Article Text

Abstract
Objectives To define disease activity levels, minimal clinically important improvement (MCII) and patient-acceptable symptom state (PASS) with the primary Sjögren's syndrome (SS) disease activity indexes: European League Against Rheumatism (EULAR) SS disease activity index (ESSDAI) and EULAR SS patient-reported index (ESSPRI).
Methods For 790 patients from two large prospective cohorts, ESSDAI, physician evaluation of disease activity, ESSPRI and patients’ satisfaction with their current health status were recorded. Receiver operating characteristic curve analyses and anchoring methods were used to estimate disease activity levels of ESSDAI and the PASS of ESSPRI. At follow-up visit, patients and physicians assessed, respectively, whether symptoms and disease activity have improved or not. An anchoring method based on this evaluation was used to estimate MCII of ESSDAI and ESSPRI.
Results Low-activity (ESSDAI<5), moderate-activity (5≤ESSDAI≤13) and high-activity (ESSDAI≥14) levels were defined. MCII of ESSDAI was defined as an improvement of at least three points. The PASS estimate was defined as an ESSPRI<5 points and MCII as a decrease of at least one point or 15%.
Conclusions This study determined disease activity levels, PASS and MCII of ESSDAI and ESSPRI. These results will help designing future clinical trials in SS. For evaluating systemic complications, the proposal is to include patients with moderate activity (ESSDAI≥5) and define response to treatment as an improvement of ESSDAI at least three points. For addressing patient-reported outcomes, inclusion of patients with unsatisfactory symptom state (ESSPRI≥5) and defining response as an improvement of ESSPRI at least one point or 15% seems reasonable.
- Sjøgren's Syndrome
- Outcomes research
- Patient perspective
Statistics from Altmetric.com
Primary Sjögren's syndrome (SS) is a systemic disorder primarily characterised by lymphocytic infiltration of exocrine glands, resulting in functional impairment of salivary and lachrymal glands. The inflammatory process however extends beyond the exocrine glands and can potentially affect any organ.
As a result, clinical features can be divided into two facets for which two disease activity indexes have been recently developed by the European League Against Rheumatism (EULAR) SS task force: the EULAR SS disease activity index (ESSDAI)1 for systemic features and the EULAR SS patient-reported index (ESSPRI)2 for patients’ symptoms. These indexes have been developed to be used as outcome measures in clinical trials and improve clinical research in the field of primary SS. Both indexes have been validated. They have been shown to be valid, reliable and sensitive to change.3 ,4 Sensitivity to change was, however, better for ESSDAI than ESSPRI.
This study aimed at defining disease activity levels of ESSDAI, patient-acceptable symptom state (PASS) with ESSPRI and minimal clinically important improvement (MCII) of these two disease activity indexes. The objective was also to help determine the most effective way of conducting clinical trials for evaluation of new treatments in primary SS and to suggest thresholds to be used as entry criteria and response criteria.
Patients and methods
PATIENTS
EULAR cohort
Between 2009 and 2011, 395 patients with primary SS, according to the American-European Consensus Group (AECG) criteria,5 from 14 countries were prospectively included by 30 experienced investigators participating in this international EULAR collaborative project (project code CLI 010). This 6-month study aimed to validate ESSDAIs.3 Investigators were asked to include approximately half of patients with systemic features, and therapeutic management was left to their discretion. This study was conducted with the approval of the institutional review board of GHU Paris Nord (n°IRB0006477). In each country, local ethical requirements have been observed.
ASSESS cohort
Between 2009 and 2011, 395 patients with primary SS according to AECG were included from 15 centres of Rheumatology and Internal Medicine in France in the ‘Assessment of Systemic Signs and Evolution of SS’ (ASSESS) 5-year prospective observational cohort that aim to identify predictive factors of systemic complications.6 ,7 Therapeutic management was left to the discretion of treating physician. Data from baseline and the first year were analysed in the present study. Both cohorts included the same number of patients by chance.
MEASUREMENT
All specific questions are provided in online supplementary file 1.
Disease activity indexes
Status measures
At enrolment, physicians assessed systemic disease activity of each patient with a 4-point Likert scale (inactive, low, moderate or high) and a 0–10 numerical scale. They also completed ESSDAI. ESSDAI theoretically ranges from 0 to 123 but observed values rarely exceed 40. To remind them to distinguish between activity and patients symptoms, they were asked also to separately assess patients’ symptoms with a 0–10 numerical scale. They also determined whether their patients were in minimal disease activity (MDA) state. A definition of MDA was provided, according to that used for rheumatoid arthritis.8 ,9 In the EULAR cohort, all these scales were reassessed at 6 months.
Measures of change
At follow-up visit, physicians evaluated the change in disease activity according to a five-point Likert scale (much worse, worse, the same, better and much better).
Patient-centred measures
Status measures
At enrolment and at follow-up visit, all patients completed ESSPRI. ESSPRI ranges from 0 to 10. At the 6-month visit in the EULAR cohort, the patient’s acceptability/satisfaction of its current state (taking account of his symptoms: dryness, fatigue and pain) was also recorded.
Measures of change
In the EULAR cohort at the follow-up visit, patients evaluated the change in their state according to a five-point Likert scale (very importantly improved, importantly improved, slightly improved, no change, worsened). To detect improvement, patients also assessed whether their current health status has importantly improved with a binary question.
STATISTICAL ANALYSES
Quantitative data are presented as mean±SD or median with IQRs. The 95% CIs for quantiles (median, upper quartile) were calculated based on a method that is distribution-free that uses order statistics (ranks) to compute the confidence limits as described by Hahn and Meeker.10
The following analyses aimed at defining disease activity levels of ESSDAI, PASS of ESSPRI and MCII of ESSDAI and ESSPRI. Analyses were performed in the two cohorts. If the results were reasonably similar, the estimates were integrated to obtain the final criteria. These final criteria were then tested for different aspects of external validity on data of all clinical trials11–16 where ESSDAI and/or ESSPRI have been measured, whatever their positive and negative results. The aim was to assess their ability to discriminate between placebo and treated arms.
Definition of disease activity levels with ESSDAI
This step involved two distinct statistical methods.
Receiver operating characteristic curve analysis
Physicians’ evaluation of disease activity was used as an external standard to determine the activity levels. For each cut-off, we computed a separate receiver operating characteristic (ROC) curve and calculated its sensitivity and specificity. For determining the cut-off of low-disease activity, we looked for the ESSDAI score that better discriminated between patients with inactive or low activity versus those with moderate or high activity. For the cut-off of high-disease activity, we looked for the ESSDAI score that better discriminated between patients with high activity compared with all other patients. For each cut-off, we selected the ESSDAI score having the maximal Youden index.17
Anchoring method according to MDA status
Two groups of patients were considered: those in MDA (MDA group), and those not (non-MDA group). For each group, we then identified the 75th centile of the ESSDAI values. This upper quartile determined the threshold between low and moderate activity in the MDA group and the threshold between moderate and high activity in the non-MDA group.18
External validation
The threshold of moderate activity was foreseen to be used as an entry criterion in randomised control trials (RCTs) evaluating immunosuppressants or biologics. We then estimated, from these two cohorts3 ,6 and from clinical trials,11–16 the number of patients that would have been eligible according to the obtained thresholds. We retained the one sufficiently discriminating to select patients with active disease, but not too restrictive, so as not to limit recruitment for RCTs.
Determination of minimal clinically important improvement (MCII) with ESSDAI
MCII was estimated using an anchoring method based on the physician's assessment of evaluation of change in disease activity. MCII was estimated in the population of patients considered as ‘better’. MCII was computed both as absolute and relative change of ESSDAI. MCII estimates were defined as the median value of the change in ESSDAI score in the population judged as improved.19 ,20 To assess whether MCII estimates were above measurement error, we also calculated the minimal detectable change (MDC) with 95% confidence level using the following formula (MDC=1.96*√2*SEM). MDC provides another threshold that helps interpretation, that is, when a score change exceeds this level, there is reasonable certainty that it is true signal, and not just noise or error.21
External validation
In an RCT, MCII may be used as response criteria. We examined, using the different MCII estimates, what would have been the response rates in the placebo and active treatment arms of clinical trial.11–16 Among them, we retained the minimal threshold having the best ability to discriminate between placebo and treated arms.
Definition of PASS with ESSPRI
PASS is defined as the value beyond which patients consider themselves well. The concept of PASS for patients’ measures of symptoms is similar to the concept of low-disease activity for systemic disease activity measures.22–24 However, they did not necessarily overlap, particularly in pSS where patients' symptoms and disease activity did not correlate.7
This step comprised also two distinct methods, performed in the two cohorts.
ROC curve analysis
ROC curves were computed for various cut-offs of ESSPRI score to calculate the sensitivity and specificity. To determine PASS, we looked for the ESSPRI score that better discriminated between patients who considered themselves in a satisfactory state and those not. We selected the optimal cut-off of ESSPRI as the one having the maximal Youden index.17
Anchoring method
Two groups of patients were determined: those considering their current health status as satisfactory (PASS group) and those not (non-PASS group). PASS was defined as the 75th centile of ESSPRI distribution in the PASS group.23
Final criteria and external validation
PASS threshold of ESSPRI might be used as entry criteria in RCTs evaluating symptomatic treatments. We estimated, from these two cohorts3 ,6 and recent trials,11–16 ,25 the number of patients that would have been eligible using the estimated cut-offs. We retained the one that correctly classified the highest number of patients.
Determination of MCII with ESSPRI
To estimate MCII, an anchoring method based on the patient's assessment of evaluation of change in symptom state was used. MCII was estimated by focusing on the population of patients who were considered as being ‘importantly and slightly improved’. MCII was computed both as absolute and relative change of ESSPRI. MCIIs estimates were defined as the median value of the change (absolute or relative) in ESSPRI score in this target population. We performed the same analyses in the patients that answered to the binary question that they considered their current health status as importantly improved.
External validation
To assess the relevance of the obtained MCII estimates as response criteria and to assess whether a rounded value performed the same as a precise estimate, we examined for each threshold what would have been the response rates in placebo and treated arms of previous trials.11–16 We finally retained the MCII thresholds based on their ability to discriminate between placebo and treated arms and its ease of use.
All statistical analyses involved the use of SAS release V.9.3 (SAS Institute, Cary, North Carolina, USA) and R release V.2.2.7 (The R Foundation for Statistical Computing, Vienna, Austria) statistical software packages.
Results
Patients’ characteristics
The EULAR cohort (table 1) included 395 patients with a median ESSDAI score of 6 (IQR=2–12) and a median ESSPRI score of 6 (IQR=4.3–7.3). A total of 350 patients (88.6%) have been followed until the 6-month visit. The ASSESS cohort (table 1) included 395 patients with a median ESSDAI score of 2 (IQR=0–7) and a median ESSPRI score of 5.7 (IQR=4.0–7.0), of whom 371 (93.9%) have been followed until the 1-year visit.
Characteristics of primary Sjögren's syndrome patients
Definition of disease activity levels with ESSDAI
Using both anchoring method and ROC curve analysis, in the ASSESS cohort and at the 6-month visit in the EULAR cohort, the estimates of low-disease activity were similar (ESSDAI<5) (table 2). However, this threshold was higher at the baseline visit of the EULAR cohort due to the inclusion of patients with more active disease. The threshold of 5 was therefore retained. Except for the JOQUER trial and for the ASSESS cohort that included principally patients with low-disease activity, we estimated that 60.0–93.3% of the patients from all recent trials and from the EULAR cohort had an ESSDAI score ≥5 at inclusion (table 3).
Tentative cut-off of disease activity levels with ESSDAI and PASS with ESSPRI
ESSDAI and ESSPRI baseline values in real-life cohorts and clinical trials
The estimates of high-disease activity were similar (ESSDAI≥14) in both cohorts and at each visit, whatever the method used. According to this threshold, a high disease activity was found in 23.9% (92/385) and 10.2% (39/383) of the patients of the EULAR and ASSESS6 cohorts, respectively, and 35/122 (28.7%), none, 10/119 (8.4%), 4/30 (13.3%) and 5/15 (33.3%) of the patients from TEARS,12 rituximab trial from the Netherlands,14 JOQUER,13 BELISS16 and ASAP trials,15 respectively.
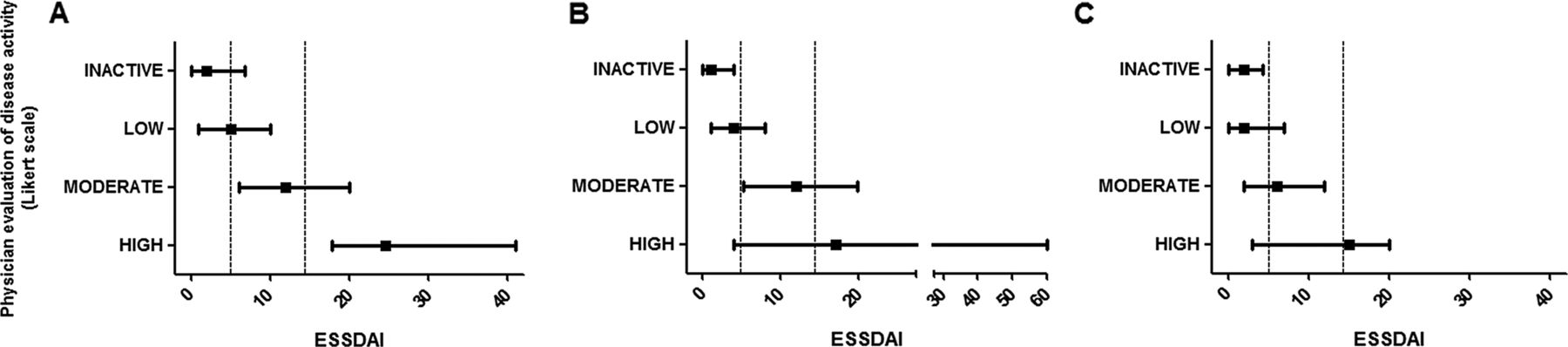
Thus low-activity, moderate-activity and high-activity levels were defined by an ESSDAI<5, between 5 and 13 and ≥14, respectively (figure 1).

{kind=link}
Distribution of European League Against Rheumatism Sjögren's syndrome disease activity index (ESSDAI) score according to disease activity levels. In patients from European League Against Rheumatism (EULAR) cohort at inclusion (A), at 6 months (B) and in the Assessment of Systemic Signs and Evolution of SS (ASSESS) cohort (C). Vertical dot lines represents disease activity thresholds of moderate activity (ESSDAI=5) and high activity (ESSDAI=14). ESSDAI score distribution is represented with mean value (square) and IQR, in each subgroups of activity as assessed by the physicians.
Determination of MCII in disease activity with ESSDAI
In each cohort, MCII estimates were obtained for the whole cohort and in the population of patients having at least moderate activity at inclusion (table 5). From these results, three thresholds were considered: improvement of two, three or four points of ESSDAI. Since relative estimates were not concordant between the two cohorts, only absolute changes were retained. For each threshold, we estimated from data from recent trials the response rate in the placebo and treated arms (table 4). MDC was 4.4 and 2.7 in the EULAR and ASSESS cohorts, respectively. These thresholds were just below those of MCII estimates in each cohort. We finally retained an improvement of at least three points of ESSDAI as MCII since this threshold was the one that better discriminated between placebo and treated arms.
Definition of MCII with ESSDAI and ESSPRI
Definition of PASS with ESSPRI
The PASS estimates (table 2) were similar across cohorts whatever the method used. The two estimates of 5 and 6 were tested to assess how they discriminated between PASS and non-PASS groups. The threshold of 5 was the one that classified the higher number of patients (see online supplementary table S1). Even less specific, this threshold was more sensitive and less restrictive for inclusion of patients in clinical trial. This threshold was particularly sensitive to identify patients from the non-PASS group and identify 76.1–81.8% of these patients. Thus PASS was defined as an ESSPRI<5.
Determination of MCII in patients’ symptoms with ESSPRI
MCII estimates were obtained from the EULAR cohort: in the whole cohort and in the population of patients having ESSPRI≥5 at baseline (table 4). In these two populations, MCII estimates were, respectively, 0.67 and 1 point, whatever the question and answer modality used; and relative MCII estimates were 10% and 15% of the baseline value, respectively. Both estimates differentiated similarly between placebo and active treatment arms. We finally retained an improvement of ESPPRI of at least one point for its ease of use, and the corresponding relative estimate of decrease of at least 15% of the baseline value as MCII (table 5).
Relevance of MCII tentative cut-offs for ESSDAI and ESSPRI
Discussion
This study aimed to determine disease activity levels, PASS and MCII of the EULAR SS indexes, ESSDAI and ESSPRI. This study involved patients with primary SS from two large independent cohorts, one of which had been conducted internationally and specifically for that purpose. The results displayed reliable thresholds for defining activity levels and changes in scores that could be used for designing future clinical trials. Nevertheless, since the number of observational cohorts already used ESSDAI and ESSPRI for the evaluation of their real-life patients,6 ,26 the usefulness of these thresholds in clinical practice will be further evaluated.
Our study has some limitations. Both cohorts were observational; therefore, no therapeutic intervention was systematically applied. This might have affected the evaluation of clinically relevant changes. Nevertheless, to date no treatment has formally demonstrated superiority versus placebo. In addition, since therapeutic management was left to the discretion of the treating physician, when treatment was needed, patients were treated. Furthermore, this limitation has been encompassed by the use of external anchors to assess whether the patient’s condition has changed. In the EULAR cohort, physicians were instructed to include approximately half of the patients with systemic complications, not in the ASSESS cohort. This might explain why at the baseline visit in the EULAR cohort the estimates of disease activity levels were slightly higher than at the 6-month visit and that in the ASSESS cohort. Nevertheless, these discrepancies also underlined the fact that in multisystem disease with multiorgan involvement, such as pSS, no single score can perfectly ‘translate’ expert’s evaluation of disease activity.
The treatment of primary SS remains a challenge. Effectively, whatever the drug used, hydroxychloroquine,13 tumour necrosis factor-blockers11 ,27 and even B-cell-targeted therapies, such as rituximab,12 most of the RCTs did not achieve their primary endpoints. Regarding rituximab, the results remains however controversial with positive results in a small trial14 and at 6 weeks in a larger recent study, but not confirmed at 24 weeks.12 However, since not available, none of these trials used a systemic disease activity measure as the primary outcome, but patient-reported outcomes or dryness measures, which have been shown to be less sensitive to change.3 In addition, some of the recent trials used ESSDAI as a secondary outcome and found it sensitive to change.15 ,16 ,28 ,29
Learning from these results, methodological insight was needed to improve the design of clinical trials in primary SS. The present study helps addressing main methodological questions for designing RCT: determining the key inclusion criteria and defining response criteria.
Better definition of inclusion criteria is a key issue. The objective is to select the patients who are most likely to benefit from the treatment in order to increase the chances of demonstrating treatment efficacy. For biologics or immunosuppressants, they might be a combination of factors, such as the inclusion of patients with active systemic complications, very early and/or biologically active disease.16 ,30 An alternative, or complementary, approach is to require a minimal ESSDAI score, such as moderate activity threshold (ESSDAI≥5), to ensure inclusion of patients with active disease. We showed that most of the patients in recent trials had at least moderate activity, which demonstrates that this will not be a limit for recruitment in future RCTs.
The other key issue is to determine an optimal primary endpoint. To evaluate biologically active and immunosuppressive drugs, preferentially dedicated to patients with active systemic disease, the use of more objective endpoints, for example, ESSDAI, seems preferable. This study had determined MCII of ESSDAI (decrease of at least three points), which can be a first step for the definition of response criteria. The MCII value was of five points in the EULAR cohort and three points in the ASSESS cohort, both above the respective MDC found in each cohort. Thus, an MCII of 3 is the minimal required, but it can be increased in case of trials involving highly systemic patient populations.
In systemic lupus erythematosus (SLE), such a process of determining better definition of inclusion criteria to select active patients more likely to respond to treatment31 and using a powerful response criteria (the SLE responder index32) has been applied with success to show the effectiveness of belimumab.33 ,34
Even though in clinical practice most of patients with pSS has low-disease activity, a part of patients had severe systemic complications. Nevertheless, among these systemic patients who might require and/or benefit from immunosuppressive treatment or biologic, we might keep in mind that patients included in the RCTs have usually less severe systemic manifestations than those treated in real life. Effectively, the most severe patients cannot be exposed to the risk of receiving placebo. This might explain the discrepancies between the results of RCTs and real-life experience, as for rituximab.35 Also, this might make it more difficult to demonstrate drug efficacy since RCTs mainly included patients with mild to moderate activity. Therefore, even though they are less sensitive to change, a PRO such as ESSPRI can be considered as an outcome in an RCT whatever the drug used. Effectively, PROs and particularly ESSPRI or its individual components have been shown to significantly improve in some recent trials.14–16 The treatment of chronic diseases finally aims to improve quality of life and patient-perceived health status. PROs are the only tools addressing this issue. Thus, considering the inclusion of patients having an ESSPRI above the threshold of unsatisfactory symptom state (ESSPRI≥5) and a defining response as an improvement of ESSPRI MCII (ESSPRI decrease of at least one point or 15%) might also be considered for future clinical trials.
In conclusion, this study, including two large cohorts of patients, has defined disease activity levels, PASS and MCII of ESSDAI and ESSPRI. Hopefully this will help to homogenise and determine the most effective way to conduct clinical trials. To evaluate treatments of systemic complications, the proposal is to include patients with at least moderate activity (ESSDAI≥5) and to define response to treatment as an improvement of ESSDAI of at least three points. For addressing patient-reported outcomes, inclusion of patients with unsatisfactory symptom state (ESSPRI≥5) and defining response as an improvement of ESSPRI of at least one point or 15% seems reasonable. The choice of ESSDAI or ESSPRI or a combination of both will depend on the type of the drug to evaluate the study design and remains to be determined by future studies.
Acknowledgments
The authors would like to thank patients with pSS included in the EULAR cohort; EULAR for its grant to the project; Prs Maxime Dougados, Alan Tyndall, Daniel Aletaha and Désirée van der Heijde for their guidance and support; the EULAR house in Zurich for their hospitality and outstanding organisation (Ernst Isler and his associates). They also thank patients with pSS included in the ASSESS cohort; Direction de la Recherche Clinique (DRC) de l’Assistance Publique des Hôpitaux de Paris and Myriem Carrier; Djilali Batouche, Karine Inamo, Stanie Gaete, Laina Ndiaye, Helene Agostini and Laurent Becquemont (Unité de Recherche Clinique Paris Sud); Mickael Randrianandrasana, Isabelle Pane, Gabriel Baron (Epidémiologie et Santé Publique, Hotel Dieu); the French Society of Rheumatology for its grant to the cohort.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online questions
- Data supplement 2 - Online table
Footnotes
Handling editor Tore K Kvien
Collaborators Members of the EULAR Sjögren's Task Force who participated in this study: Elena Bartoloni and Roberto Gerli, Rheumatology Unit, Department of Clinical and Experimental Medicine, University of Perugia, Italy; Stefano Bombardieri, Rheumatology Unit, Department of Internal Medicine, University of Pisa, Italy; Hendrika Bootsma, Cees Kallenberg, Department of Rheumatology and Clinical Immunology, University Medical Center Groningen (UMCG), Groningen, Netherlands Simon J Bowman, Rheumatology Department, University Hospital Birmingham, Birmingham, UK, Johan G Brun, Department of Rheumatology, Haukeland University Hospital, Bergen, Norway; Roberto Caporali, Department of Rheumatology, University of Pavia, IRCCS S. Matteo Foundation, Pavia, Italy; Salvatore De Vita, Clinic of Rheumatology, University Hospital of Udine, University of Udine, Udine, Italy; Valerie Devauchelle and Alain Saraux, Rheumatology Department, la Cavale Blanche Teaching Hospital, Brest, France; Thomas Dörner, Rheumatology Department, Charité, University Hospital Berlin, Berlin, Germany; Anne-Laure Fauchais, Department of Rheumatology, University Hospital, Limoges, France; Jacques Eric Gottenberg, Department of Rheumatology, Strasbourg University Hospital, Strasbourg, France; Eric Hachulla, Department of Internal Medicine, Claude Huriez Hospital, Lille, France; Aike A Kruize, Departments of Rheumatology and Clinical Immunology, University Medical Center, Utrecht, The Netherlands; Thomas Mandl and Elke Theander, Department of Rheumatology, Malmö University Hospital, Lund University, Sweden; Xavier Mariette, Frederic Demoulins and Raphaèle Seror, Department of Rheumatology, Bicetre Hospital, Le Kremlin Bicêtre, France; Petra Meiners, Department of Oral and Maxillofacial Surgery, University of Groningen, University Medical Center Groningen, P.O. Box 30.001, 9700 RB Groningen, The Netherlands; Carlomaurizio Montecucco, Department of Rheumatology, University of Pavia, Pavia, Italy; Wan-Fai Ng, Musculoskeletal research group, University of Newcastle, Newcastle, UK; Sonja Praprotnik and Matija Tomsic, Department of Rheumatology, University Medical Centre, Ljubljana, Slovenia; Manel Ramos Casals and Pilar Brito-Zerón, Laboratory of Autoimmune Diseases ‘Josep Font’, Hospital Clinic, Barcelona, Spain; Philippe Ravaud, Center of Clinical Epidemiology, Hopital Hotel Dieu, Paris, France; Hal Scofield and Kathy L. Sivils, Arthritis and clinical immunology, Oklahoma Medical research foundation, Oklahoma City, USA; Roser Solans Laqué, Departement of Autoimmune systemic Diseases, Vall d’Hebron University Hospital, Barcelona, Spain; Takayuki Sumida, Department of internal medicine, university of Tsukuba, Japan; Susumu Nishiyama, Rheumatic disease centre, Kurashiki medical centre, Kurashiki, Japan; Athanasios Tzioufas, Department of Pathophysiology, School of Medicine, University of Athens, Greece, Roberta Priori and Guido Valesini, Department of Medicina Interna e Specialità Mediche, Rheumatology Clinic, La Sapienza University of Rome, Rome, Italy; Valeria Valim, Division of Rheumatology, Department of Medicine, Federal University of Espírito Santo, Brazil; Claudio Vitali, Sections of Rheumatology, Instituto San Giuseppe, Como and Casa di Cura di Lecco, Lecco, Italy, Cristina Vollenweider, Department of Rheumatology, German Hospital, Buenos-Aires, Argentina. And members of the ASSESS cohort who participated in this study: Valerie Devauchelle and Alain Saraux, Rheumatology Department, la Cavale Blanche Teaching Hospital, Brest, France; Jean-Jacques Dubost, Department of Rheumatology, Clermont-Ferrand, France; Anne-Laure Fauchais, Department of Rheumatology, University Hospital, Limoges, France; Vincent Goeb, Department of Rheumatology, Amiens university hospital, Amiens, France; Jacques-Eric Gottenberg and Jean Sibilia, Department of Rheumatology, Hôpitaux Universitaires de Strasbourg, Strasbourg, France; Eric Hachulla, Department of Internal Medicine, Claude Huriez Hospital, Lille, France; Gilles Hayem, Department of Rheumatology, APHP-Hôpital Bichat, Paris, France; Pierre- Yves Hatron, Department of Internal Medicine, Hôpital Claude Huriez, Lille, France; Claire Larroche, Department of Internal Medicine, Hôpital Avicenne APHP, Paris, France; Veronique Le Guern and Xavier Puéchal, National Referral Center for Rare Systemic Auto-immune Diseases, Cochin Hospital AP-HP, Paris, France; Jacques Morel, Departement of Immuno-Rheumatology, Lapeyronie University Hospital, Montpellier, France; Aleth Pedriger, Department of Rheumatology, University Hospital, Rennes, France; Stephanie Rist, Department of Rheumatology, Hôpital de la Source, Orléans, France; Damien Sene, Department of Internal Medicine, Hôpital La Pitié–Salpêtrière, APHP, Paris, France; Olivier Vittecoq, Department of Rheumatology, Rouen University, Rouen, France, Claire Zarnitsky, Department of Rheumatology, Le Havre Hospital, Le Havre, France.
Contributors Conception and design: RS and PR. Analysis and interpretation of data: RS, GB, XM and PR. Drafting the article or revising it critically for important intellectual content, acquisition of data and final approval of the version published: all authors.
Funding The EULAR Sjogren’s task force collaborative project (project code CLI 010) received a grant from EULAR. The ASSESS national multicentre prospective cohort (Assessment of Systemic Signs and Evolution in Sjögren's Syndrome) was set up in 2006 thanks to a grant of the French Ministry of Health (Programme Hospitalier de Recherche Clinique 2005: P060228).
Competing interests None.
Patient consent Obtained.
Ethics approval The study, promoted by Assistance Publique-Hôpitaux de Paris (Programme Hospitalier de Recherche Clinique 2005: P060228), was approved by the Ethics Committee of Hôpital Bichat and the ‘Commission Nationale Informatique et Libertés’ in 2006. All patients gave their informed written consent. Institutional review board of GHU Paris Nord (n°IRB0006477).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data are available upon request.