Article Text

Abstract
Objective To estimate the prevalence of spondyloarthritis (SpA) in reference to HLA-B27 in the French population.
Methods In 1989, 20 625 employees of the French national gas and electricity company aged 35–50 years were enrolled in the GAZEL cohort. In 2010, 18 757 still active participants were screened by a questionnaire validated for the detection of SpA. Responders with available DNA were retained for further studies. Pelvic radiograph and HLA-B27 typing were performed in all the self-reported cases of SpA or psoriatic arthritis. Self-reported diagnosis was verified by a qualified rheumatologist. HLA-B27 determination was also performed in subjects without any SpA feature.
Results The target population consisted of 6556 responders with available DNA. Their male:female ratio was 3.6 and their mean age was 65.5±3.3 years. A diagnosis of SpA was confirmed in 32 of the 72 self-reported cases, 75% of them being HLA-B27 positive. Estimated SpA prevalence adjusted for sex was 0.43% (95% CI 0.26% to 0.70%). HLA-B27 positivity rate in 2466 healthy controls was 6.9% (95% CI 5.9% to 7.9%). The relative risk of SpA in HLA-B27 positive individuals was 39 (95% CI 17 to 86).
Conclusions We estimated the prevalence of SpA in the French population in 2010 to 0.43%. With an estimated prevalence of 75.0% in SpA and 6.9% in healthy controls, HLA-B27 increased the disease risk 39-fold, as compared with HLA-B27 negative subjects.
- Ankylosing Spondylitis
- Spondyloarthritis
- Epidemiology
Statistics from Altmetric.com
Introduction
Spondyloarthritis (SpA) is a frequent chronic inflammatory disorder. Depending on its clinicoradiological presentation, it has classically been subdivided into the following subsets: ankylosing spondylitis (AS), psoriatic arthritis (PsA), arthritis associated with inflammatory bowel disease, reactive arthritis and undifferentiated SpA (uSpA).1 More recently, the Assessment of SpondyloArthritis international Society (ASAS) developed new classification criteria based on the anatomical distribution of rheumatic manifestations, subdividing the disease entity into axial SpA and peripheral SpA2, 3
Until now, most epidemiological studies in the field of SpA have been focused on AS. Recently, several studies have embraced all the SpA subtypes together 4 but only one of them has taken into account the ASAS classification criteria.5 One of the goals of these criteria was to allow the conduct of clinical trials for the treatment of non-radiographic SpA. Several studies using them have already been published and have showed response rates to tumour necrosis factor (TNF) blockers similar to those initially reported in AS.6 ,7 Thus, it seems important to obtain prevalence data according to ASAS classification criteria with regards to public health.
HLA-B27 is a major genetic factor of susceptibility for SpA. Its population prevalence has been previously estimated in many countries, leading to infer the proportion of HLA-B27 positive individuals expected to develop SpA,8 ,9 but to our best knowledge, such proportion has not been directly established in previous studies. HLA-B27 is one of few biological tests that may help with SpA diagnosis and is a key component of internationally validated classification criteria for SpA.2 ,3 Thus, it is important to determine its prevalence as precisely as possible to appreciate the diagnostic performance of the test.10
The aim of the present work was to estimate the population prevalence of SpA in reference to HLA-B27 in a cohort of French workers, the GAZEL cohort.
Subjects and methods
Subjects
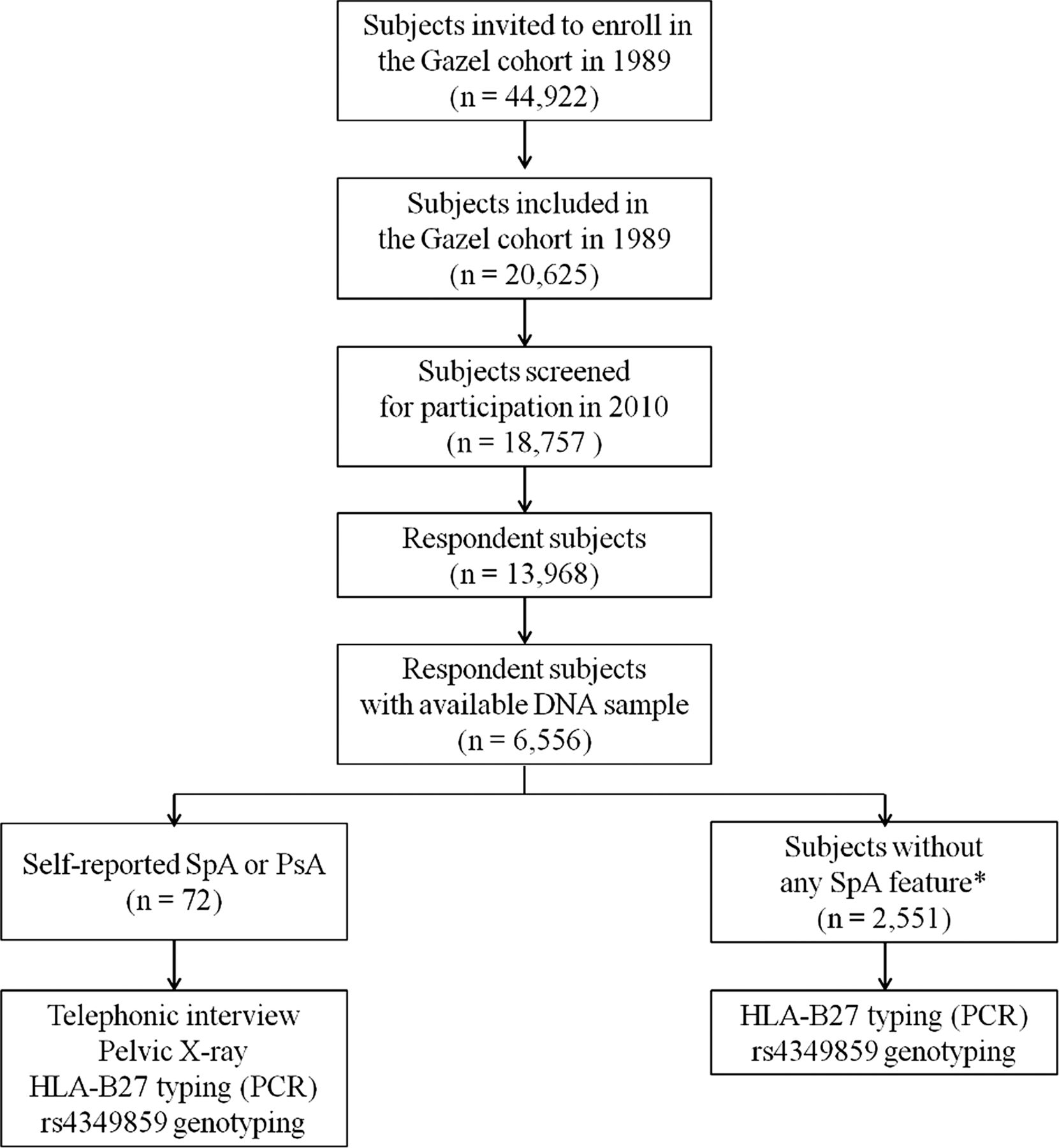
The GAZEL cohort is an ongoing general population-based cohort established among the employees of the French national electricity and gas company: Electricité de France-Gaz de France (EDF-GDF).11 This firm employs approximately 150 000 people of diversified socioeconomic statuses throughout France. The epidemiological profile of this population is very close to that of the French general population.12 Noteworthy, the staff of this company is very stable because they benefit from protective social advantages. In particular, employees of the company usually start their career while in their 20s and remain hired by the company, even if they become invalid or are unable to work because of chronic illness. These conditions minimised the risk of left-censoring effect in the cohort (ie, the risk of missing cases because their chronic illness would keep them away from the workforce). In January 1989, 44 922 persons (31 411male employees aged 40–50 years and 13 511 female employees aged 35–50 years) were invited to enrol in the cohort, of whom 20 625 accepted (15 011men and 5614 women). Each year, data on health, lifestyle, socioeconomic factors and occupational factors were collected via a mail questionnaire. Blood samples or buccal cells were stored for approximately a third of the participants. In 2010, the 18 757 remaining participants were invited to answer a medical questionnaire previously validated for the detection of SpA.13 All the responders with stored biological sample available for DNA extraction were kept for further analysis. This subset of subjects with stored biological sample was representative of the whole cohort with regards to most determinants.14 The study flow chart is shown in figure 1.

Study flow chart. SpA, spondyloarthritis.
The GAZEL protocol was approved by the French authority for data confidentiality (‘Commission Nationale Informatique et Liberté’) and by the Ethics Evaluation Committee of the ‘Institut National de la Santé et de la Recherche Médicale (INSERM)’ (IRB0000388, FWA00005831). Informed consent for this specific study was obtained from each participant and was approved by the local ethics committee of Ambroise Paré Hospital (Boulogne-Billancourt, France).
Screening and validation of SpA diagnosis
The screening questionnaire researched previous diagnosis of SpA or PsA as well as suggestive features of SpA as previously described.13 Performance of self-reported diagnosis of SpA, as previously reported in the French population for an estimated prevalence of the disease of 0.5% was close to 100% for negative predictive value and low for positive predictive value (9%).15
This is why patients with self-reported diagnosis of SpA or PsA were interviewed by phone by a qualified rheumatologist (RS-N) to verify clinical grounds of the diagnosis. For all the self-reported cases of SpA or PsA, anteroposterior radiograph of the pelvis and HLA-B27 typing were performed. Using available information, a diagnosis of SpA was confirmed or dismissed by RS-N, in reference to ASAS classification criteria for axial and peripheral SpA. Peripheral PsA cases that did not fulfil ASAS classification criteria for peripheral SpA (ie, patients with peripheral joint arthritis of symmetric distribution and predominating in the upper limbs, in a context of psoriasis but without other features of SpA) were classified separately.
All the subjects with available biological samples who had answered negatively to all the items in the questionnaire were considered as definite healthy controls from the perspective of SpA. Subjects who did not report SpA or PsA but who had answered positively to at least one item in the questionnaire were not investigated further.
Determination of HLA-B27 status
HLA-B27 status was determined in the suspected SpA cases and in the definite healthy controls. Two methods were used for this determination: allele-specific PCR and genotyping of the single-nucleotide polymorphism rs4349859, known to strongly tag the HLA-B27 allele.16
DNA extraction
DNA was extracted from stored buccal cells (n=927) or blood samples (n=1694). Buccal cells had been collected with a sterile cytobrush (Histobrush, Hardwood Products Company, USA) by twirling it on the inner cheek. Blood sample had been obtained by venipuncture and buffy coat was then isolated and stored. DNA was extracted with QIAamp DNA Blood Midi and Mini kit (QIAGEN, Valencia, California, USA) from buffy coats and cytobrushes, respectively.
HLA-B27 status determination
Exon 2 and exon 3 of the HLA-B locus were amplified with HLA-B27 specific primers (Forward: GGTCTCACACCCTCCAGAAT, Reverse: GCGTCTCCTTCCCGTTCTCA) together with GAPDH primers (Forward: ACCACAGTCCATGCCATCA, Reverse: CCACCACCCTGTTGCTGT) as internal control. Detection of the amplified products was carried out by means of 2% agarose gel electrophoresis.
Genotyping of rs4349859 was performed using Taqman genotyping assay (Applied Biosystems, Foster City, California, USA) according to the manufacturer's recommendations.
Statistical methods
Continuous variables were expressed as mean±SD. Crude and sex-adjusted prevalences were estimated. Adjusted prevalence was calculated based on the sex distribution in the source population as determined by the last national census (2010).17 The 95% CIs were constructed using the logit transformation.18 To evaluate SpA prevalence according to HLA-B27 status, we estimated the number of HLA-B27 positive subjects based on HLA-B27 typing in healthy controls and individuals having reported SpA. Categorical variables were compared using the χ2 test and continuous variables using the Student t test. The level of type I error used to determine statistical significance was 5%. Statistical analyses were performed with R for Windows, V.2.15.1.
Results
Characteristics of the population
As shown in figure 1, 18 757 subjects (91% of the initial cohort) were screened for participation by a dedicated questionnaire. The overall response rate was 74.5%. Among the responders, 6556 had stored buccal cells or buffy coat sample available for DNA extraction, representing 34.9% of the screened cohort. They constituted the target population for the rest of the study. Participants included in this study were not different from the whole GAZEL cohort, except for being more often retired and having a higher socioeconomic level.
SpA prevalence
Seventy-two subjects reported to have AS, SpA or PsA. As shown in figure 2, a diagnosis of SpA was confirmed in 32 of them, a diagnosis of peripheral PsA in 7 of them and another diagnosis in 28 of them. In two cases, diagnosis remained doubtful. Clinical characteristics of the confirmed cases are summarised in table 1 and presented in detail in online supplementary table S1. All the confirmed cases fulfilled ASAS classification criteria for SpA and 75% of them were HLA-B27 positive (80% of the AS cases and 67% of the other SpA cases).
Clinical characteristics of confirmed SpA cases

{kind=link}
{kind=link}
Diagnosis flow chart. PsA, psoriatic arthritis; SpA, spondyloarthritis.
The overall sex-adjusted estimated prevalence of SpA was 0.43% (95% CI 0.26% to 0.70%). Table 2 shows the prevalence of SpA, according to age, sex and HLA-B27 status. There was no statistically significant difference in prevalence according to age or sex.
Prevalence of SpA in the GAZEL cohort in 2010
HLA-B27 prevalence in healthy controls
Individuals having answered negatively to all items of the arthritis questionnaire (n=2551, ie, 38.9% of the target population) were considered as definite healthy controls and used for HLA-B27 status determination, by allele-specific PCR.
Overall, 6.9% (95% CI 5.9% to 7.9%) of the tested samples were HLA-B27 positive. There was no significant difference between men and women. However, a trend towards a lower rate of HLA-B27 was observed in subjects older than 70 years (5.1%; 95% CI 3.4% to 7.4%), as compared with younger subjects (7.3%; 95% CI 6.2% to 8.6%), that was close to significance (p=0.06) (table 3). The relative risk of developing SpA in HLA-B27 positive individuals, as compared with HLA-B27 negative ones was 39 (95% CI 17 to 86).
Prevalence of HLA-B27 in healthy controls of the GAZEL cohort in 2010
The minor allele frequency of rs4349859 (corresponding to allele A which tags HLA-B27) was 6.8% (95% CI 5.9% to 7.9%). In comparison with HLA-B27 PCR results, rs4349859 showed high specificity (99.7%) and sensitivity (97.0%) for HLA-B27 detection.
Discussion
Accurate public health planning requires reliable epidemiological data to be effective. Although several recent studies have estimated the prevalence of SpA,4 as far as we know, the present study is the first to estimate SpA and HLA-B27 prevalence in a single large-scale cohort. Moreover, to our knowledge, it is the first to report the prevalence of SpA in the general population, according to ASAS classification criteria, since Strand et al5 studied SpA prevalence in US rheumatology practices. By screening subjects aged more than 56 years old in the French GAZEL cohort, we estimated SpA prevalence around 0.43% and that of HLA-B27 carriers around 6.9% in healthy controls and 75.0% in patients with SpA.
Such SpA prevalence appears higher than the 0.3% value reported by Saraux et al19 from a survey conducted in the French adult population, in 2001, albeit the 95% CI of estimate overlaps between both studies. Such discrepancy can be explained by the fact that the age of subjects investigated here was ≥57 years. Given that a diagnosis of SpA is, most of the times, made before the age of 50 years,20 one can assume that the present study yielded a nearly approximate value of the cumulative risk of developing SpA in the French population. Consistent with other recently published studies, we observed no significant variation in prevalence according to sex.19 ,21 AS was by far the most common subtype of SpA in our study (69%), which may appear different from other studies, in which PsA and/or uSpA were found to be more frequent than AS.9 ,19 ,22 Two major factors could explain such apparent discordance. First, a pelvic radiograph was obtained in SpA cases in a systematic fashion only in our study. Second, subjects in the present study were older than in the previous ones at the time of ascertainment and some of those presenting at first with uSpA or PsA could have progressed to AS over time.23 ,24
To estimate SpA prevalence, it is important to target a general population sample and not only patients who have been referred to a rheumatologist. This is why we have used the GAZEL cohort, which is composed of subjects from all French regions and of various socioeconomic statuses. Several studies have shown that the epidemiological profile of the cohort is close to that of the French general population in terms of distribution of disorders and causes of death.25 ,26 Nevertheless some bias could be seen as a limitation to generalisation of those results in the entire French population. First, there was a high proportion of men in the cohort. Second, all the subjects were more than 55 years old. Third, GAZEL participants were volunteers, thus subject to a selection effect potentially associated with their health status.27 Fourth, French nationality is required to be employed in EDF-GDF, thus ethnic variability in the cohort was lower than in the general population.
However, such potential biases should be very limited: the prevalence rate of SpA was similar between men and women and we calculated sex-adjusted prevalence. Although elderly onset of SpA is possible,28 we can consider that very few cases should occur later given the age of the population studied and that we have estimated here the cumulative prevalence of SpA. Thus we did not adjust prevalence for age. It is unlikely that having a SpA could introduce a selection bias in EDF-GDF recruitment. Indeed, mean age at recruitment in the company was around 20 years and once recruited, all the individuals remained in the company and were proposed to enter the cohort, even in case of work disability or long-term illness. Moreover, in previous studies having assessed confounding factors in the GAZEL cohort, rheumatic condition was not associated with initial participation nor was it associated with attrition during follow-up.12 ,29 All these data support that the GAZEL cohort can be considered as representative of the French Caucasian population.
As another possible source of bias, our screening was based on self-reported diagnosis so that we might have missed some undiagnosed cases, in particular in those individuals who had declared some SpA features. Again, previously reported negative predictive value of self-reported SpA being close to 100%, such bias should be minor.15 Self-reported diagnoses were validated by phone interviews by a qualified rheumatologist. Previous reports suggested that telephone survey may represent a reliable alternative to face to face interview15 ,19 with no major differences in the responses obtained by the two methods.30
In the present study, the estimated HLA-B27 prevalence in the French population was 6.9% in controls, a result close to that of a recent study reporting a HLA-B27 prevalence of 7.5% in non-Hispanic white subjects, in USA31 We inferred a 39-fold relative risk of developing SpA in HLA-B27 positive individuals, as compared with B27 negative individuals. Braun et al reported a lower relative risk in HLA-B27 individuals from the Berlin population (20.7) but the SpA prevalence used to estimate it (1.9%) was probably overrated in their initial study.32
Interestingly, a trend towards a lower rate of HLA-B27 positivity was found in subjects older than 70 years. In our study, the lowest rate of B27 was observed in persons born during World War II. Since many epidemics have occurred during this period in France, it may suggest a higher susceptibility of HLA-B27 positive individuals to tuberculosis or other unidentified infectious disease.33 This observation is reminiscent of that recently reported in the US population by Reveille et al31 in subjects aged 50–69 years. The shift observed in age range may reflect differences in pathogens exposure between France and USA.
We assessed the presence of HLA-B27 by direct PCR genotyping and also by genotyping rs4349859, a surrogate marker for B27.16 Our study showed good agreement between both methods. Thus, we confirmed that genotyping rs4349859 is a highly specific method to detect HLA-B27 that can be used to screen large population samples, particularly for epidemiological studies.
In conclusion, cumulative SpA prevalence in the French population in 2010 was slightly higher than that previously reported in France in 2001, with a high proportion of AS. Although less than 5% of HLA-B27 carriers have developed SpA, disease relative risk conferred by this antigen was high with a 39-fold increase. The trend towards decreased HLA-B27 rate in older subjects could also suggest another role for this molecule with a possibly higher childhood-related mortality in HLA-B27 carriers due to exposure to infection risk having vanished since the 1950 s in France.
Acknowledgments
The authors thank Dr Joëlle Benessiano and the Hospital Bichat-Claude Bernard Biological Resource Center (CRB-BCB, Paris, France) for DNA extraction and storage of GAZEL samples.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
FC and AT contributed equally.
-
Contributors All the authors contributed to the manuscript based on (1) substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published.
-
Funding This work was supported by grant from Agence Nationale de la Recherche (grant ANR 2010 GEMISA). FC was supported by a grant from Société Française de Rhumatologie (SFR). AT was supported by a grant from Arthritis Fondation Courtin. The GAZEL Cohort Study was funded by EDF-GDF and INSERM, and received grants from the ‘Cohortes Santé TGIR Program’, Agence nationale de la recherché (ANR) and Agence française de sécurité sanitaire de l'environnement et du travail (AFSSET).
-
Competing interests None.
-
Ethics approval Ethical comity of Lorraine, Ambroise-Paré Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.