Article Text

Abstract
Objectives To examine the extent and cost of work disability among patients with gout compared with matched population controls and to analyse predictors of work disability.
Methods A regional cohort study using data from Swedish national and regional registries from January 2000 through December 2012, including 4571 patients with gout of working age, with a first recorded diagnosis of gout in the years 2003–2009 and 22 482 population controls, matched by age, sex and place of residence. Differences in baseline characteristics (educational level, income, previous employment and comorbidities) and the number of work-loss days (absenteeism) due to sick leave and disability pension for 3 years after identification were calculated. Predictors for new-onset work absenteeism (>90 days/year) in a subset were determined by conditional logistic regression.
Results Patients with gout (median age 53 years) had significantly more comorbidities, lower income and lower level of education than matched controls. The average work absentee rate during the 3-year follow-up period was higher among patients with gout than controls, 22% and 14%, respectively (P<0.0001). New-onset absenteeism was in multivariate analyses significantly predicted by gout (OR 1.47; 95% CI 1.23 to 1.75). Other variables independently related to new-onset absenteeism were education ≤12 years, previous unemployment and history of sick leave, in addition to several comorbidities (renal disease, cardiovascular disease, alcohol abuse and obesity).
Conclusions Gout is associated with substantially higher work absenteeism and costs for society due to productivity loss, after adjusting for associated comorbidities and socioeconomic differences. Whether more intensive treatment of gout is cost-effective needs to be addressed in future studies.
- economic evaluations
- epidemiology
- gout
Statistics from Altmetric.com
Introduction
Gout is the most common form of inflammatory arthritis with a prevalence of 1.8% in the Western Swedish Health Care Region (WSHCR).1 Recent epidemiological studies from the UK, USA and Sweden have found an increasing incidence and prevalence of gout.1–3 The underlying disease mechanism of gout is high levels of circulating urate, causing monosodium urate crystal deposition in joints and soft tissues leading to recurrent episodes of painful arthritis,4–6 causing significant disability.7 8 Gout is associated with cardiovascular, renal and metabolic comorbidities, including diabetes, hyperlipidaemia, hypertension and coronary atherosclerosis.9–14
Treatment of gout consists of, on the one hand, anti-inflammatory therapy of acute attacks and, on the other hand, urate-lowering therapy (ULT). ULT is potentially curative as it halts ongoing crystal deposition and with time dissolves crystals already deposited. ULT is widely underused in clinical practice internationally and in the WSHCR.2 15–18
Patients with gout have been shown to have substantially higher direct healthcare costs for medical care and pharmaceuticals compared with matched controls, with most of the excess being explained by comorbid conditions.19 20 The indirect costs of gout in the form of absenteeism from work, presenteeism and associated costs of productivity loss have been less well studied. Productivity loss due to gout flares for patients with treatment refractory chronic gout was described in an uncontrolled study of 81 patients, finding that this group of patients on average was absent 25.1 days per year from work.21 Another US study found a linear relationship between indirect costs and number of gout flares per year when flares exceeded three per year.22 In Europe, cost of illness in gout, encompassing both direct and indirect costs, has been evaluated in a cohort study in Spain of 3130 patients from primary and specialist care23 and in Holland in a cohort study of 126 patients with gout treated by rheumatologists.24 Controlled studies providing data on the impact of gout on indirect costs on a population level are however lacking. The aims of the present study were therefore (1) to describe the difference in extent and costs of absenteeism due to sick leave (SL) and disability pension (DP) between patients with gout and population controls and (2) to determine socioeconomic and disease-related predictors of absenteeism.
Methods
Study design
This is a population-based cohort study of patients with gout who were of working age (≤62 years) at the time of their first recorded diagnosis and age-matched and sex-matched general population controls without gout. National and regional registers were used to assess work absenteeism due to SL and DP, as well as relevant confounders for the analyses. Data linkage was performed using the personal identification number, unique to every individual residing in Sweden.
Setting and study population
The Swedish healthcare system is tax-funded and offers universal access. Patients with gout are typically diagnosed and treated in primary care in Sweden. The Swedish Social Insurance Agency guarantees financial compensation to all individuals registered in Sweden who are unable to work due to disease or injury. Further details of the Swedish work disability compensation system are described in the online supplementary file.
Supplementary file 1
All inhabitants in the WSHCR from 1 January 2000 to 31 December 2012 constituted the study population. Approximately 1.6 million people, or 20% of the total population of Sweden, resides in the WSHCR, and the region is considered to be representative for Sweden with regard to health status and demographics.25 26
Register sources
The Western Swedish Health Care Register
The Western Swedish Health Care Register (VEGA) contains information about all healthcare contacts at inpatient and outpatient secondary clinics, as well as at primary care clinics, including date of contact and both primary and auxiliary diagnoses given by the treating physician according to the Swedish version of the International Statistical Classification of Diseases (ICD).
VEGA was used to identify gout cases and to determine the prevalence of predefined comorbidities for cases and population controls.
The Swedish census register
The census register contains demographic information on all registered individuals in Sweden as well as dates of deaths and emigrations. The census register was used to find up to five controls for each case, matched for age, sex and place of residence on municipality level at the date of identification. Controls were assigned the same date of identification as their corresponding case.
The Longitudinal Integration Database for Health Insurance and Labor Market Studies
The Longitudinal Integration Database for Health Insurance and Labor Market Studies (LISA) is administered by Statistics Sweden and holds annual registers on all individuals 16 years of age and older. Data on work-loss days due to SL and DP (absenteeism) per year as net days (see below for definition), excluding periods shorter than 14 days, were retrieved as well as data on education level, income and occupation (for further information regarding the Swedish Social Insurance system and time trends, see online supplementary text).
Laboratory database of the WSHCR
Laboratory data were available for cases but not for controls from the laboratory database of the WSHCR, containing laboratory results from the major regional laboratories.
The Swedish Prescribed Drug register
All prescribed drugs dispensed by Swedish pharmacies are recorded in the Swedish Prescribed Drug register. The register has been available since 1 July 2005. Dispensation of ULT and other medications could therefore only be determined for the part of the cohort included from 2006 and onwards.
Case definition
Gout cases were defined by having a first recorded diagnosis of gout in the years 2003–2009 by ICD-10 codes (M10 and M14.0) in VEGA. The VEGA database was searched from 1 January 2000 to 31 December 2002, resulting in a minimal period of 3 years free of visits to physician with a gout diagnosis before start of follow-up. Cases were included if their age at identification was 30–62 years, to allow for a follow-up period of 3 years before reaching the retirement age of 65 years.
For the descriptive analyses of overall differences between gout cases and controls, the whole study sample was used. For the predictor analyses, only cases and matched controls with no work-loss days (absenteeism) in the calendar year prior to the year of identification were included. Furthermore, for the predictor analyses, we only included individuals who had been residing in Sweden for the entire predictor period of 3 years previous to the year of identification (a full description of the case selection and exclusion process is available in the online supplementary file).
Definition of comorbidities and education level
Comorbidities (diabetes, cardiovascular disease (CVD) (hypertension, ischaemic heart disease, atrial fibrillation/flutter, congestive heart failure, thrombotic stroke or transient ischaemic attack), psoriasis, renal disease, transplantation, obesity, hyperlipidaemia and alcohol abuse) were identified in VEGA and were defined as the presence of at least one visit to a physician in primary or specialised care or a hospitalisation with a corresponding ICD-coded diagnosis occurring at least 1 day before the date of identification as case or control (for definitions used, see online supplementary table 2). VEGA was searched from 1 January 2000 to 30 December 2009 for predefined comorbidities, selected on the basis of having been shown in previous research to associate with gout. Serum urate (s-UA) measurements were only available in a minority of cases and thus not included in the analyses.
Data on education level were provided from Statistics Sweden and dichotomised into ≤12 years and >12 years. In the age group being studied, a length of education exceeding 12 years corresponds to a university-level education.
Follow-up
Cases were followed until the end of the year of identification and then for an additional three calendar years, that is, a case identified on 15 March 2006 was followed from 15 March 2006 until 31 December 2009. Matched controls were followed in an identical fashion.
Outcome
Data on work-loss days (absenteeism) for patients and population controls were collected from the LISA database for a period of three calendar years prior to the year of identification until three calendar years after the year of identification, excluding periods ≤14 days. All work-loss days were included irrespective of the form of compensation (SL or DP). The outcome variable studied was net days of SL and DP combined during each whole calendar year, including weekends and holidays, meaning that the maximum number of work-loss days each year was 365 days. One net day signifies a whole day lost from work, for example, 1 day with 100% SL, 4 days with 25% SL or 1 day with 75% DP and 25% SL. For predictor analyses, outcome was defined as having >90 net days of work loss during the calendar year after the year of identification.
Costs
Costs of absenteeism were estimated using the human capital approach (HCA). The HCA assumes that the cost of an individual’s lost productivity is equal to the amount an employer would be willing to pay for that production. One usually assumes this amount to be equal to the average gross salary plus employer contributions (social fees),27 28 which in Sweden are 31%.29 30 Costs were then calculated by multiplying the number of work-loss days each year with the average Swedish daily salary of that year with added social fees. The average daily salary with added employer contribution for women during the whole period was 120 EUR and 142 EUR for men. Salary figures were taken from the database of Statistics Sweden.31
Costs were converted to February 2017 SEK monetary value and then converted to euros using the February 2017 exchange rate (1€=9.48 SEK).
Statistics
Demographic and descriptive data were expressed in crude numbers and proportions (%). The difference between cases and controls in yearly net days lost from work due to SL and DP was assessed by analysis of variance, accounting for the matched design and applying non-parametric bootstrapping to calculate CIs. Conditional multivariable logistic regression taking into account the 1-to-5 matched design of the study was performed for the outcome of ≥90 days of work loss (absenteeism) in the year after identification. In the overall analyses of gout cases and controls together, age and sex were not included due to the matched design of this study. Logistic regression was also used to determine predictors of absenteeism among cases and controls separately. Significant interactions between examined predictors and the presence of gout were systematically searched for. All statistical analyses were performed in IBM SPSS Statistics V.24.
Results
Baseline characteristics
A total of 4571 individuals, aged 30–62 years, that received a diagnosis of gout in 2003–2009 were included in the study and were matched to 22 482 gout-free population controls. Men constituted 77% of the cohort, and the median age at identification was 53 years. The cohort selected for the prediction analyses consisted of 3029 cases and 11 556 controls. The prediction cohort was slightly younger, had fewer females and less comorbidities than the cohort as a whole (table 1). s-UA measurements were only available for 25% of the cases at the time of first diagnosis.
Characteristics of gout cases and population controls
Gout treatment
Data on dispensation of ULT, non-steroidal anti-inflammatory drugs (NSAIDs), colchicine and glucocorticosteroids were available for the part of the cohort included from 2006 and onwards (2613 cases and 12 787 controls). The proportions of cases filling at least one prescription during the first 365 days after diagnosis (for the period 2006–2012) were for ULT 28%, NSAIDs 39%, glucocorticosteroids 9% and colchicine 1%. In this subset, ULT ever-users had more days of work disability at all time points than never-users (data on file).
Sick leave and disability pension
Work-loss days (absenteeism)
The average number of work-loss days was significantly higher for gout cases compared with the general population controls at all time points during the 3-year follow-up. Patients with gout were absent from work on average 81 days per year (range: 80–82 days) while controls were absent on average 52 days per year (range: 51–53 days) (figure 1). In total, patients with gout were absent for 22% of the follow-up period while controls had 14% absenteeism.
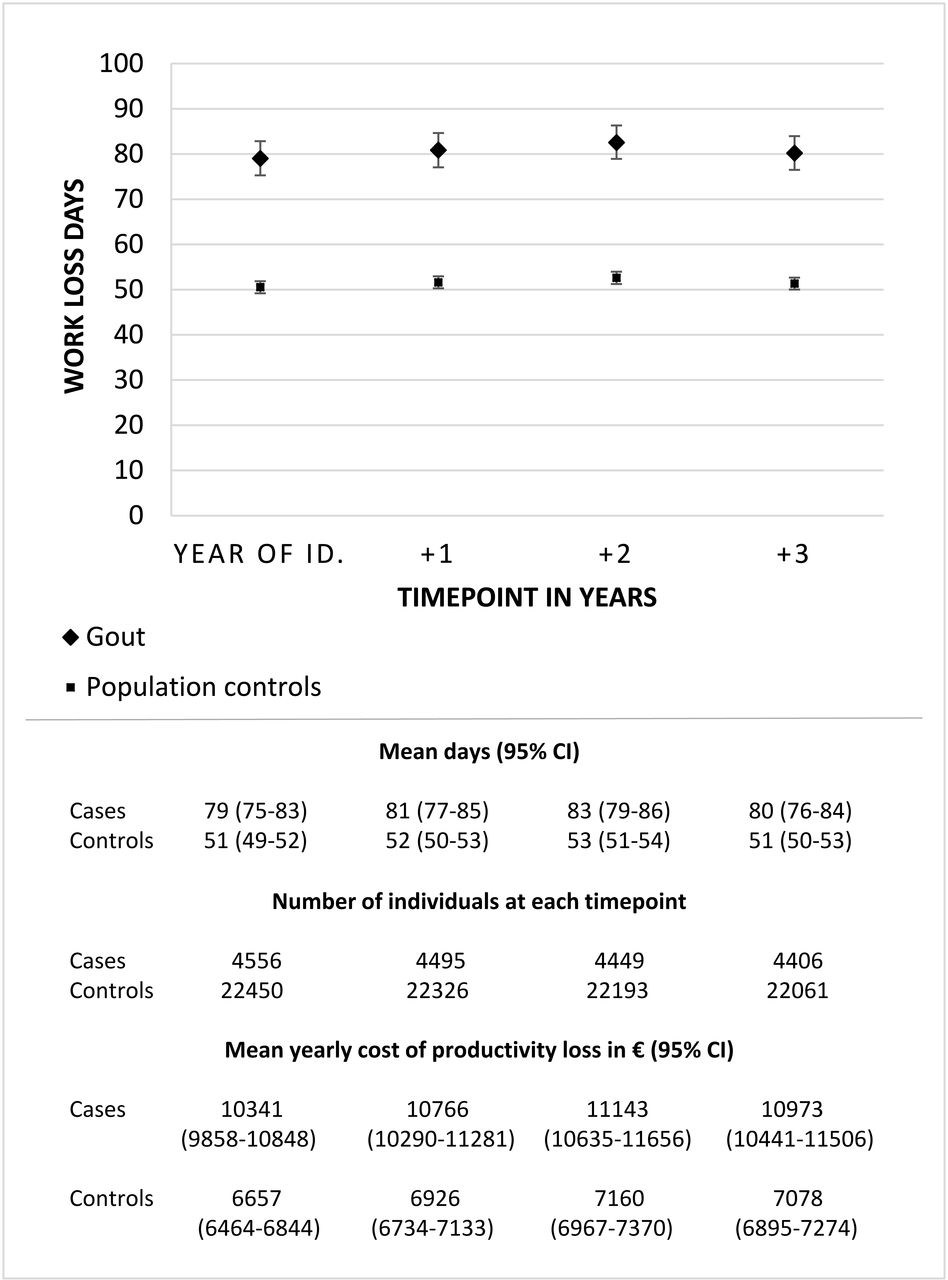
Mean work-loss days reimbursed as sick leave or disability pension, number of patients and mean costs for productivity loss per year for the whole cohort of gout identified in 2003–2009 and population controls matched for age, sex and place of residence. Error bars signify 95% CIs.
Productivity loss
The annual cost of productivity loss during follow-up in the gout group was €10 964 per individual compared with €7055 for controls (figure 1).
Predictors of new-onset work disability
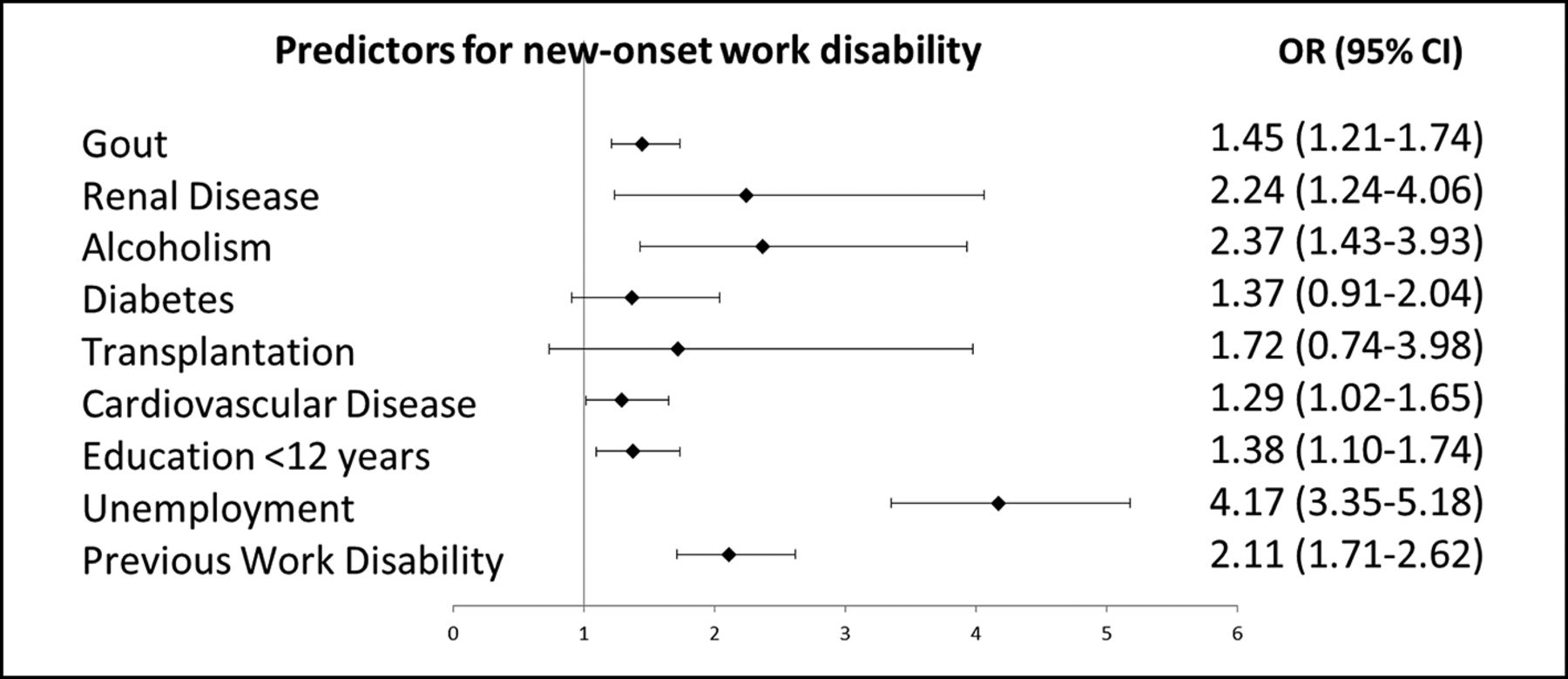
In total, 3029 patients with gout and 11 556 matched population controls did not have any work-loss days in the year before diagnosis (figure 2). Of these, 230 (7.6%) of the gout cases and 487 (4.2%) of the population controls had >90 net work-loss days in the year after identification. In a conditional multivariable logistic regression model, the strongest predictors of new-onset absenteeism in multivariate analyses were socioeconomic; education ≤12 years (OR 1.38; 95% CI 1.10 to 1.74), unemployment (OR 4.17; 95% CI 3.35 to 5.18) and history of SL (OR 2.11; 95% CI 1.71 to 2.62). In addition, a diagnosed gout (OR 1.45; 95% CI 1.21 to 1.74) and several comorbidities (renal disease, CVD, alcohol abuse, obesity) significantly predicted new-onset absenteeism (figure 3). Predictor analyses for cases and controls separately showed overall similar patterns (see online supplementary figure 3), thus not indicating any major interaction between gout and other predictors investigated.

Mean work-loss days reimbursed as sick leave or disability pension and number of individuals,including only subjects with no days of work loss in the calendar year preceding the year of identification.Population controls are matched for age, sex and place of residence. Error bars signify 95% CIs.
{kind=link}
{kind=link}
{kind=link}
Predictors for >90 days of new-onset work disability in the year after the year of identification.ORs with 95% CI.
Discussion
In this study, we demonstrate that patients with gout have 56% more work-loss days than population controls. This was in part, but not fully, explained by increased frequency of comorbidity in patients with gout (for a stratified analysis of patients with and without comorbidity, please see online supplementary figures 1 and 2). Absenteeism was strongly predicted by socioeconomic status and previous absenteeism. In addition to several other common comorbidities, gout significantly predicted absenteeism. Use of ULT in the subset with available prescription data is in line with earlier reports, demonstrating a low frequency of treatment.18 In the subset with available data, ULT users had more work-loss days than non-users. This is likely to be a reflection of suboptimal use of ULT, where treatment is preferentially given to patients with the most severe disease and even then most often with insufficient dosing.
Due to the scarcity of laboratory data on urate levels, we were unable to construct a definition of ‘optimised ULT’ in this cohort, making us unable to in this study assess whether such treatment lessened work disability. Further studied are needed to elucidate whether more intensive and focused gout treatment can reduce work disability among patients with gout.
It is well known from both research and official statistics that age, gender, place of residence (urban vs rural community) and socioeconomic status associate strongly with absenteeism.32 The mechanisms behind the increased absenteeism in this study for individuals with gout after taking demographic and socioeconomic confounders and major comorbidities into account are not completely understood but could be due to disease-related factors such as frequent gout attacks or pain and disability related to poorly treated chronic gouty arthritis. It is, however, also possible that the increased absenteeism among patients with gout could partly be due to residual confounding not captured in the available data, for example, related to lifestyle or work environment.
As a consequence of the increased absenteeism in patients with gout, the annual cost of productivity loss per patient with gout (€10 964) was significantly higher compared with controls. The annual cost was also larger than that estimated for patients with psoriatic arthritis in a recent Danish study (€5450),33 but not as high as has been estimated for rheumatoid arthritis patients (€16 907)34 or for individuals of working age that have recently had an ischaemic stroke (€13 588)35 in two Swedish studies.
Some limitations should be acknowledged. First, some selection bias towards more severe or advanced cases of gout being identified is introduced, as mild or early cases possibly do not seek healthcare for their condition. Second, when using register-based ICD codes there is always a possibility of misclassification. A previous validation study demonstrated a high validity for a more strict definition of gout requiring two or more visits with a gout diagnosis in primary care.36 As the baseline characteristics and comorbidity patterns of gout cases with one diagnosis were very similar to the characteristics of cases with multiple diagnoses of gout in this cohort (data on file), similar validity for the two definitions can be assumed. Third, absenteeism for SL periods ≤14 days could not be taken into account, and due to the episodic nature of gout this might rather have underestimated the effect of having a gout diagnosis. Fourth, we were unable to assess the costs of presenteeism due to lack of data. Fifth, misclassification of other exposures could be a problem. Regarding definitions for comorbidities, the validity of ICD codes in the Swedish national patient register is generally good,37 but all diagnoses used as covariates in this study have not been validated, such as obesity and alcohol abuse. It is notable that the prevalence of alcohol abuse and obesity in Sweden as measured by the annual public health surveys by the National Public Health Agency is significantly higher than what is found in this study,38 and we are thus likely to underestimate the occurrence of these comorbidities, when ICD codes were used for definitions. There is no reason to believe however that such under-reporting should be of a different magnitude for cases compared with controls. Lastly, it could be argued that results are not based on the most recent data. However, the relative disability rates, comparing cases and controls, were similar for all calendar years (see online supplementary table 5) and the overall disability rate for Sweden has only marginally changed between 2012 and 2016, arguments that support contemporary validity of our results.
The study has several strengths. First, the population-based design, including all gout cases in the region, reduces the risk of selection bias. Second, several unrelated independent data sources were used. For example, case identification and information regarding outcome were retrieved from completely independent sources. Data on socioeconomic factors, such as educational level and income, were retrieved from national registries with high coverage and data quality,39 40 precluding the need for using area-based markers of socioeconomic status.
In conclusion, gout is associated with substantially increased work disability. Costs of productivity loss are considerably higher for patients with gout compared with the general population after adjusting for comorbidities.
References
Footnotes
Handling editor Tore K Kvien
Contributors All authors were involved in the conception and design of the study. LJ and MD contributed to the acquisition of the data. All authors contributed to analysis and interpretation of the data and take responsibility for the integrity of the data and the accuracy of the analyses. All authors participated in the drafting of the manuscript or revised it critically for intellectual content. All authors approved the final version to be published.
Funding This study was supported by grants from The University of Gothenburg and The Swedish Rheumatism Association.
Competing interests None declared.
Ethics approval Ethical Review Board of Gothenburg, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.