Article Text

Abstract
Objectives Some studies have reported a possible association between exposure to tumour necrosis factor (TNF) inhibitors and an increased risk of melanoma. The aim of this study was to investigate the incidence of invasive cutaneous melanomas in patients with rheumatoid arthritis (RA) treated with TNF inhibitors (TNFi), other biologic disease modifying drugs and non-biologic therapy.
Methods Eleven biologic registers from nine European countries participated in this collaborative project. According to predefined exposure definitions, cohorts of patients with RA were selected. Using the country-specific general population of each register as reference, age, sex and calendar year standardised incidence ratios (SIRs) of invasive histology-confirmed cutaneous melanoma were calculated within each register. Pooled SIR and incidence rate ratios (IRRs) comparing biologic cohorts to biologic-naïve were calculated across countries by taking the size of the register into account.
Results Overall 130 315 RA patients with a mean age of 58 years contributing 579 983 person-years were available for the analysis and 287 developed a first melanoma. Pooled SIRs for biologic-naïve, TNFi and rituximab-exposed patients were 1.1 (95% CI 0.9 to 1.4), 1.2 (0.99 to 1.6) and 1.3 (0.6 to 2.6), respectively. Incidence rates in tocilizumab and abatacept-exposed patients were also not significantly increased. IRR versus biologic-naïve patients were: TNFi 1.1 (95% CI 0.8 to 1.6); rituximab 1.2 (0.5 to 2.9).
Conclusions This large European collaborative project did not confirm an overall increased risk of melanoma following exposure to TNFi.
- Rheumatoid Arthritis
- Anti-TNF
- Epidemiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Invasive cutaneous malignant melanoma (hereafter referred to as melanoma) is the sixth most frequently diagnosed cancer in Europe with an age standardised incidence rate of 11.1 per 100 000 in 2012.1 The incidence of melanoma varies across European countries, with rates highest in northern Europe.2 Melanoma is immunogenic and patients with impaired immunity, for example, due to solid organ transplantation or AIDS, are at increased risk of melanoma.3–5 Whether, and to what degree, patients with rheumatoid arthritis (RA) are also at increased risk is less clear. Conflicting results were reported in patients with biologic-naïve RA.6–10 With the introduction of biologic therapies and in particular tumour necrosis factor inhibitors (TNFi) to the treatment of RA and other diseases, concerns were raised that these therapies may increase the risk of malignancy and in particular melanoma.5 ,11 ,12 TNF may play a protective role in the growth or recurrence risk of melanoma13 ,14 and high dose, locally administered TNF has been shown to have a powerful antineoplastic effect against melanoma.15 No overall increased risk of solid tumours has been observed in a large Swedish population-based study, a later meta-analyses of RCTs, and in other observational cohort studies.11 ,12 ,16–19 Conversely, both meta-analysis of randomised controlled trials and observational cohort studies have raised concerns regarding an increased risk of melanoma and non-melanoma skin cancer in patients who had RA treated with TNFi,5 ,11 ,12 ,20 ,21 supporting the hypothesis of a causal pathway from TNF inhibition to developing melanoma.
Because of these concerns, representatives from 11 European biologic registers undertook a collaborative project to investigate the risk of developing invasive melanoma in patients who had RA treated with conventional synthetic or biologic disease modifying antirheumatic drugs (DMARDs) under the auspices of the European League Against Rheumatism (EULAR) Registers and Observational Drug Studies (RODS) Study Group. The aim of this study was to conduct a collaborative project across several European countries to compare rates of invasive melanoma in different treatment groups of patients with RA to those in the general population.
Patients and methods
Study design
The study population was assembled by a working group of representatives from European biologic registers within the EULAR RODS Study Group. The working group met three times in 2013 and 2014, discussed objectives of the project, data ascertainment methods, proposals for a coordinated analysis, agreed-upon the statistical analysis plan and finally discussed first results and possible limitations of the findings. The following registers participated in this project: French biologic register ‘autoimmunity and rituximab’ (AIR),22 Swedish biologics register (ARTIS),23 Czech biologics register (ATTRA), British Society for Rheumatology Biologics Register for Rheumatoid Arthritis (BSRBR-RA),24 Danish Rheumatologic database (DANBIO),25 Italian biologic register (GISEA), French biologic register ‘Orencia and RA’,22 German biologics register ‘Rheumatoid arthritis observation of biologic therapy’ (RABBIT),17 French REGistry—RoAcTEmra,22 Portuguese RA register (Reuma.pt) and Swiss Clinical Quality Management Database. Registries were required to have at least one melanoma reported among patients with RA in order to participate. Each registry study was given approval by their local Data Protection Agency/ethics committee according to local regulations.
Patients
Patients were required to have RA and be prospectively followed-up in one participating European biologic register. Patients with a history of invasive melanoma prior to registration were excluded to prevent the inclusion of recurrent lesions. Patients with prior melanoma in situ were permitted to enter the analysis due to difficulties in identifying such patients accurately and misclassification between melanoma in situ and benign lesions. Cohorts of biologic-naïve patients and patients treated with TNFi, rituximab (RTX), tocilizumab (TOC) and abatacept (ABT) were assembled. Based on previous findings5 which did not observe an association between melanoma occurrence and exposure time to TNFi we did not differentiate between cohorts with shorter or longer mean length of follow-up/shorter or longer exposure times to TNFi or other biologic and non-biologic DMARDs.
One exposure definition was used for the biologic-naïve cohorts: patients had to be biologic-naïve at the time of first registration and at follow-up. Exposure time started at first registration and was censored either at the date of invasive melanoma, death, end of follow-up or the date of receiving a first biologic drug, whichever came first.
Three exposure definitions were applied in the anti-TNF cohorts: prior exposure to biologic drugs (other than anakinra) was not permitted in any of the corresponding anti-TNF cohorts. An ‘ever-exposed’ approach was used in the primary analysis. Patients were at risk and contributed follow-up time to the anti-TNF cohort from the first dose of an anti-TNF drug after registration until invasive melanoma, death or end of follow-up (no later than 30 April 2014). In a second ‘most recent drug’ approach, a switch to a non-anti-TNF drug also led to a censoring of the subsequent observation time. In a third on-drug approach the observation time was censored 3 months after treatment termination, invasive melanoma, death or end of follow-up (no later than 30 April 2014), whichever came first.
In the case of the RTX, TOC and ABT cohorts, the same three exposure definitions were applied. In the third approach patients were considered on RTX treatment 9 months after the last dose. Prior exposure to TNFi was allowed for non-anti-TNF biologics, reflecting real-world practice during the period of data collection.
In registries where a drug cohort had fewer than 1000 person-years (pyrs) of follow-up accumulated this subcohort was excluded from the analysis, since these subcohorts very likely contribute only to the denominator (pyrs) but not to the numerator (number of events) of the incidence rates. In the case of the BSRBR-RA TOC cohort, this exclusion led, however, also to the exclusion of one melanoma case. Nevertheless, the exclusion had no influence on the significance of the TOC results.
Outcome
The outcome was first invasive melanoma (cutaneous or metastatic). Three registries received reports of melanoma through linkage of all participants to their national cancer registry: DANBIO (Denmark), ARTIS (Sweden) and BSRBR-RA (UK). The remaining registries (as well as the UK) received reports of melanoma from the patient's rheumatologist. These melanomas were required to be confirmed by histology report.
Statistical analyses
The incidence of melanoma in the general populations of the participating countries varied considerably (table 1). To deal with these differences and the increasing melanoma incidences over time (see ref. 2), melanoma incidence rates were first compared with age-matched and sex-matched incidences in the general population of the corresponding country and calendar year. For that reason the observation time of each cohort within one calendar year was stratified by sex and 5 years age bands and then the expected number of melanomas within that cohort in the specific calendar year was calculated based on the age-stratified and sex-stratified population data of the corresponding register in the corresponding calendar year. Standardised incidence ratios (SIRs) were then calculated by dividing the sum of observed melanoma by the sum of expected melanomas.
Means of age-standardised incidence rates of melanoma (years 2003–2012) using the European standard population aged 40–84 as reference
Therefore, the calculation of SIRs took account of temporal changes in the melanoma incidence in the general populations over the course of data collection for this study (see ref. 2). Poisson regression models were used to summarise the register-specific SIRs to overall SIR estimates as weighted sums of individual SIRs such that the weights were higher for cohorts with higher numbers of events.
SIRs of melanoma in biologic-exposed patients were compared with those in biologic-naïve patients within countries by calculating incidence rate ratios (IRRs). Overall IRRs were calculated, again weighting according to the number of events in the registers. To explore whether or not the variation in the SIRs can be completely explained by random variation due to low numbers of events, the Marshall and DerSimonian Laird methods to estimate the systematic heterogeneity in the SIRs were applied.26 Generally speaking heterogeneity is measured by the observed variability in the SIRs minus the expected variability due to low event numbers. In the case of zero (no) heterogeneity the result of this difference might be negative, it will then be reported to be zero. Since the two methods agreed only one result is reported.26
Furthermore, in sensitivity analyses SIRs and IRRs were also calculated for females and males separately as well as for patients aged 55–74, because in a previous analysis from ARTIS the risk of melanoma in patients exposed to TNFi was noted to be higher in men and those aged 55–74.5 To explore a possible under-reporting of rheumatologists, SIRs and IRRs observed in registers with record linkage to cancer registries were compared with the corresponding SIR or IRR estimates in the remaining registers by means of Poisson regression. To compare incidence rates in the general population, country and calendar year-specific incidence rates of melanoma in the general populations were standardised by using the European standard population (WHO 1990) aged 40–84 as reference.
Results
Overall 130 315 patients from 11 registers contributing 579 983 pyrs were included. The mean age at the time of first registration ranged between 50 (ATTRA TNFi cohort) and 62 (ARTIS) (table 2) years. Similar large variations were observed for the portion of female patients ranging between 65% (GISEA TNF cohort) and 87% (Reuma.pt TNFi cohort) and the median disease duration of RA, which was lowest in the biologic-naïve DANBIO cohort (3.9 years) and highest in RTX-treated patients in AIR (17 years).
Baseline characteristics of biologic-naïve, TNFi rituximab, tocilizumab or abatacept ever-exposed RA patients
Comparisons to the general populations by means of SIRs
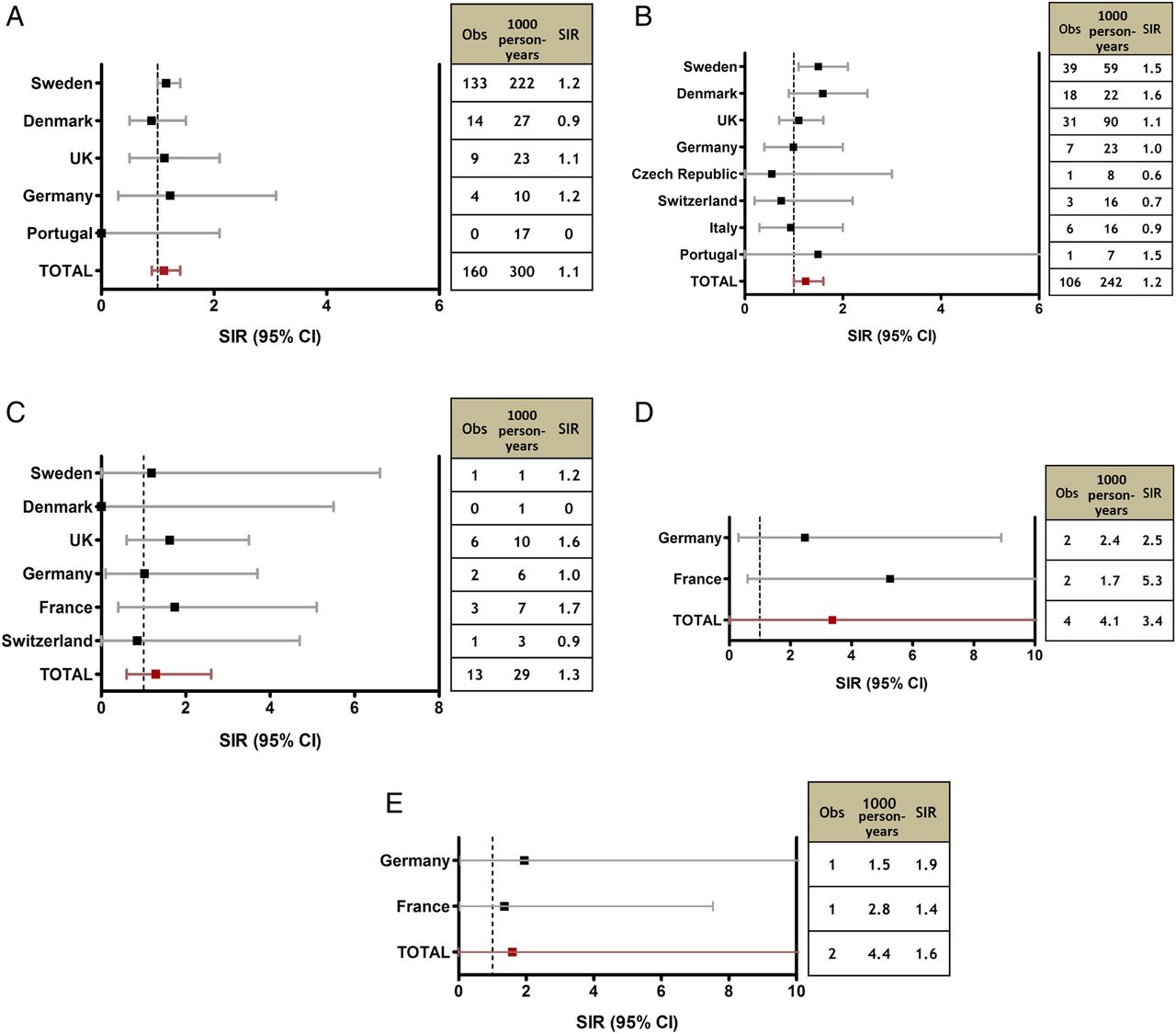
In total 287 patients developed a first melanoma. Overall 160 melanomas were reported in biologic-naïve patients with RA from five countries (figure 1A). Using country and calendar year-specific melanoma rates in the general populations of the corresponding biologic registers as reference only minor variations in the SIRs across registries and a minor non-significant increase in the overall SIR: 1.1 (95% CI 0.9 to 1.4) were observed. A total of 106 patients developed a first melanoma in patients ever exposed to TNFi. A larger variation was observed in the SIR in TNFi-exposed patients between registries (figure 1B). Furthermore, the overall SIR observed in registers with data linkage to cancer registries (Sweden, Denmark, UK) was numerically higher 1.3 (0.85 to 2.1) but did not achieve statistical significance. In general, the observed variation was attributable to random variation because of low numbers of cases of melanoma within individual registers. The portion of the variation attributable to systematic heterogeneity was estimated to be 0%. After combining the country-specific results to an overall SIR a small increase in the melanoma incidence of TNFi ever exposed patients was observed (SIR 1.2 (0.99 to 1.6), p=0.062). The most recent drug use approach resulted in a similar finding. Ninety-three melanomas in 220 259 pyrs of TNF-exposed patients corresponded to an SIR of 1.2 (0.9 to 1.6). Using the on-drug approach 77 melanomas were observed in 188 051 pyrs of TNF-exposed patients (SIR 1.2 (0.8 to 1.8)).

Standardised incidence ratios (SIRs) of melanoma in: (A) biologic-naïve, (B) tumour necrosis factor inhibitors (TNFi) ever exposed, (C) rituximab ever exposed, (D) tocilizumab ever exposed and (E) abatacept ever exposed patients with RA. obs, Observed melanoma.
No significantly increased melanoma incidence and no heterogeneity between the register-specific results were observed in patients ever (13 melanoma in 28 707 pyrs, SIR 1.3 (0.6 to 2.6)) or most recently (11 melanoma in 23 248 pyrs, SIR 1.4 (0.6 to 3.2)) exposed to RTX (figure 1C). Limited data were available for TOC and ABT-treated patients. For that reason very wide 95% CIs of the SIR estimates were calculated for TOC ever (four melanoma in 4053 pyrs, SIR 3.4 (0.0 to 1930), p=0.25) or ABT ever (two melanoma in 4399 pyrs, SIR 1.6 (0 to 12 704), p=0.63) exposed patients.
Comparisons between biologic-naïve patients and TNFi, RTX, TOC or ABT-exposed patients
The comparison of the SIRs of biologic-exposed patients with the SIRs of biologic-naïve patients resulted in slightly but non-significantly increased IRRs for TNFi and RTX-exposed patients (figure 2A, B). The IRR global of TNFi ever exposed patients was 1.14 (0.8 to 1.6). In registers with data linkage to cancer registries (Sweden, Denmark, UK) the IRR of TNFi ever exposed patients was slightly higher (IRR: 1.2 (0.8 to 1.7)) but did not differ significantly from those observed in registers which relied solely on physician reporting of melanomas (IRR=1.1, p=0.28). SIRs of TOC and ABT-treated patients also did not differ significantly from the SIRs in biologic-naïve patients.

Melanoma incidence rate ratios (IRRs) of (A) tumour necrosis factor inhibitors (TNFi) ever exposed and (B) rituximab ever exposed patients compared with biologic-naïve patients.
Sensitivity analyses
Sensitivity analyses performed separately in males and females were similar to previous findings in the Swedish register with lower IRRs of TNFi ever exposed females (IRR 0.9 (0.4 to 1.9) vs IRR males: 1.6 (0.6 to 4.4)). However, none of these IRRs differed significantly from 1. The SIR of Swedish TNFi patients aged 50–74 at time of melanoma diagnosis was numerically higher than the corresponding SIR of Swedish biologic-naïve patients (figure 3). Across the three registers with sufficient data in these subcohorts there was no significant difference between both treatment exposure groups (IRR=1.39 (0.6 to 3.3)).

{kind=link}
{kind=link}
{kind=link}
Subgroup analysis: standardised incidence ratios (SIRs) of melanomas in patients aged 50–74 years at the time of melanoma diagnosis. TNF, tumour necrosis factor.
Discussion
In all treatment groups the incidence of invasive melanoma was slightly higher in RA than in the corresponding general populations of the participating countries. Nevertheless, even with this large European collaborative project of 11 registers from nine countries the previous signal of an increased risk of melanoma following TNFi reported by ARTIS5 and DANBIO12 was not replicated across the other registries in this study. We did not detect a significant overall increase in the age and sex standardised incidence ratios. No significant differences in the melanoma incidence were observed between biologic-naïve patients and patients exposed to TNFi, RTX, ABT or TOC. Sensitivity analyses of subcohorts of TNFi-exposed patients confirmed these findings, whereas limited sample sizes require a cautious interpretation of the findings for patients treated with ABT and TOC.
We were furthermore not able to confirm a previous finding of an increased melanoma risk in RA males or RA patients aged 50–74 who were treated with TNFi.5
It is a notable achievement that we were able to bring together investigators from multiple national biologics registers in order to undertake this collaborative analysis. Despite the power of individual national registers, there remain safety concerns of clinical importance that individual registers are unable to address with confidence. Here, we were able to collate over half a million person-years of monitoring across Europe. Similar to others we assumed that treatment decisions were made independently of skin type and patients' behaviour to deal with exposure to ultra violet radiation. The application of rather strict case validation methods and the consideration of different exposure models contributed to the strengths of this study. Nevertheless, the validity of our findings depends on the validity of the data of each subcohort. The impact of biases or residual confounding in individual datasets on the summary results cannot be estimated or controlled for. We presumed that dropouts and especially measures to detect melanoma early in an in situ stage had no different impact on the results in biologic-naïve or bDMARD-treated patients. Furthermore, the SIR for melanoma risk in TNFi-treated patients was numerically higher, although not statistically different, when limited to countries with linkage to cancer registries (Denmark, Sweden, UK). This raises the possibility that ascertainment of melanoma cases was incomplete in other registries. Considering these limitations we cannot completely rule out an increased melanoma risk in patients with RA treated with TNFi. Nonetheless, the findings of the different registers were rather consistent. We detected no systematic heterogeneity between the country-specific SIRs. For these reasons we conclude that this large European collaborative project did not confirm an overall increased risk of melanoma following exposure to TNFi.
Acknowledgments
We thank Adele Green (Paterson Institute for Cancer Research, The University of Manchester), Lene Mellemkjær (Danish Cancer Society Research Center, Copenhagen), Florence Tubach (Département d'Epidémiologie et Recherche Clinique, Université Paris Diderot, Paris), Piet van Riel (Department of Rheumatic Diseases, Radboud University Nijmegen Medical Centre), Victoria Hernández (Research Unit, Sociedad Española de Reumatología, Madrid, Spain), for valuable discussions regarding this project. We also thank Hanna Dyck (German Rheumatism Research Centre) for her support in the statistical analysis of the data.
References
Supplementary materials
Lay summary
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Tore K Kvien
Twitter Follow William Dixon at @WGDixon
Contributors Study concept and design: LKM and JL. Acquisition of the data and critical revision of the manuscript for important intellectual content: LKM, JA, PR, WGD, LD, MLH, AS, AZ, XM, AF, HC, FI, JZ, JM, J-EG, KLH and JL. Drafting the manuscript: LKM and JL.
Funding Individual registries were funded by pharmaceutical companies (AbbVie, BMS, MSD, Pfizer, Roche, UCB). The pharmaceutical companies funding these registers were, however, not involved in the planning of the project, the statistical analyses or the interpretation of the results.
Competing interests JA received grant/research support from AstraZeneca, Merck, Lilly and Pfizer, and has received grant support from Abbvie, Pfizer, Merck, Roche, BMS and UCB for the ARTIS register. LD has received speaking fees from UCB and MSD. AS received speakers fees (<$10 000) from BMS, MSD, Pfizer, Roche, Sanofi-Aventis. AZ received grant/research support from Abbvie, Amgen, BMS, MSD, Roche, Pfizer and UCB for the German biologics register RABBIT and speakers fees (<$10 000) from BMS, MSD, Novartis, Pfizer, Roche, Sanofi and UCB. XM received honorarium (<$10 000) from BMS, Pfizer and UCB. AF received honorarium (<$10 000) from Abbvie, BMS, Pfizer, Roche and UCB. FI received personal fees from Actelion, Celgene, Janssen, Pfizer, AbbVie, UCB and MSD outside the submitted work. JZ received honorarium (<$10 000) from Abbvie and Hospira. JM received <$10 000 for honoraria and consultancies from Roche. J-EG received honorarium (<$10 000) from Abbvie, BMS, MSD, Pfizer, Roche and UCB. KLH received grant/research support from Pfizer and honoraria (<$10 000) from Abbvie and Pfizer. JL received honoraria (<$10 000) from Novartis-Sandoz and Pfizer.
Patient consent Obtained.
Ethics approval Each register was given approval by their local ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.