Article Text

Abstract
Objective Current research in rheumatoid arthritis focuses on preclinical disease phases as it is hypothesised that early preclinical treatment might prevent progression to full-blown disease. Since performance of studies in prearthritis phases in humans is challenging, animal models offer an opportunity to evaluate preventive treatments. We performed a systematic literature review and summarised treatment effects during different stages of arthritis development in animal models.
Methods Eight medical literature databases were systematically searched. Studies were selected if they reported effects of synthetic or biological disease-modifying antirheumatic drugs in animal models of arthritis (collagen-induced arthritis and adjuvant-induced arthritis) on arthritis severity, as measured with arthritis severity scores, paw swelling or paw volume. Quality was assessed using an 11-item checklist. Study characteristics were extracted and effect sizes obtained in high-quality studies were summarised in meta-analyses. Studies were categorised into three groups: prophylactic (prior to generation of autoantibody response), prearthritis (after induction of autoantibody response) and therapeutic intervention (after arthritis development).
Results Out of 1415 screened articles, 22 studies (including n=712 animals) were eligible of good quality and included in meta-analyses. Prophylactic (16 experiments, n=312 animals) and prearthritis treatment (9 experiments, n=156 animals) both were associated with a reduction of arthritis severity (p<0.001 and p=0.005, respectively). Stratified analyses for different antirheumatic drugs initiated in the prearthritis phase suggested higher efficacy of methotrexate than of anti-tumour necrosis factor.
Conclusions Data of experimental studies in animal models of arthritis suggest that prophylactic and prearthritis treatment strategies are effective and hint at differences in efficacy between antirheumatic drugs.
- Rheumatoid Arthritis
- Arthritis
- Autoantibodies
- Autoimmunity
Statistics from Altmetric.com
Introduction
During recent years, research in the field of rheumatoid arthritis (RA) has focused on the earliest stages of the disease. This has provided novel insights into the immunological processes that precede the transition from healthy to established disease. Currently, the field of RA is moving from disease suppressive treatments to prevention strategies, focusing on initiation of treatment in prearthritis phases. Within RA, it has been shown that a prolonged symptom duration at treatment start is associated with a worse disease outcome, including a lower chance on achieving disease-modifying antirheumatic drug (DMARD)-free sustained remission.1–4 Therefore, it is hypothesised that treatment initiation during prearthritis stages might result in an improved efficacy in preventing disease chronicity.5 Within type I diabetes, preventive trials have shown efficacy of very early intervention to prevent full-blown disease.6–8
To evaluate whether very early treatment initiation can also prevent the development of RA, several placebo-controlled randomised-controlled clinical trials have been initiated recently. These clinical trial studies are all pre-results and will investigate the therapeutic potential of several immunomodulatory agents such as rituximab (PRAIRI study: NTR no. 1969), abatacept (APIPPRA study: ISRCTN no. 46017566 and ARIAA study: EudraCT no. 2014-000555-93), hydroxychloroquine (StopRA trial; NCT no. 02603146) and methotrexate (TREAT EARLIER; NTR no. 4853) in individuals at a risk of RA. A study evaluating the immunomodulatory effect of atorvastatin in patients with seropositive arthralgia has also been initiated (STAPRA study: NTR no. 22389). Interestingly, design of these trials does not follow the normal development of phase I, II and subsequently phase III trials. Moreover, dosages used are from other indications targeting different biology and the length of treatment is relatively randomly defined. The performance of randomised clinical trials on preventative treatment strategies in individuals at risk for RA is therefore difficult to interpret. Early identification and recruitment of patients at risk for RA is difficult, and execution of these studies is time consuming. Altogether, it will take several years before the majority of these currently ongoing clinical trials are completed and the results are known. Likewise, because of difference in study design and patient selection, it will be difficult to compare side by side which intervention will be most effective in reaching sustained symptom-free and drug-free benefit.
Animal models of arthritis can function as innovative tools to study the potential of preventive therapies. Animal studies provide an opportunity to study the developing (auto)immune response at a very early disease phase and the translation of different stages of experimental arthritis development to the evolution of human disease might provide valuable information regarding possibilities of disease prevention. Murine models of arthritis are scientifically well defined, highly reproducible, genetic identical, represent different disease pathways relevant for RA and are readily available. While current animal research mainly focuses on testing antirheumatic drugs in established disease, it is unknown whether preventive treatment in mouse models is also effective. In addition, it is unknown if the efficacy of prophylactic or prearthritis intervention depends on the type of antirheumatic drug used. These questions prompted us to perform a systematic literature review and summarise the knowledge on the efficacy of treatment initiated before arthritis was clinically evident. Our first aim was to evaluate whether prophylactic or prearthritis treatment is effective in animal models of arthritis. The second aim was to evaluate the efficacy of different synthetic and biological DMARD treatments initiated in prearthritis phases.
We focused on two widely accepted experimental models for RA; collagen-induced arthritis (CIA) and adjuvant-induced arthritis (AIA), both models are based on immunisation-induced arthritis. In the CIA model, arthritis is induced by immunisations with cartilage proteins causing a break of tolerance and an immune-mediated inflammatory attack on the joints.9 ,10 Animals receive type II collagen emulsified in complete Freund's adjuvant typically followed by a second injection three weeks later, leading to the development of chronic destructive arthritis. There are three developmental stages of arthritis in the CIA model; an induction phase, a prearthritis phase where autoimmunity is present in the absence of clinical symptoms and established arthritis.11 The AIA model requires intradermal immunisation with mycobacterial cell wall components suspended in mineral oil causing an acute and systemic inflammation. The development of arthritis in the AIA model is thought to depend on a heat shock protein-specific T cell response. In contrast to CIA, AIA is self-limiting and contains three developmental stages of arthritis; incubation phase, prearthritis phase and a peak phase followed by a gradual regression of inflammation.12 Thus, these experimental models of arthritis have clearly defined developmental stages that can be identified by immunological disease markers. According to these developmental stages of arthritis, we discerned three types of treatment: prophylactic (prior to generation of autoantibodies), prearthritis (after induction of an autoantibody response) and therapeutic intervention (after arthritis development) (see figure 1). We performed a systematic literature review and summarised the effects of treatment initiated at these stages.

Schematic representation of developmental stages of collagen-induced arthritis (CIA) and human rheumatoid arthritis (RA). Type of intervention during different developmental stages of experimental arthritis in the CIA model. Arthritis is generally induced by immunisation with CII emulsified in complete Freund's adjuvant followed a booster injection three weeks later of CII in incomplete Freund's adjuvant. After immunisation with type II collagen, during the initiation phase, autoimmunity towards collagen will develop (blue circles). Drug intervention during this time period is referred to as prophylactic treatment. This first stage is followed by a prearthritis phase, which is characterised by the onset of autoimmunity and is marked by the development of autoantibodies against type II collagen that occurs around day 10. The time period in which autoimmunity is present and arthritis is still absent is referred to as the prearthritis period. Intervention during this prearthritis disease stage is described as prearthritis treatment. The time period of prearthritis is followed by the onset of arthritis (red triangles), which occurs around day 20 and leads to chronic destructive arthritis. Drug intervention at the established arthritis stage is described as therapeutic intervention (A). Schematic representation of human RA development. Genetic and environmental factors drive the onset of autoimmunity, which subsequently leads to undifferentiated arthritis and finally full-blown disease (B).
Methods
Search strategy
Eight bibliographic databases (PubMed, Medline, Embase, Web of Science, Cochrane Library, CINAHL, Academic Search Premier and Science Direct) were searched to identify studies investigating treatment strategies in animal models for experimental arthritis (search conducted on 14 April 2016). A systematic search strategy was developed for PubMed (see online supplementary file 1) and was subsequently applied in all other databases. Search terms were rheumatoid arthritis, experimental models for arthritis, therapeutic intervention DMARDs (Methotrexate, Leflunomide, Cyclosporine, Sulfasalazine, Azathioprine or Hydroxychloroquine, Prednisolone) or biologicals (anti-TNF, Anti-IL-1, CTLA4-Ig, anti-IL-6 or anti-CD20) combined with the Boolean operators AND/OR.
supplementary data
Inclusion and exclusion criteria
The inclusion criteria are described in online supplementary table S2. In short, we included published peer-reviewed studies reporting the effect of therapeutic intervention (synthetic or biological DMARDs) in the most commonly used in vivo models of experimental arthritis (CIA and AIA). Furthermore, experiments should be prospectively controlled and information on clinical outcome and joint structural changes should be provided. Abstracts were assessed based on type of research (animal studies), drugs tested, outcome measures (arthritis severity) and duplicates. Full papers were assessed to identify experimental arthritis models, study design, treatment and control groups, therapeutic interventions and outcomes measurements used in the studies.
Outcome measurements
Furthermore, studies were only selected if the following clinical outcomes were evaluated: arthritis severity scores (ordinal scale), paw swelling (mm) or paw volume (mL), or outcome measurements for joint structural changes by quantitative histological or radiographic scores measured with X-ray or microCT. An overview of the outcome measurements is presented in online supplementary table S3.
Data extraction
We extracted individual study characteristics from each publication, and, where a publication reported more than one experiment, these data were also extracted and considered independent experiments. Extracted data included experimental arthritis model, species, number of animals per group, drug and dose, route and time of drug administration, clinical, histological or radiological scores. Where arthritis severity measurements were performed serially, we only extracted the final time point.
Quality assessment of methodology
Study quality and risk of selection and detection bias was assessed by a modified 11-point-item checklist, adapted from the Collaborative Approach to Meta-Analysis and Review of Animal Data from Experimental studies.13 The checklist comprises items of study methodology: randomisation (1); allocation concealment (2); blinding (3); evidence of induced arthritis (macroscopic, histological or radiological) (4), sample size/power calculations (5), statement of conflict of interest (6), statement of compliance with animal welfare regulations (7), standardised method for data collection (8), (semi)quantitative scoring method for disease activity (9), (semi)quantitative scoring method for joint damage (10) and clear data presentation (11). Each item was scored as 1 if the data were reported satisfactorily and 0 if not (unclear risk of bias) and maximum score was 11. The median quality score of 6 was considered to be sufficiently high quality for further analysis. An overview of the checklist is depicted in online supplementary file S4.
Categorisation of studies according to type of intervention
Studies were discerned into three groups according to the time point of treatment initiation: (1) prophylactic treatment (days 0–9): therapy is initiated prior to injection of arthritis stimulators or after injection of arthritis stimulator but prior to the development of a systemic autoimmune response, which is characterised by production of autoantibodies. (2) Prearthritis treatment (days 10–20): start of therapy after the development of autoimmunity but before the onset of clinically evident arthritis. (3) Therapeutic treatment (>20 days): initiation of treatment after the onset of arthritis, which occurs generally around days 21–22.
Meta-analysis
Only studies with high methodological quality (score≥6) were summarised in meta-analyses. Furthermore, studies that did not provide SDs or SEM were excluded for the meta-analyses. To compare the severity of arthritis in the treatment group to an arthritic untreated control animal, we calculated the normalised mean difference (NMD) of arthritis clinical score, paw volume or paw swelling. The NMD effect size in the treated animals is calculated as a proportion of the mean in the control group.14 Similarly, we calculated the NMD for each experimental comparison as the proportional improvement in the treated group compared with the control group, along with the SE of the estimate. To account for anticipated heterogeneity, we applied the DerSimonian and Laird random-effects model15 to calculate an overall treatment effect, this random-effects model for meta-analysis uses both within-study variance and the between-study variance. We used Cochran's Q to calculate heterogeneity of the studies.16
Results
Study selection and study quality
Our systematic search identified a total of 3486 titles from eight databases (figure 2); 35 studies met the inclusion criteria based on full paper assessment. A summary overview of these 35 studies is presented in table 1; for the complete overview, see online supplementary table S5. For further selection of studies for meta-analysis, 28 studies were considered to be of sufficient high methodological quality (score≥6). Six of these studies did not report SDs or SEMs and therefore could not be included in the meta-analyses.17–22 Finally, the results of 22 studies, using a total of 712 animals (control animals, n=263 and treated animals, n=449), were summarised in meta-analyses. The most frequently used model of experimental arthritis was the CIA model (CIA 16 studies, AIA 8 studies). In total, 16 studies used rats and 6 studies used mice (supplementary table 3). Also, 13 out of 22 publications (59%) reported the blinded assessment of outcome, 15 (68%) reported randomisation and none reported performing a sample size calculation (online supplementary table S6). The outcome summarised in the meta-analysis was the proportion of reduction of arthritis severity (expressed in NMD).
List of all 35 studies that met the inclusion criteria based on full paper assessment
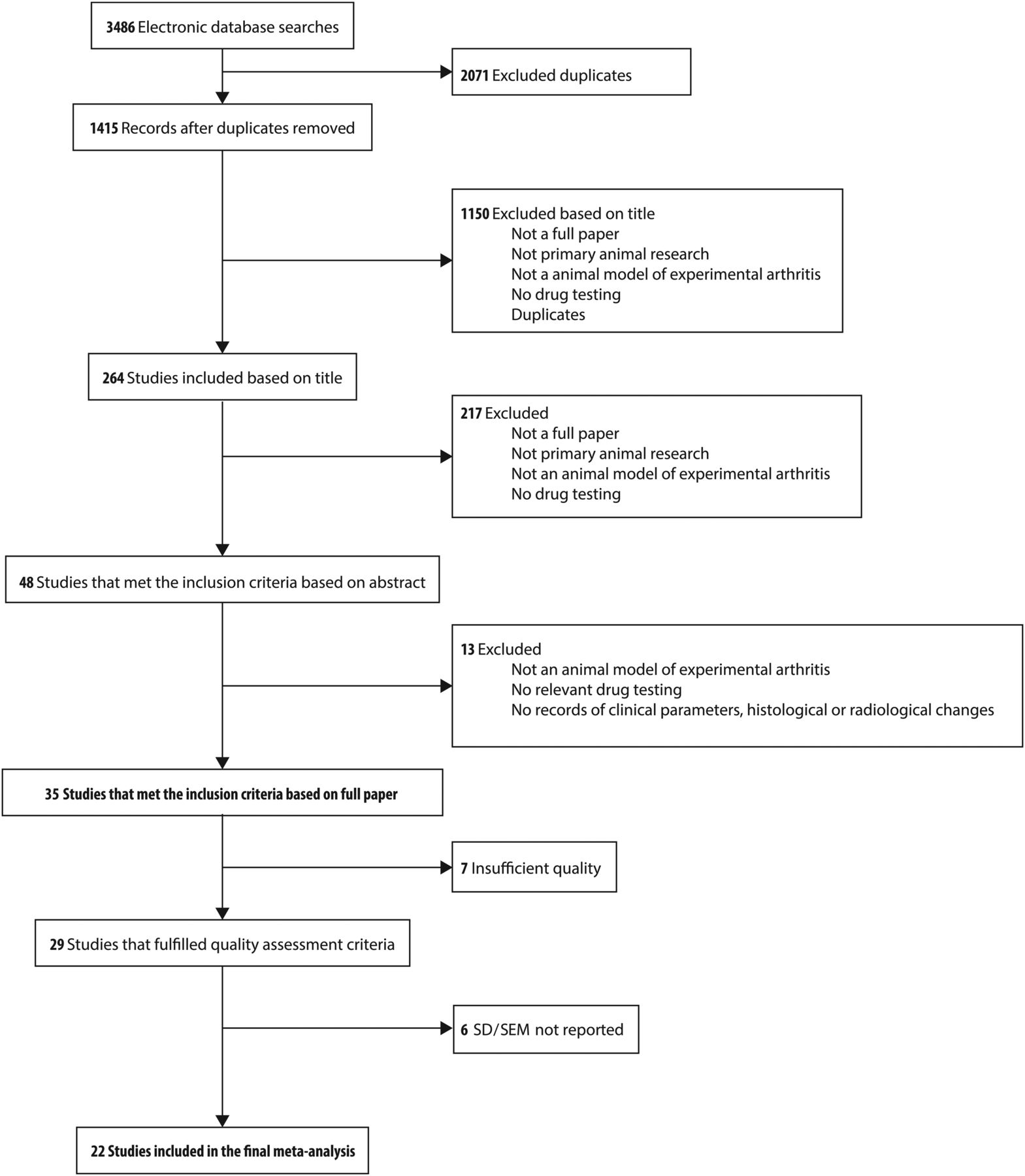
Flow diagram of study selection.
Histological and radiographic scores were not consistently scored in uniform scoring scales. Therefore, it was impossible to perform meta-analyses on these outcomes.
Effect of intervention on clinical outcome
The treatment efficacy on arthritis severity was studied per disease stage.
Prophylactic treatment
Sixteen experiments (including 312 animals) studied the effect of prophylactic intervention on the severity of arthritis (figure 3A). Several DMARDs were tested in a prophylactic setting (methotrexate (six experiments),23–27 leflunomide (one experiment),28 ciclosporin A (two experiments),26 ,27 azathioprine (one experiment),27 hydroxychloroquine (one experiment)27 and methylprednisolone/dexamethasone (two experiments),27 ,29 anti-IL1 (one experiment)29 and CTLA4-Ig (two experiments)).30 ,31 The combined effect size of the different studies indicated that prophylactic intervention is associated with a reduction of arthritis severity in animal models of arthritis (p<0.001). Prophylactic treatment with both methotrexate (p<0.001) and CTLA4-Ig (p<0.001) was significantly associated with a reduction in arthritis severity (figure 3B).
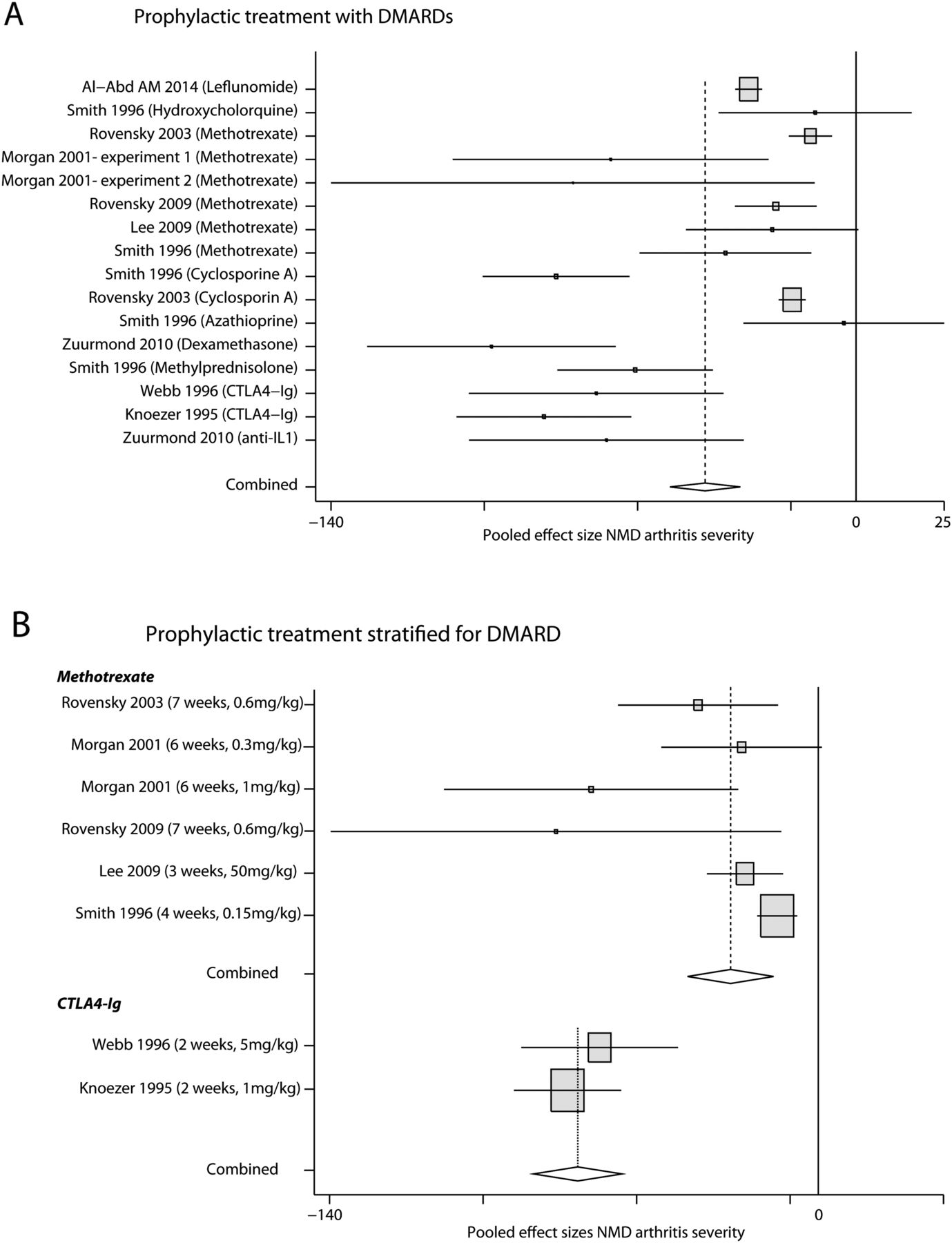
Prophylactic intervention in experimental models of arthritis. Effect of prophylactic intervention on arthritis severity reported in 16 individual experiments using synthetic or biological disease-modifying antirheumatic drugs (DMARDs). The pooled effect size of normalised mean difference (NMD) in arthritis severity is −40.1 (95% CI −50.6 to −31.4, z-value=−8.2, p<0.001) (A). Stratified meta-analysis of the different experiments investigating the effects of different antirheumatic drugs further specified for methotrexate, pooled estimate −26.0 (95% CI −38.6 to −13.5, p<0.001) and CTLA4-Ig, pooled estimate −80.2 (95% CI −100.0 to −60.7, p<0.001). Treatment length was on average 5.5 weeks for methotrexate and 2 weeks for CTLA4-Ig (B). IL, interleukin.
Prearthritis treatment
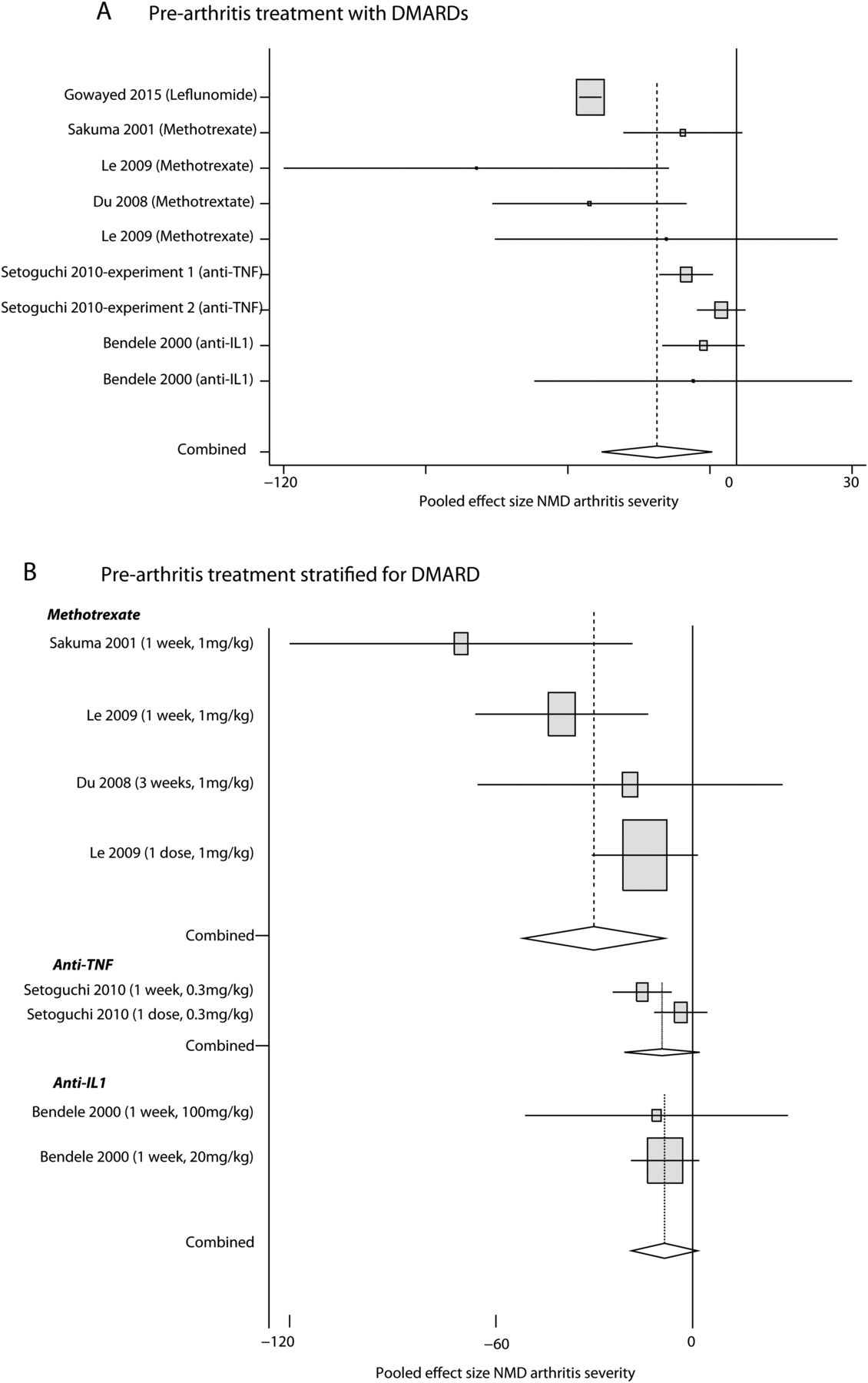
Nine experiments (including 156 animals) studied the effect of early prearthritis treatment on arthritis severity (figure 4A). DMARDs tested were leflunomide (one experiment),32 methotrexate (four experiments),33–35 anti-tumour necrosis factor (TNF) (two experiments)36 and anti-interleukin (IL)1 (two experiments).37 A meta-analysis of these studies demonstrated that prearthritis intervention is associated with a reduction of arthritis severity in animal models of arthritis (p=0.005). Stratified analysis for most commonly used DMARDs revealed that treatment with methotrexate was significantly associated with less arthritis severity (p<0.01), while no statistically significant results were obtained for anti-TNF (p=0.065) and anti-IL1 (p=0.098) (figure 4B). None of the animal studies performed in a prearthritis stage evaluated a reduction of arthritis incidence or a delay in arthritis onset after short-term treatment.
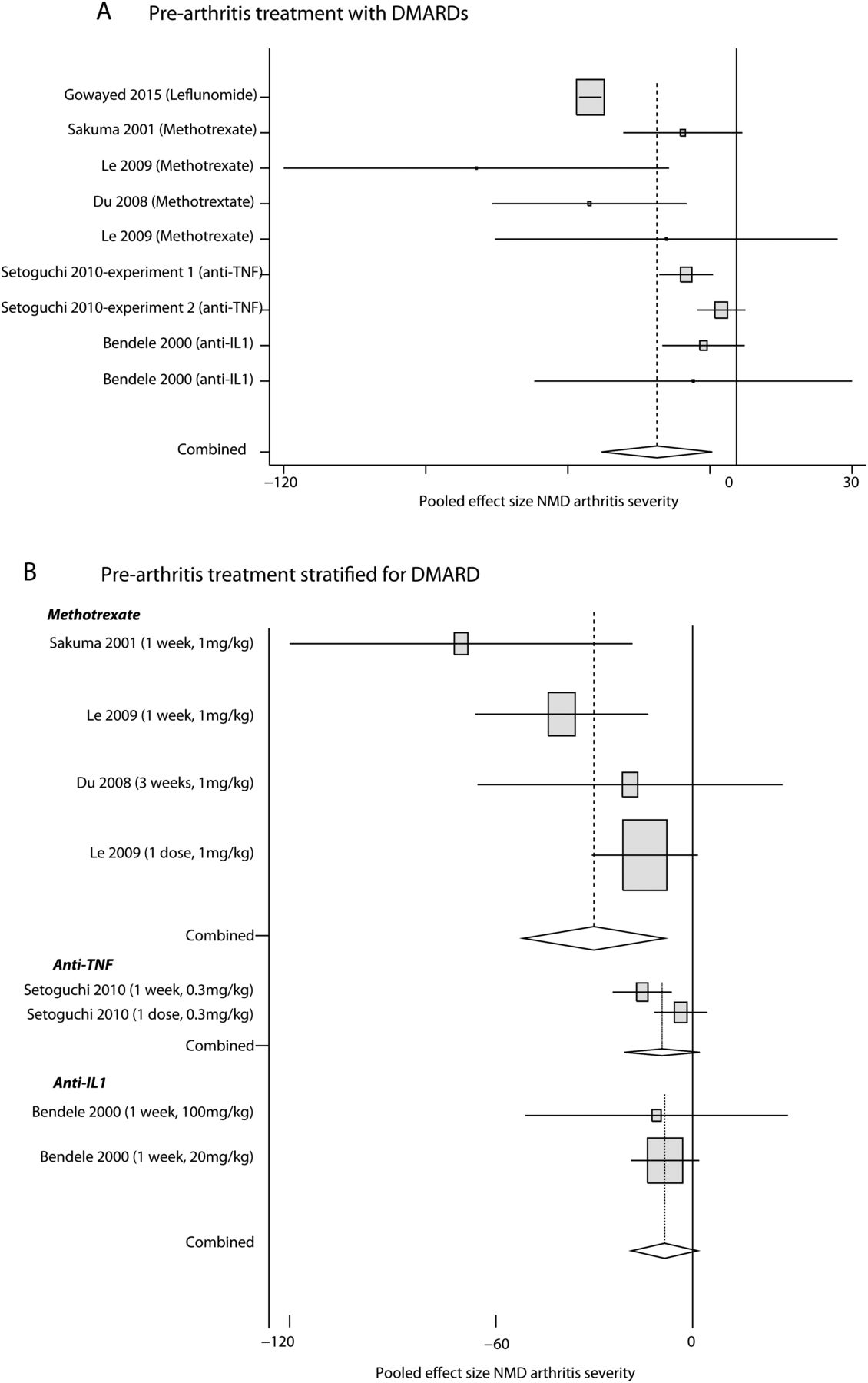
Prearthritis intervention in experimental models of arthritis. Effect of prearthritis intervention on arthritis severity reported in nine individual experiments using synthetic or biological disease-modifying antirheumatic drugs (DMARDs) in a prearthritis phase of arthritis. The pooled effect size of normalised mean difference (NMD) in arthritis severity is −21.2 (95% CI −35.9 to −6.5, z-value=−2.8, p=0.005) (A). Stratified meta-analysis of the different experiments investigating the effects of different antirheumatic drugs further specified for methotrexate pooled estimate −29.5 (95% CI −50.6 to −8.4, p=0.006), anti-tumour necrosis factor (TNF) pooled estimate –8.6 (95% CI −17.7 to 0.5, p=0.065), and anti-interleukin (IL)1 pooled estimate −9.0 (95% CI −19.6 to 1.6, p=0.098). Treatment length was on average 1 week for methotrexate, anti-TNF and anti-IL1 (B).
Therapeutic treatment
Twelve experiments (including 244 animals) studied the effect of therapeutic treatment in established arthritis (figure 5A). Antirheumatic drugs tested in established disease were sulfasalazine (one experiment),38 methotrexate (two experiments),39 ,40 anti-TNF (four experiments),39 ,41–43 anti-IL1 (three experiments)42 ,44 and CTLA4-Ig (two experiments).30 Therapeutic treatments with methotrexate (p<0.001), anti-TNF (p<0.001), anti-IL1 (p<0.001) and CTLA4-Ig (p<0.001) in established disease were all significantly associated with a reduced arthritis severity (figure 5B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Therapeutic intervention in experimental models of arthritis. Effect of therapeutic intervention on arthritis severity reported in 12 individual experiments using synthetic or biological disease-modifying antirheumatic drugs (DMARDs) in established arthritis. The pooled effect size of normalised mean difference (NMD) in arthritis severity is −44.2 (95% CI −54.4 to −34.0, z-value=−8.5, p<0.001) (A). Stratified meta-analysis of the different experiments investigating the effects of different antirheumatic drugs further specified for methotrexate −34.4 (95% CI −42.5 to −26.3, p<0.001), anti-tumour necrosis factor (TNF) −32.2 (95% CI −49.2 to −15.1, p<0.001), anti-interleukin (IL)1 −70.6 (95% CI −79.9 to −61.3, p<0.001) and CTLA4-Ig −27.9 (95% CI −34.3 to −21.5, p<0.001). Treatment length was on average 4 weeks for methotrexate, 3.3 weeks for anti-TNF, 1 week for anti-IL1 and 3 weeks for CTLA4-Ig (B).
Subanalyses
Since CIA and AIA somewhat differ in disease pathology, we have performed separate subanalyses for these models, which showed similar results as that of the total group (see online supplementary files S7 and S8).
Discussion
The present systematic literature review and the meta-analyses of data on treatment in animal models of experimental arthritis reveal that “prophylactic and prearthritis treatment strategies” are effective and result in less severe disease. Currently, research emphasises on early identification of individuals at risk for developing RA with as ultimate goal the reduction of disease severity or even to prevent clinically manifest disease. Although it will take years before the results of current clinical trials will be at the stage of publishing, results of the present study in animals support the concept that very early treatment may be effective.
Observational studies in patients with RA have provided evidence that supports the concept of a therapeutic ‘window of opportunity’. The period in which the disease is most susceptible to treatment is presumed to consist of the first three months after symptom onset.52 ,53 Although some studies have treated patients rapidly after arthritis has become clinically evident,54–57 studies that initiate treatment already in prearthritis phases are more challenging to perform because of the difficulty to identify patients with arthralgia and a high predicted risk for developing RA. Some of the preventive studies in human RA aim to target autoantibody-positive subjects with arthralgia, and we hypothesise that this phase corresponds to intervention in the prearthritis phase of the CIA model. But, although the CIA mouse model is widely used to mimic the antibody-dependent process of RA pathogenesis, anticollagen antibodies are not the most prominent antibodies in human RA and conflicting results on ACPA induction in CIA exist.58 Thus, while CIA and AIA are informative, these models only partially resemble the situation in human RA and reflect only some of the basic disease mechanisms and molecular pathways involved in RA development. Despite the disparities between animal models of arthritis and RA, animal models of arthritis are of interest, and the summarised data suggest that very early treatment is effective.
The second aim was to evaluate the effect of different medications in animal models. The most frequently studied DMARDs were methotrexate and anti-TNF. In humans, several other drugs (abatacept, hydroxychloroquine, atorvastatin) are now also being investigated in prearthritis phases. Studies investigating the effect of hydroxychloroquine on animal models are limited; in our meta-analysis, we included only one study that evaluated hydroxychloroquine on CIA. Our literature search was limited to studies that tested DMARDs; statins were not included. Nevertheless, the effects of statins have been studied, with contrasting results; some studies reported anti-inflammatory effects44 ,45 while others pointed to an accelerated onset of CIA in mice.46 In our meta-analysis, we observed a higher effect for methotrexate than for anti-TNF, which may suggest that methotrexate is more disease-modifying in this very early disease phase. Though, formal conclusions on the difference in efficacy or treatment dose cannot be made and translation to the human setting is limited. None of the prearthritis studies compared the different medications head to head.
We distinguished treatment started in the initiation phase (prophylactic intervention) and in the phase autoantibodies had developed (prearthritis intervention). Meta-analyses suggested that treatment started in both phases was effective. However, none of the studies performed side-by-side comparisons of prophylactic, prearthritis and therapeutic interventions. Therefore, we cannot conclude whether the first two strategies are more effective than treatment initiated in the established disease phase. Similarly, the results obtained on prophylactic strategies cannot be compared with those of prearthritis strategies.
There are more limitations. Surprisingly, the majority of studies that aimed to test the efficacy of prophylactic treatment used an extended treatment period (average of 4.6 weeks, thus continuing within the phase of established disease). Principally, treatment is preventive if given in preclinical phases only. Studies that initiated treatment at a prearthritis stage did treat animals with a short course of (at average) 1 week and still observed less severe arthritis in the clinical phase of the disease.33–37
Furthermore, none of the studies evaluated the occurrence of clinical arthritis. Hence, there are no data from animal models to conclude whether clinical disease can be prevented. For human translation, it would be most interesting to determine whether preventive treatment can actually reverse autoimmunity and prevent RA.
The studies that were evaluated were heterogeneous in several aspects. The use of standard operating procedures for validation of results is crucial to reduce study heterogeneity. Using an 11-point-item quality checklist, we aimed to select studies that had a reliable study design; despite the funnel used, still considerable differences were present in the experiments that were included in the meta-analysis. Mice as well as rats were studied. In addition, results of two different animal models (CIA, AIA) were evaluated. Subanalyses stratified for CIA and AIA, however, showed similar results as that of the total group. Furthermore, arthritis severity was assessed in different ways. Although a validated method was used to compare these outcomes (NMD), this adds to the heterogeneity. For these different reasons, the NMDs—including those resulting from the meta-analyses performed for different disease phases and for the different treatments—should not be compared in their effect size. Thus, although the efficacy of different treatment strategies cannot be compared, this study provides an overview of all available data on animal models and provides an evaluation whether treatment initiated in very early disease phases is effective.
Based on the present evaluation of the available literature, we conclude that the ideal experiment on animals for this research question should still be performed. This study should test interventions side by side in different disease phases and with a similar treatment schedule to be able to compare efficacy. In addition, a head-to-head comparison of DMARDs like methotrexate, abatacept, rituximab and anti-TNF with a defined duration could answer the question whether prearthritis treatment can reverse autoimmunity and prevent arthritis in mouse models. Proper controls are sham-treated mice that develop a natural course of experimental-induced arthritis. The presence and evolution of systemic autoimmunity in CIA, defined by autoantibody production against CII, should be determined and linked to clinical outcome. Ideally, the effect of (a short course of) prearthritis treatment should be evaluated over an extended period of time to determine whether there is long-term arthritis-free ‘benefit’ or a delayed onset of arthritis.
In conclusion, this study systematically evaluated the results of animal studies and suggested that both prophylactic and prearthritis treatment strategies lead to a significant reduction of arthritis severity scores and hits at a possibility for preventive therapy in RA. However, larger studies are needed to confirm this.
References
Footnotes
Handling editor Tore K Kvien
Contributors JSD and JWS collected the data. JSD performed the analysis. AHMvdH-vM, TWH and RET supervised the project. All authors wrote and approved the manuscript.
Funding The authors acknowledge the financial support from the Dutch Arthritis Foundation, The Netherlands Organization for Scientific Research, the IMI JU funded project BeTheCure, contract no 115142-2. The work of AHMvH-vM was supported by a ZON-MW Vidi grant.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All relevant data are within the paper and its online supplementary information files.