Article Text

Abstract
Objectives Inflammatory arthritis (IA) can lead to anxiety, depression, pain and fatigue. Psychological support can improve quality of life and self-management; and European and American guidelines recommend support be offered. This study examined patient views on psychological support for their IA.
Methods A questionnaire designed by researchers, patient partners and clinicians was administered to 2280 patients with IA.
Results 1210 patients responded (53%): 74% women; mean age 59 years (SD 12.7); patient global 5 (2.3); disease duration <5 years (41%), 5–10 (20%), >10 (39%). Only 23% reported routinely being asked about social and emotional issues by a rheumatology professional, but 46% would like the opportunity to discuss psychological impact. If offered, 66% of patients reported they would use a self-management/coping clinic (63% pain management, 60% occupational therapy, 48% peer support groups, 46% patient education, 46% psychology/counselling). Patients want support with managing the impact of pain and fatigue (82%), managing emotions (57%), work and leisure (52%), relationships (37%) and depression (34%). Preferences are for support to be delivered by the rheumatology team (nurse 74%, doctor 55%) and general practitioners (GPs) (51%). Only 6% of patients stated that social and emotional issues were not relevant.
Conclusions Demand for psychological support is high; however, less than a quarter of patients reported being asked about social and emotional issues, suggesting a gap between needs and provision. The preference is for delivery from rheumatology clinicians and GPs, and research should establish whether they have the skills and resources to meet patients’ needs.
- Health services research
- Patient perspective
- Psychology
Statistics from Altmetric.com
Introduction
While there is no evidence that patients have primary psychological disturbances, the diagnosis of a long-term condition can increase the risk of developing depressive symptoms with lasting psychological effects.1 Inflammatory arthritis (IA) refers to a group of long-term rheumatic diseases, the most common of which is rheumatoid arthritis (RA). IA is characterised by pain, joint swelling, stiffness and fatigue, often resulting in functional disability.2 The prevalence of anxiety and clinical depression in rheumatic diseases is about twice the prevalence seen in the general population.3 A study with recently diagnosed patients found that at all time points during the 10-year follow-up, 20–30% had clinically important levels of anxiety and 5–13% had clinically important levels of depression.4 At a milder level, the occurrence of psychological distress that does not fulfil diagnostic criteria of anxiety and depression (e.g. negative affective states such as low mood, sorrow, worry, irritability, apprehension, insomnia and restlessness) is estimated to be as high as 65%.5
Evidence suggests that in RA disease status and disease activity alone are not good predictors of psychological distress,6 ,7 and factors such as illness beliefs, locus of control and coping strategies are influential.8–10 Psychological interventions have been shown to enhance medical regimes of care by improving coping and self-efficacy, and reducing functional disability and pain.11 ,12 For example, cognitive behavioural therapy, which examines the links between thoughts, beliefs and feelings that drive behaviours, has been shown to prevent psychological and physical morbidity, facilitate adjustment and reduce long-term use of healthcare resources.13–15 Mindfulness, meditation and relaxation have also been shown to be a safe and effective means of reducing distress and improving well-being in patients with RA.16 ,17 The psychological consequences of IA are increasingly recognised, with American and European treatment guidelines recommending that clinical management address patients’ psychosocial functioning.18–21
To facilitate adherence to guidelines and inform the allocation of healthcare resources requires information on the acceptability and applicability of different psychological support services from the patient perspective.22 For example, recent research found that patients wanted emotional support from a professional, regarding it as beneficial to share problems with someone outside of their social environment.23 There is some evidence that different psychological factors affect coping and adaptation at different stages, making disease duration and disease trajectory (e.g. flares or drug changes due to toxicity) potentially important considerations in targeting timing of psychological support.24 One point when psychological support might be particularly helpful is close to diagnosis, and research has identified a wish for support to be explicitly offered at this time.25 Left unaddressed, patients’ early psychological response to their IA might have long-term implications, for example, psychological distress 4 years postdiagnosis has been found to correlate highly with initial psychological distress.26 In other studies, no statistically significant differences were found for anxiety, depression and acceptance of illness between those with short disease duration (<1 year) compared with those with longer disease duration (>10 years),27 and anxiety was not found to be related to RA disease duration.28 Data are sparse in relation to modality; however, as the use of computerised and mobile devices to deliver health-related interventions becomes more widespread, there might be an increasing preference among patients for online support services.29
Despite the acknowledgement of the psychosocial impact of IA, data are lacking on patient views of current levels of psychological support from the rheumatology team and on patient preferences for the type, timing and mode of delivery of future services. Therefore, this study had two aims. The first was to collect data on patients’ perceptions of the levels of support they had received for the social and emotional impact of IA. The second was to collect data on patients’ preferences for types of psychological support including when services might be delivered and by whom.
Participants and methods
A brief questionnaire was designed by the research team, comprising rheumatology and psychology clinicians, patient partners and researchers, who agreed on questions addressing personal experience of social and emotional support received from the rheumatology team; and patient preferences for psychological support, including type of service, provider, mode of delivery and areas for help (see online supplementary file 1). The questionnaire was piloted with six patients to check clarity and the inclusion of relevant domains from the patient perspective. The feedback indicated that there were no problems and that the questionnaire took approximately 10 minutes to fill in.
To capture a range of views, participants were recruited through a national patient RA charity and rheumatology units in six regional hospitals across England, selected to reflect diverse geographical locations and serving differing communities in relation to urbanity/rurality and socioeconomic makeup. The only inclusion criteria were patients over 18 years old with a confirmed diagnosis of a form of IA and either a member of the patient charity or attending an outpatient appointment at one of the collaborating hospital sites. The patient charity mailed the questionnaire to 1200 patients selected randomly from their membership database, and subsequently placed a generic reminder in an electronic newsletter. In each of the six hospital sites, a member of the local team handed out 180 questionnaires to consecutive patients attending outpatient appointments and mailed a reminder approximately 2 weeks later. Whether recruited through the patient charity or an outpatient's clinic, all questionnaires were completed anonymously and returned directly to the central research team in a prepaid envelope.
Results
Questionnaire data were entered into an Excel spreadsheet by hand, and distributions of the responses (numbers and percentages) for each response category were calculated. A total of 1210 patients responded (53%), with rates ranging from 33% to 98% at the hospital sites and 44% among the patient charity members invited to take part (table 1).
Response rates
Due to the lower response rate at site F, their demographic and clinical data were compared with sites A–E to see whether respondents differed in relation to sex, age, ethnicity, living arrangements, disease duration and patient global assessment of overall health (see online supplementary file 2). However, no differences were identified, with site F scores within the ranges of the other five sites for all the variables examined. Data from the patient charity and the six hospital sites have been presented both in combination and separately because the sampling and recruitment processes differed (table 2).
Demographic and clinical data
The percentage of respondents who reported being asked about social and emotional issues by a rheumatology professional (this could include doctors, nurses, occupational therapists and physiotherapists) was 23%, but 46% would have liked the opportunity to discuss psychological impact. Two-thirds of respondents (66%) reported that they would use a self-management/coping clinic (63% would attend pain management, 60% occupational therapy, 48% peer support groups, 46% patient education, 46% psychology/counselling) if the service were offered. This percentage was slightly higher for the patient charity respondents and slightly lower for the hospital sites respondents (figure 1). The preference would be for psychological support to be delivered by the rheumatology team (nurse 74%; doctor 55%) and general practitioner (51%). Other preferred sources would be family (49%) and friends (35%), other people with arthritis (37%) and patient support groups (33%), written/online information (31%), psychologist/counsellor (29%) and occupational therapist (27%). Only 3% of respondents stated that they would prefer not to talk about social and emotional difficulties and not to receive any support. There were some small differences between the samples, with patient charity respondents expressing a greater preference for all the different providers of support compared with the hospital site respondents, except for ‘family member’ (figure 2).

Patient preferences for type of psychological support service, if offered (n=1194).
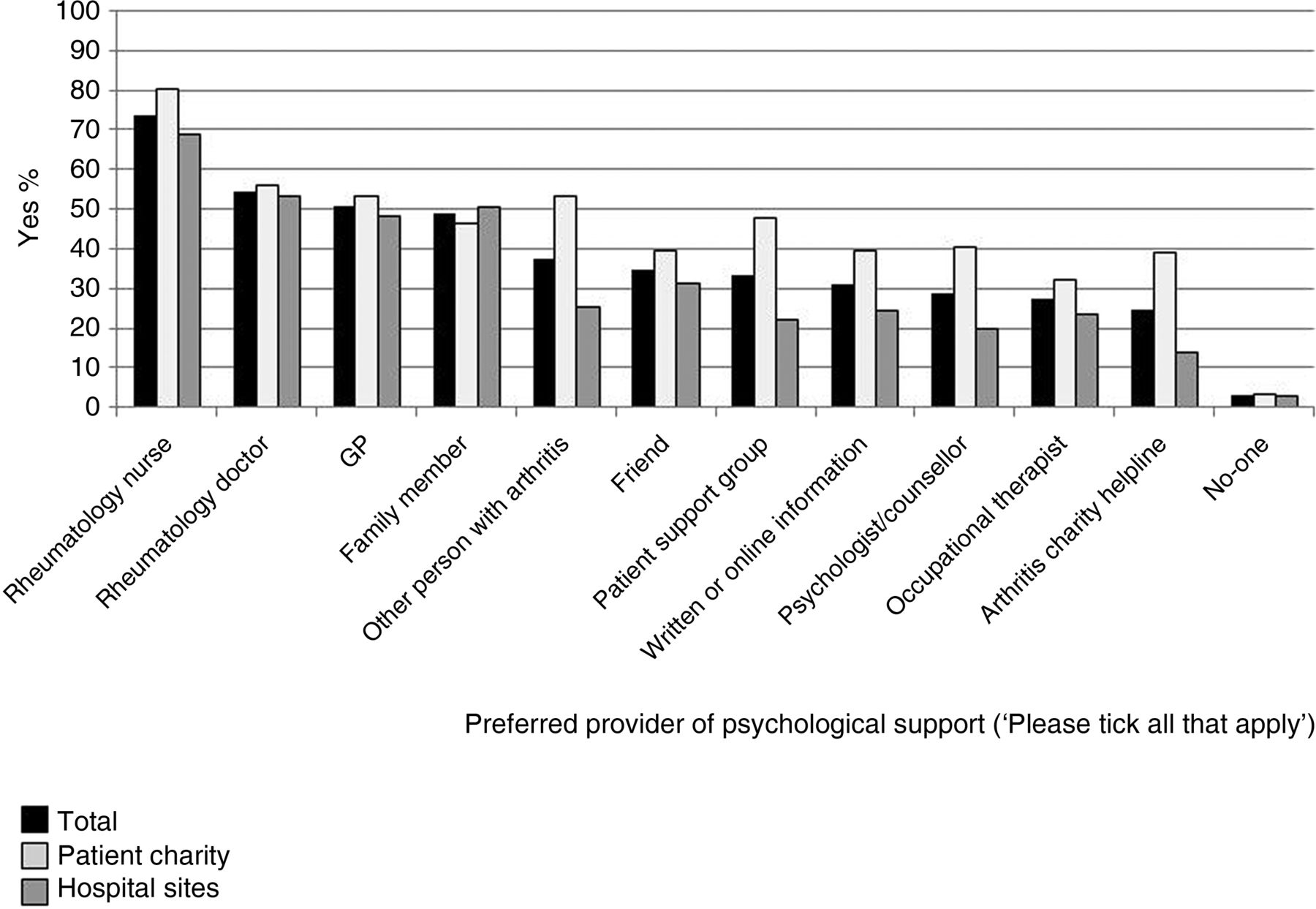
Patient preferences for provider of psychological, social and emotional support (n=1201). GP, general practitioner.
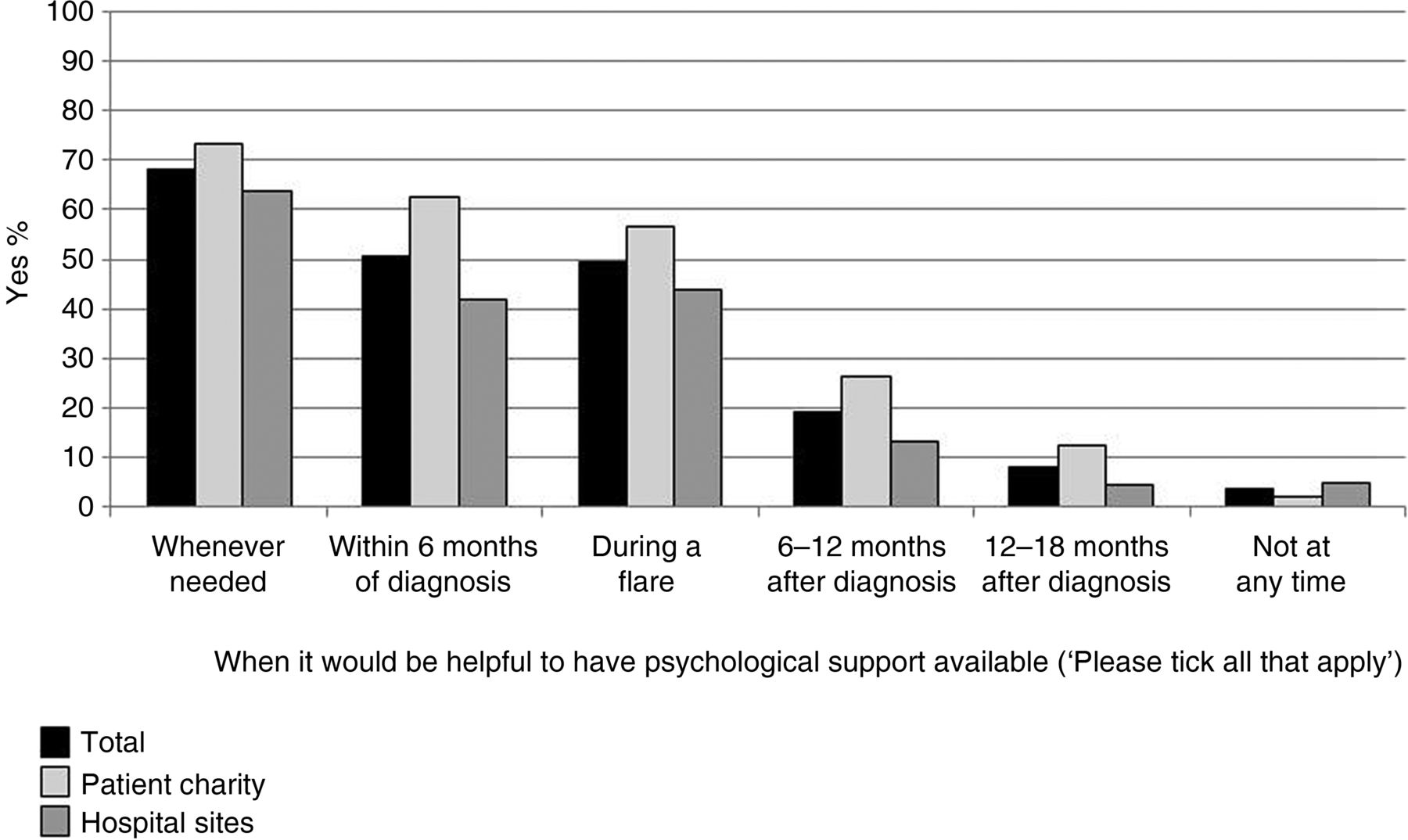
The preferred mode of delivery was stated to be face-to-face (80%) compared with telephone (14%) and email/online (8%). Patients want support to manage the impact of IA in relation to symptoms such as pain and fatigue (82%); emotions such as low mood, anxiety and stress (57%); the effects on work and leisure (52%); relationships with family and friends (37%); and depression (34%) (figure 3). Support might include help with relaxation techniques (42%) and talking to others with arthritis (36%). Only 6% of respondents stated that social and emotional issues were not relevant. Preferred timing for psychological support would be whenever needed (68%), within 6 months of diagnosis (51%) and during a flare (49%); only 4% of respondents reported that they would choose not to use psychological support services at any time (figure 4).

Patient preferences for areas of support in relation to disease impact (n=1199).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patient preferences for timing of psychological support provision (n=1200).
Discussion
The psychological status of patients can be described on a continuum from adaptive coping, through disease-related distress, to psychological and psychiatric conditions. The questionnaire used in this survey was designed to capture views on a range of areas of support, from dealing with the impact of common symptoms, such as pain and fatigue, through to managing depression. This survey found that the demand for psychological support was substantial, with very low numbers reporting that they would not wish to receive any support at any time. It also found that almost half of the respondents reported that they would like the opportunity to discuss social and emotional issues, but less than a quarter were being asked by their rheumatology team. These data do not provide information on the dialogue between clinicians and patients; however, the discrepancy could indicate a gap between needs and provision.
Two-thirds of respondents reported that they would use a self-management/coping clinic if the service were offered. Facilitating effective self-management involves supporting patients to adjust to a range of disease consequences, which can include symptoms, disability, uncertainty, loss of independence, fear and depression, anger, loneliness, sleep disorders and stress.30 Over half of the respondents indicated a preference for support to deal with the impact of their IA in relation to symptoms such as pain and fatigue, emotions, and work and leisure. Research has shown that how patients manage symptoms and physical disability influences their ability to engage in meaningful, valued activities, including the domains of work, family life, leisure and social relationships.31 Over a third of respondents stated that they would want help with managing depression, while very few respondents preferred not to receive any support, ticking the option that social and emotional issues are not relevant.
The issues that patients want help with have implications for who is best placed to deliver support services. This survey found clear preferences for the rheumatology team to provide these services, with three quarters of respondents identifying the rheumatology nurse as one of their ideal sources of support. By contrast, just under a third of respondents also named a psychologist or counsellor, indicating that fewer patients perceived a need to access the services of specialist psychology professionals. These findings fit with a stepped approach to psychological care, in which patients are treated at the lowest appropriate intervention level in the first instance, only stepping up to more intensive services as clinically required.32 There is increasing recognition that the rheumatology team, with their understanding of the disease and its treatment, can play a vital therapeutic role in helping patients with IA to increase their sense of control and improve their psychological well-being,33 and these survey findings suggest that patients would find this acceptable and useful. Other research has highlighted the value of nurse-led, patient-centred care for improving patients’ coping and emotional states,34 ,35 and European guidelines recommend that nurses provide psychosocial and self-management support.36 In light of evidence that access to psychological services is limited for patients with RA, the finding has significant implications for service delivery and policy development.37 In addition to the patient perspective, there is evidence that rheumatology teams view psychological support as part of their remit, but further research is needed into their skills training and resource needs if such care is to become integrated into routine practice.38 ,39
Respondents in this survey were overwhelmingly in favour of face-to-face delivery of psychological support compared with computer-based interventions, reflecting findings from previous research at a single site over 10 years ago.40 However, this preference needs to be seen in the context of more recent evidence that some internet-based programmes have been shown to be effective.41 It might be that for specific groups (e.g. patients in remote locations) or specific issues (e.g. self-management), online support is appropriate. While half of the respondents want support to be available within 6 months of diagnosis, over two-thirds reported that they would prefer to access it whenever needed. Prospective research has shown that adjustment to the disruption of a long-term condition unfolds over time and that there is heterogeneity in trajectories across patients.42 Influential factors include interpersonal relationships, personality attributes, cognitive variables and coping processes. Many of these factors would be addressed through the types of services that respondents say they would use, such as self-management and pain management programmes.
A key strength of this survey study was the involvement of patient partners (AP, JC) from design through to interpretation of the findings. Examples where their input was particularly influential included developing a definition of psychological support in relation to IA and making potentially important distinctions in the questionnaire response options, such as help with low mood as distinct from support for depression. The findings were further strengthened by the large sample size recruited from diverse sites, increasing the likelihood that the data reflected a range of views. Although the study was conducted in the UK, the literature suggests commonalities in the psychological impact of IA across Europe and North America; therefore, these findings on patient preferences for psychological support might be relevant to patients internationally.3 ,43
A limitation of the survey was the considerable variation in the response rates. A contributory factor might have been the resources available locally to support research. For example, site E had a research nurse and a dedicated room in the rheumatology unit where patients could complete the questionnaire. However, there were no differences between the six sites in relation to patients’ data (i.e. their preferences for psychological support provision). The collaborating sites and the patient charity were not aware of which patients took part in the survey and no information was collected on who did not respond and why, meaning we could not check for response bias. However, the percentage of white British respondents was higher than that in the IA population, suggesting that patients from other ethnic backgrounds were more likely to be non-responders. This has implications for the design of support services as there is evidence that ethnicity influences support priorities and needs.44 It could be, for example, that those patients with greater psychological support needs were more likely to have completed the questionnaire. Furthermore, the questionnaire asked about support that patients would want, but it cannot be known how this would translate into uptake in clinical practice if such provision were offered.
Conclusions
This survey indicates that the demand for psychological support is high across the disease trajectory, but few patients reported being asked about social and emotional issues, suggesting a gap between needs and current provision. In particular, patients would like to have support to manage the impact of their IA in relation to symptoms such as pain and fatigue, emotions, and work and leisure. The preference is for delivery from rheumatology clinicians, in particular rheumatology nurses, and research should explore whether teams can be taught the skills and can use resources to meet patients’ needs.
Acknowledgments
The authors thank the patients who participated in the study and the National Rheumatoid Arthritis Society (NRAS) and collaborating hospital sites and for their support in administering the survey.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online supplement
Footnotes
Handling editor Tore K Kvien
Contributors ED was involved in the study conceptualisation and design, and data collection, analysis and interpretation. CA was involved in the study design, data collection, analysis and interpretation. JC, AP, JP and SH were involved in the study conceptualisation and design, data analysis and interpretation. NA was involved in the study conceptualisation and data interpretation. All authors read drafts of the manuscript and approved the final version.
Funding Grant support: Arthritis Research UK, grant number 19755.
Competing interests None.
Ethics approval The National Research Ethics Service Committee (North East: County Durham & Tees Valley).
Provenance and peer review Not commissioned; externally peer reviewed.