resistin (fig 2). Double immunolabelling was performed to confirm the previous results (data not shown).

Resistin expression in rheumatoid arthritis synovial tissue (A). Synovial lining layer and vessel walls showed similar staining patterns in osteoarthritis synovial tissue (B), whereas sublining synovial tissue fibroblasts and inflammatory cells overexpressed resistin in rheumatoid arthritis in contrast with osteoarthritis tissue samples. Negative controls with rabbit immunoglobulin fraction are shown for rheumatoid arthritis (C) and osteoarthritis tissue samples (D). Original magnification ×100. The inset in (A) shows resistin expression by plasma cells in rheumatoid arthritis synovial sublining layer, original magnification ×400.

Confocal microscopy of rheumatoid arthritis synovial tissues showing colocalisation of resistin with CD20 B lymphocytes, CD68 monocytes/macrophages, CD138 plasma cells and CD3 T lymphocytes. Original magnification ×630.
Resistin levels in serum, synovial fluid and synovial tissue eluates
No statistical differences between rheumatoid arthritis and SpA serum resistin concentrations were found, but resistin levels in these patient groups were significantly higher than in patients with osteoarthritis (7.0 (3.0) and 6.0 (2.3) vs 4.4 (1.6) ng/ml, for both p<0.01; fig 3A). Synovial fluid resistin was highest in patients with rheumatoid arthritis, followed by patients with SpA and those with osteoarthritis (37.5 (13.4) vs 14.9 (12.1) vs 1.6 (0.8) ng/ml, respectively, p<0.001 for all comparisons) (fig 3B). In patients with SpA, synovial fluid resistin was also higher in contrast with patients with osteoarthritis (p<0.001). Resistin concentration in synovial fluid was significantly higher than in serum both in rheumatoid arthritis (37.5 (13.4) vs 7.0 (3) ng/ml, p<0.001) and in patients with SpA (14.9 (12.1) vs 6.0 (2.3) ng/ml, p<0.001). On the contrary, patients with osteoarthritis had lower resistin levels in synovial fluid than in serum (1.6 (0.8) vs 4.4 (1.6) ng/ml, p<0.001). Resistin levels in serum correlated with those in synovial fluid only in patients with osteoarthritis (r = 0.51, p = 0.02), but not in patients with rheumatoid arthritis (r = 0.33, p = 0.16) or in patients with SpA (r = 0.26, p = 0.27). Both serum and synovial fluid resistin levels were comparable between patients with ankylosing spondylitis and psoriatic arthritis in the SpA group (data not shown). The levels of serum and synovial fluid resistin in all groups were not influenced by the gender of the investigated individuals (female median 5.4 vs male 6.4 ng/ml, p = 0.27, and 15.0 vs 14.5 ng/ml, p = 0.35, respectively). When we analysed PBS eluates from synovial tissue samples, we observed substantially higher levels of resistin in rheumatoid arthritis samples in contrast with the osteoarthritis samples (1.90 (1.66) vs 0.14 (0.03) ng/ml).

{kind=link}
{kind=link}
{kind=link}
Serum (A) and synovial fluid (B) levels of resistin in patients with rheumatoid arthritis (RA), spondylarthropathy (SpA) and osteoarthritis (OA). The horizontal bar within the box represents the median; the boxes represent a range of ±25% around the median. Vertical bars indicate 95% CI.
Relationship of resistin with inflammatory status and rheumatoid arthritis disease activity
Serum CRP was highest in patients with rheumatoid arthritis, followed by patients with SpA and those with osteoarthritis (66.1 (40.8) vs 20.2 (30.7) vs 2.4 (7.2) mg/l). Serum resistin levels positively correlated with laboratory activity of rheumatoid arthritis as measured by US CRP (r = 0.53, p<0.02) and disease activity based on DAS28 (r = 0.44, p<0.05). Conversely, in both patients with osteoarthritis and those with SpA, no relationship between serum resistin levels and CRP was observed (r = 0.01, p = 0.95 and r = 0.03, p = 0.91, respectively). Synovial fluid resistin did not show any significant relationship with CRP in all studied groups (data not shown). To determine the relationship of resistin with selected adipose tissue derived factors and cytokines in patients with rheumatoid arthritis, we measured a set of markers including IL1β, IL6, IL8, leptin, TNFα and MCP-1. None of these markers correlated significantly with resistin in serum or in synovial fluid (table 2). In contrast with resistin, leptin tended to be higher, although not significantly, in serum than in synovial fluid, and its levels correlated significantly between those two body fluids (r = 0.70, p = 0.005). In addition, a positive association on the borderline of statistical significance was observed between serum resistin levels and disease duration in patients with rheumatoid arthritis (r = 0.40, p = 0.07). On the other hand, serum as well as synovial fluid levels of resistin did not correlate with age or BMI in all studied patients (data not shown). Patients with rheumatoid arthritis as well as those with SpA treated with and without glucocorticoids presented similar systemic resistin levels (7.0 (2.7) vs 5.9 (2.5) ng/ml, p = 0.60).
Serum and synovial fluid levels of selected adipose- and inflammatory-derived markers, and their correlations with resistin in patients with rheumatoid arthritis
DISCUSSION
This is the first study demonstrating the expression of resistin in synovial tissue. The intensity of resistin expression was significantly higher in the synovial sublining layer from patients with rheumatoid arthritis than those with osteoarthritis. Resistin was expressed by numerous different cell types including synovial fibroblasts, and several types of inflammatory cells residing in rheumatoid arthritis synovium such as macrophages, B lymphocytes and plasma cells, but not T lymphocytes. On the basis of both in vivo and ex vivo experiments, we could demonstrate that resistin is a secreted protein, and its increased serum levels may be directly linked to an enhanced inflammatory as well as disease activity status of patients with rheumatoid arthritis.
In mice and rats, adipose tissue and adipocytes are the major site of resistin production, whereas other tissues such as gastrointestinal tract, adrenal gland and skeletal muscles contribute less significantly.3,15 Our preliminary data on transgenic lipoatrophic A-ZIP mice that lack white adipose tissue show that their resistin levels are markedly reduced in contrast with both wild-type and morbidly obese ob/ob mice (Haluzík et al, unpublished data).16 In contrast with rodents, macrophages seem to be a major producer of resistin in humans.4 Recently, it has been suggested that resistin secreted from macrophages may represent a novel link between metabolic signals, inflammation and atherosclerosis,10,17 although some studies including our data failed to confirm this association.18 In our study, similar staining patterns and intensity for resistin were detected in the synovial lining layer in rheumatoid arthritis and osteoarthritis tissue samples, whereas there was a strikingly increased expression of resistin in the synovial sublining layer in the case of rheumatoid arthritis. We suggest that markedly increased resistin expression in rheumatoid arthritis synovium is a result of abundant accumulation of inflammatory cells in the rheumatoid arthritis synovial tissue. It has to be determined whether increased local expression of resistin precedes the development of joint inflammation in patients with rheumatoid arthritis and whether its circulating levels, synovial fluid levels and/or synovial tissue expression can be influenced by the treatment of the disease. It has been demonstrated previously that circulating levels of other adipocytokines such as leptin and adiponectin in patients with rheumatoid arthritis were not affected by treatment with biologicals.19
Resistin was expressed in numerous cell types within the synovial tissue in our study, including macrophages, which have been identified as a source of resistin by Jung et al.17 Here we demonstrate that other cell types such as plasma cells, B lymphocytes and synovial fibroblasts can also produce resistin. Moreover, in an ex vivo setting, we were able to show much higher resistin levels in eluates from rheumatoid arthritis in contrast with osteoarthritis synovial tissue samples when incubated with PBS. These findings support the idea that resistin may represent a novel secreted signalling molecule, that could be involved in the activation of the above-mentioned cell types during chronic inflammatory processes such as rheumatoid arthritis. We have previously shown that other inflammatory conditions such as hepatitis C or B also significantly increase circulating resistin levels.20
Resistin was originally discovered as a potential link between obesity and insulin resistance in rodents, and its role, especially in the development of liver insulin resistance has been clearly documented by later experimental studies.21 On the contrary, its exact pathophysiological role in humans is still a matter of debate. Our data, together with previously published papers, suggest that in humans resistin is more directly related to inflammation, whereas its relationship with insulin resistance has been documented only in some but not in all studies. For example, it was shown that, in vitro, resistin expression can be upregulated upon proinflammatory stimuli.9,12 Moreover, several inflammatory markers correlated well with plasma resistin levels in patients with metabolic disorders.10 In our study, serum resistin postitively correlated with ESR and CRP, but not with other pro-inflammatory cytokines such as IL6, IL8, TNFα or MCP-1. While synovial fluid resistin levels in patients with rheumatoid arthritis were markedly higher than its serum counterparts, the opposite was true for another adipocytokine leptin. Leptin concentrations were higher in systemic circulation than locally in synovial fluid, and it was related neither to resistin levels nor to other proinflammatory markers in body fluids from patients with rheumatoid arthritis. In agreement with Schäffler et al,11 we found significantly higher levels of resistin in the synovial fluid in the case of rheumatoid arthritis than in the case of osteoarthritis. Interestingly, we also detected higher serum resistin levels in patients with rheumatoid arthritis in contrast with control patients with osteoarthritis. This finding is in disagreement with recently published data12,22 showing no significant difference in blood resistin levels between patients with rheumatoid arthritis and healthy controls. The explanation for higher resistin levels in patients with rheumatoid arthritis from our study group may lie in the fact that our group consisted of patients with rheumatoid arthritis with more severe disease course as measured by acute-phase reactants and disease activity score. This is further supported by our finding that serum resistin levels correlated not only with inflammatory status (ESR, CRP) but also with the clinical disease activity (DAS28) in patients with rheumatoid arthritis. On the other hand, we did not see a significant relationship between increased synovial fluid resistin and inflammatory markers as shown previously.11,12 Furthermore, we did not confirm speculations that serum resistin levels would be reflected by those in synovial fluid in inflammatory arthritides.23 Taken together, it can be concluded that the joint compartment represents a major site of resistin production in patients with rheumatoid arthritis. Resistin levels in synovial fluid might reflect both the intensity of the inflammatory infiltrates within synovial tissue and the number of inflammatory cells within the synovial fluid. Since rheumatoid arthritis represents a condition with polyarticular involvement, we suggest that serum resistin levels could be more relevant to systemic inflammation and/or disease activity, whereas synovial fluid resistin reflects the particular inflammatory process of the affected joint.
Adipose tissue in males expresses higher levels of resistin than in females as shown in animal models.3 However, we did not find any influence of sex or age with regard to the resistin levels in human body fluids, which is in agreement with the previous study by Schäffler et al.24 Although we observed no influence of BMI on resistin levels, it can support the idea that resistin may be the link to inflammatory processes rather than to obesity or insulin resistance in humans. Moreover, numerous hormonal factors including glucocorticoids can regulate resistin levels. As glucocorticoids can increase resistin production,25 we could speculate that the increased resistin level in patients with rheumatoid arthritis is the result of glucocorticoid treatment. To further assess the possible influence of glucocorticoids on resistin level, we compared the subgroups with and without glucocorticoid treatment and found no significant differences between these two groups in terms of resistin levels. We thus suggest that mechanism(s) other than stimulation by exogenous glucocorticoids is (are) responsible for the increase of resistin levels in patients with rheumatoid arthritis. With regard to the recently published data by Bokarewa et al,12 the role of proinflammatory cytokines and a positive feedback loop (resistin itself) can be hypothesised as a cause for the upregulation of resistin under inflammatory conditions such as rheumatoid arthritis. Furthermore, exogenous resistin induced NF-κB activation, resulting in a strong upregulation of proinflammatory cytokines such as TNFα or IL6, and, when injected into healthy murine joints, induced synovial pannus formation and cartilage destruction.12
It has to be noted that the present study has several limitations. Firstly, it was designed as a cross-sectional study with a relatively low number of enrolled patients, and hence the role of DMARDs on the resistin levels in follow-up could not be determined due to this cross-sectional character. Secondly, the synovial tissue samples were obtained at the time of both arthroscopy and open joint surgery in our study. As recent work showed increased cell infiltration, expression of proinflammatory cytokines, matrix-degrading enzymes and growth factors in synovium obtained by arthroscopy in contrast with end stage destructive rheumatoid arthritis synovium obtained by total joint replacement,26 the possible influence of the tissue harvesting procedure on resistin expression has also to be taken into account.
In summary, we have shown markedly increased production of resistin at local sites of inflammation such as synovial tissue and synovial fluid in patients with rheumatoid arthritis. This local overproduction of resistin was also reflected by increased circulating resistin levels in patients with rheumatoid arthritis compared with those with osteoarthritis. Resistin was produced not only by activated macrophages but also by synovial fibroblasts and several other inflammatory cell types. The link between increased serum resistin, inflammation and disease activity of rheumatoid arthritis suggests a role of resistin as a novel proinflammatory mediator and supports the idea that, except for adiponectin,27 resistin may also play a role in chronic joint inflammatory diseases.
Acknowledgments
This study was supported by the Czech Ministry of Health (Research Project MZO 000064165).
REFERENCES
Footnotes
-
Published Online First 22 November 2006
-
Competing interests: None declared.