Article Text

Abstract
Objectives To describe the incidence of atrioventricular (AV) block II–III, atrial fibrillation (AF), pacemaker implantation (PM) and aortic regurgitation in patients with ankylosing spondylitis (AS), undifferentiated spondyloarthritis (uSpA) and psoriatic arthritis (PsA) compared with the general population (GP) and with each other.
Methods A prospective nationwide study with cohorts of patients with AS (n=6448), PsA (n=16 063) and uSpA (n=5190) and a GP (n=2 66 435) cohort, identified in 2001–2009 in the Swedish National Patient and Population registers. Follow-up began on 1 January 2006 and ended at event, death, emigration or 31 December 2012. Age-standardised and sex-standardised incidence rates and hazard ratios (HRs) were calculated.
Results The highest incidence rates were noted for AF (5.5–7.4 events per 1000 person-years), followed by PM (1.0–2.0 events per 1000 person-years). HRs for AV block, AF, PM and aortic regurgitation were significantly increased in AS (HRs 2.3, 1.3, 2.1 and 1.9), uSpA (HRs 2.9, 1.3, 1.9 and 2.0) and PsA (HRs 1.5, 1.5, 1.6 and 1.8) compared with the GP cohort. The highest HRs were seen for AV block in male uSpA (HR 4.2) and AS (HR 2.5) compared with GP. Compared with PsA, significantly increased HRs were noted for PM (HR 1.5) in AS and for AV block (HR 1.8) in uSpA.
Conclusions Patients with SpA are at increased risk of aortic regurgitation, cardiac rhythm disturbances and, as a probable consequence, also PM. Particularly for AF, the most common arrhythmia, increased caution is warranted, whereas AV block should be looked for especially in men with AS or uSpA.
- ankylosing spondylitis
- psoriatic arthritis
- spondyloarthritis
- cardiovascular disease
Statistics from Altmetric.com
Introduction
Ankylosing spondylitis (AS) may increase the risk of cardiac manifestations, such as conduction disturbances and aortic regurgitation.1 2 Most of the existing studies regarding these cardiac manifestations in patients with AS are small scaled, some lack controls from the general population (GP) and the results have been inconsistent.3–10 In more recent studies of AS, the reported prevalence of (often subclinical) aortic regurgitation and conduction disturbances have been in the range of 10%–18% and 5%–33%, respectively.5–8
AS belongs to the spondyloarthritis (SpA), which is a cluster of rheumatic diseases with a spectrum of similar clinical features and a varying degree of association with HLA-B27.11 12 In this cluster of diseases, reactive arthritis has been associated with similar cardiac manifestations as AS.13–15 HLA-B27 has in itself been linked to conduction disturbances and aortic regurgitation, even in the absence of rheumatic disease.16 17 Therefore, other SpA subtypes, such as psoriatic arthritis (PsA) and undifferentiated SpA (uSpA), may presumably also have an increased risk of such cardiac manifestations. Furthermore, the risk of atrial fibrillation (AF), a commonly occurring arrhythmia in the GP, has hardly been studied in patients with SpA irrespective of subtype.18
The main aim of this study was therefore to investigate the incidence and risk of cardiac rhythm disturbances (atrioventricular (AV) block II–III, AF) and aortic regurgitation in patients with AS, PsA and uSpA compared with the GP and with each other. We also aimed to investigate the incidence and risk of pacemaker implantation (PM) as a possible consequence of severe arrhythmia.
Method
Study design and register sources
This is a prospective nationwide population-based cohort study, including three separate cohorts of patients with AS, PsA and uSpA identified from the Swedish National Patient Register (NPR) and one GP cohort identified from the Swedish Population Register. Through the unique personal identification number of each Swedish resident, the subjects were linked to NPR, the Population Register, Swedish Rheumatology Quality Register (SRQ), the Swedish Prescribed Drug Register (PDR) and the Swedish Register of Education to identify outcomes as well as sociodemographic data, comorbidities and pharmacological treatment in order to characterise the populations.
NPR was established in 1964 and contains data of inpatient care (with full national coverage from 1987) and from 2001 also non-primary outpatient care. Primary and secondary diagnoses reported by the physician are recorded at each visit according to the International Classification of Diseases (ICD). The register also includes surgical procedure codes.
The Population Register holds information of residency, immigration, emigration and deaths for all the Swedish residents.
PDR started in July 2005 and contains information regarding all dispensed prescriptions of pharmacological treatment, registered according to the Anatomical Therapeutic Chemical Classification (ATC) system.
SRQ started in 1995 and includes information on treatment with biological disease-modifying antirheumatic drugs (bDMARDs), with an estimated national coverage of 85% for patients with SpA treated with bDMARDs.19
Informed consent was not needed due to the register-based study design.
Study population
This study is part of a large-scale nationwide register linkage project, which identified all patients with a registered diagnosis of AS, PsA or uSpA, given at a visit to a physician, in NPR 1968 through 2009. From the Population Register, up to five controls per patient were identified, matched on birth year, sex and place of residence at the date when the index patient received his/her first SpA diagnosis in NPR.
AS, uSpA and PsA cohorts
From these larger groups of patients with SpA, we selected all patients with at least one physician visit with an AS, PsA or uSpA diagnosis in rheumatology or internal medicine outpatient care between 2001 and 2009, at the ages 18–99 years, alive and living in Sweden at start of follow-up. These patients were included in the AS (n=6448), PsA (n=16 063) or uSpA (n=5190) cohorts. Patients who also had received an ICD code indicating rheumatoid arthritis or systemic lupus erythematosus were excluded.
The ICD codes (online supplementary table S1) used to identify eligible patients have previously been validated. In patients with AS and available data of imaging and/or HLA-B27 status, the positive predicted values (PPVs) for fulfilling the modified New York criteria and any set of SpA criteria were 80% and 97%, respectively.20 The corresponding PPVs in uSpA were 26% and 89%, respectively.20 The PPVs of an ICD code for PsA within primary or specialised care was within the range of 63%–92%, where the highest proportion of confirmed PsA was noted if the PsA was diagnosed in specialised care (as the patients with PsA in the present study) and at least on two occasions.21
Supplementary file 1
Patients diagnosed with ≥2 subtypes of SpA
Patients with ICD codes for more than one subtype of SpA diagnosis before start of follow-up were not included in the AS, PsA or uSpA cohorts but analysed separately to avoid case mixing (n=1082).
GP cohort
All initially identified GP controls from the first register extraction, at the ages 18–99 years, alive and living in Sweden at start of follow-up, were included in the GP cohort (n=2 66 435) and analysed as unmatched GP comparators. GP comparators were excluded from the GP cohort if they had been diagnosed with AS, uSpA or PsA before start of follow-up (n=340).
Definition of outcome
The primary outcomes were incident AV block II–III, AF, PM and aortic regurgitation. Each outcome was analysed separately. The outcomes were identified in NPR and defined as follows:
First occurrence of AV block II–III reported as a primary or secondary diagnosis from either inpatient or outpatient care.
First occurrence of AF reported as a primary or secondary diagnosis from either inpatient or outpatient care.
First occurrence of PM reported as a surgical procedure code in either inpatient or outpatient care.
First occurrence of isolated aortic regurgitation reported as a primary or secondary diagnosis in either inpatient or outpatient care. Aortic regurgitation in combination with stenosis was not included.
The ICD codes used to identify the outcomes are described in online supplementary table S1. Importantly, subjects with a history of the outcome of interest prior to start of follow-up were excluded from that specific analysis.
Follow-up
The follow-up started on 1 January 2006 for subjects receiving their first AS, uSpA or PsA diagnosis in rheumatology or internal medicine outpatient care prior to 30 June 2005 and 6 months after the date of first diagnosis for those with a first registered diagnosis after 30 June 2005. This was done to make the rates comparable in SpA contra GP, by reducing the risk for detection bias in the SpA cohorts as a result of increased surveillance in connection with receiving an SpA diagnosis. For GP subjects, the follow-up began on 1 January 2006 or the date of immigration if this occurred later than 1 January 2006.
All subjects were followed until first occurrence of outcome, emigration, death or 31 December 2012, whichever occurred first. Subjects were censored in the GP cohort if diagnosed with an SpA diagnosis and subsequently eligible to enter the corresponding SpA cohort. Patients were censored from their original SpA cohort if diagnosed with a different SpA subtype during follow-up and subsequently eligible to enter the SpA cohort with ≥2 subtypes of SpA (described above).
Baseline characteristics
Cardiovascular and SpA-related comorbidities were regarded as prevalent at baseline if the specified ICD codes and surgical procedure codes (online supplementary table S1) were identified in NPR before start of follow-up. Pharmacological treatment at baseline was defined as a dispensed prescription within 6 months before start of follow-up according to specified ATC codes in PDR (online supplementary table S1). Current treatment with the intravenous tumour necrosis factor-inhibitor infliximab was retrieved from SRQ. From the Register of Education, we retrieved level of education as a measure of socioeconomic status.
Statistical analyses
Descriptive statistics are presented as number (percentage) or mean±SD. For each outcome, incidence rates, overall and stratified by sex, were calculated from the number of incident events and person-years at risk. To enable comparison between the cohorts, standardised incidence rates were calculated, using the age and sex distribution in the GP cohort as standard. For incidence rates, we assumed a Poisson distribution when estimating 95 % CI. For the risk assessment, age-adjusted and sex-adjusted HRs were calculated using Cox proportional hazard regression analyses, with the GP cohort and the largest SpA cohort—the PsA cohort—as the reference populations. The proportional hazards assumption for the Cox regression analyses was evaluated graphically and considered fulfilled in all analyses. Further adjusted HRs, with additional selected covariates from baseline characteristics, were calculated (online supplementary data). We also calculated age-standardised and sex-standardised prevalence and corresponding prevalence ratio (PR) at baseline for prior AV block, AF, PM and aortic regurgitation in the SpA cohorts, using the age and sex distribution in the GP cohort as standard/reference. Statistical analyses were performed by PASW Statistics V.19 and SAS V.9.3.
Results
Study population
Cohorts of patients with AS (n=6448), PsA (n=16 063) and uSpA (n=5190) and one with GP comparators (n=2 66 435) were identified. Baseline characteristics are presented in table 1. All SpA cohorts had a significantly increased age-standardised and sex-standardised PR for prior AV block, AF, PM and aortic regurgitation compared with the GP cohort (online supplementary table S2).
Baseline characteristics of patients with AS, uSpA, PsA and GP comparators at start of follow-up
AV block II–III
During follow-up, 31, 17 and 55 AV block events occurred in the AS, uSpA and PsA cohorts, respectively, resulting in standardised incidence rates of 0.9, 1.2 and 0.7 AV block events per 1000 person-years at risk compared with 0.5 in the GP cohort (table 2). The age-adjusted and sex-adjusted HRs (95% CI) were significantly increased in AS (2.3 (1.6 to 3.3)), uSpA (2.9 (1.8 to 4.7)) and PsA (1.5 (1.1 to 1.9)) compared with the GP cohort. In the sex-stratified analyses, the highest age-adjusted HR point estimates were noted for male uSpA (4.2 (2.5 to 7.0)) and AS (2.5 (1.7 to 3.7)) compared with the male GP cohort. When compared with PsA, significantly increased HRs were noted for uSpA patients overall and for male uSpA in the sex-stratified analyses. No statistically increased HRs for AV block were noted for any of the groups of female patients with SpA neither compared with female GP comparators nor compared with female patients with PsA. (figure 1)
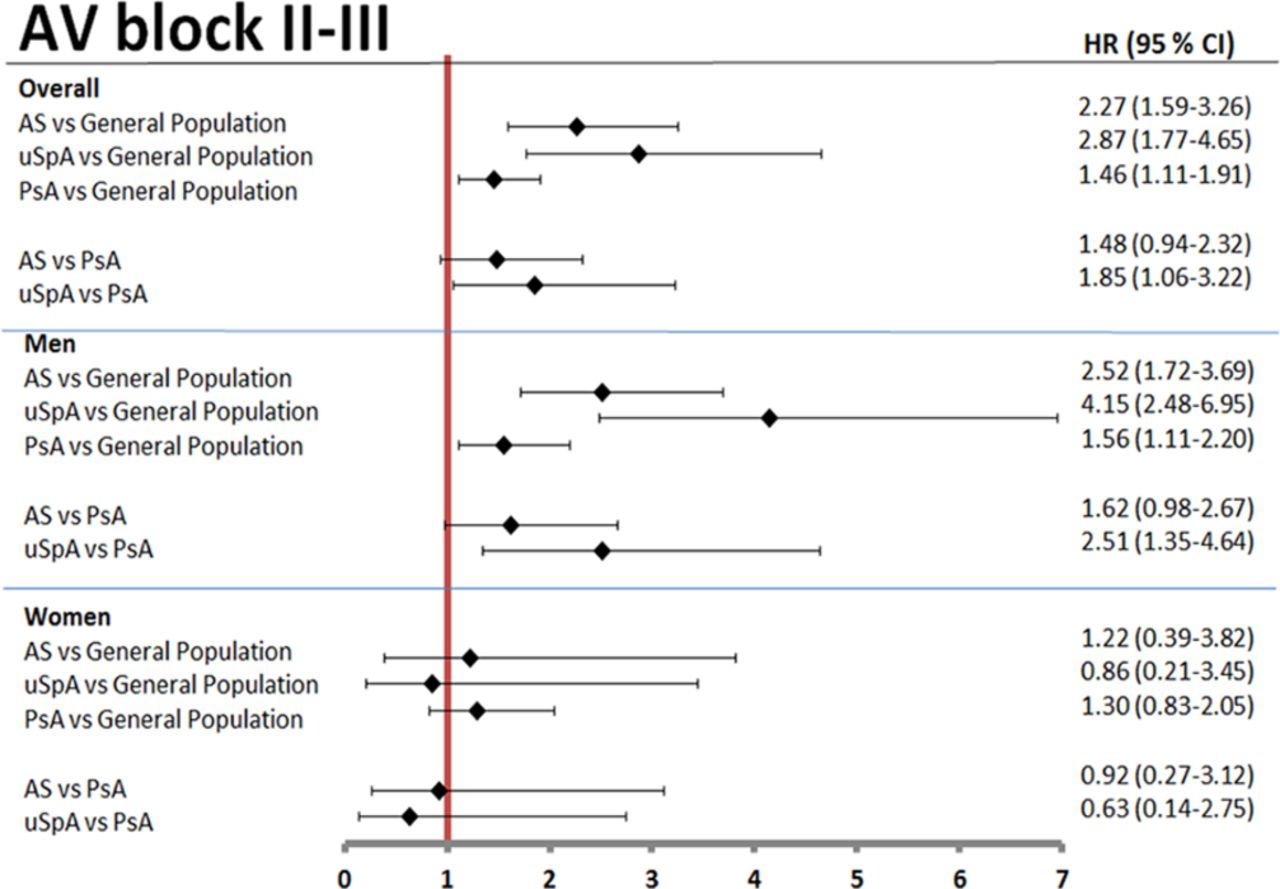
Age-adjusted and sex-adjusted HRs for AV block II–III, overall and stratified by sex, in patients with AS, uSpA and PsA using general population comparators and patients with PsA as reference. AS, ankylosing spondylitis; AV, atrioventricular; PsA, psoriatic arthritis; uSpA, undifferentiated spondyloarthritis.
Incidence rates of atrioventricular block, atrial fibrillation, pacemaker implantation and aortic regurgitation in patients with AS, uSpA, PsA and in GP comparators
Atrial fibrillation
Based on 174, 77 and 560 AF events in the AS, uSpA and PsA cohorts, respectively, the standardised incidence rates were 7.1, 6.4 and 7.4 AF events per 1000 person-years at risk compared with 5.5 in the GP cohort (table 2). The age-adjusted and sex-adjusted HRs were significantly increased in AS (1.3 (1.2 to 1.6)), uSpA (1.3 (1.0 to 1.6)) and PsA (1.5 (1.3 to 1.6)) compared with the GP cohort. There were no significant differences between AS and uSpA compared with the PsA cohort. (figure 2)

Age-adjusted and sex-adjusted HRs for atrial fibrillation, overall and stratified by sex, in patients with AS, uSpA and PsA using general population comparators and patients with PsA as reference. AS, ankylosing spondylitis; PsA, psoriatic arthritis; uSpA, undifferentiated spondyloarthritis.
Pacemaker implantation
During follow-up, 53, 21 and 113 PM events occurred in the AS, uSpA and PsA cohorts, respectively, resulting in standardised incidence rates of 2.0, 1.5 and 1.5 PM events per 1000 person-years at risk compared with 1.0 in the GP cohort (table 2). The age-adjusted and sex-adjusted HRs were significantly increased in AS (2.1 (1.6 to 2.8)), uSpA (1.9 (1.2 to 2.9)) and PsA (1.6 (1.3 to 1.9)). In the sex-stratified analyses, the highest age-adjusted HR point estimate was noted for male patients with uSpA (2.9 (1.8 to 4.6)). A significantly increased age-adjusted and sex-adjusted HR was noted in AS (1.5 (1.0 to 2.1)) compared with PsA (figure 3).
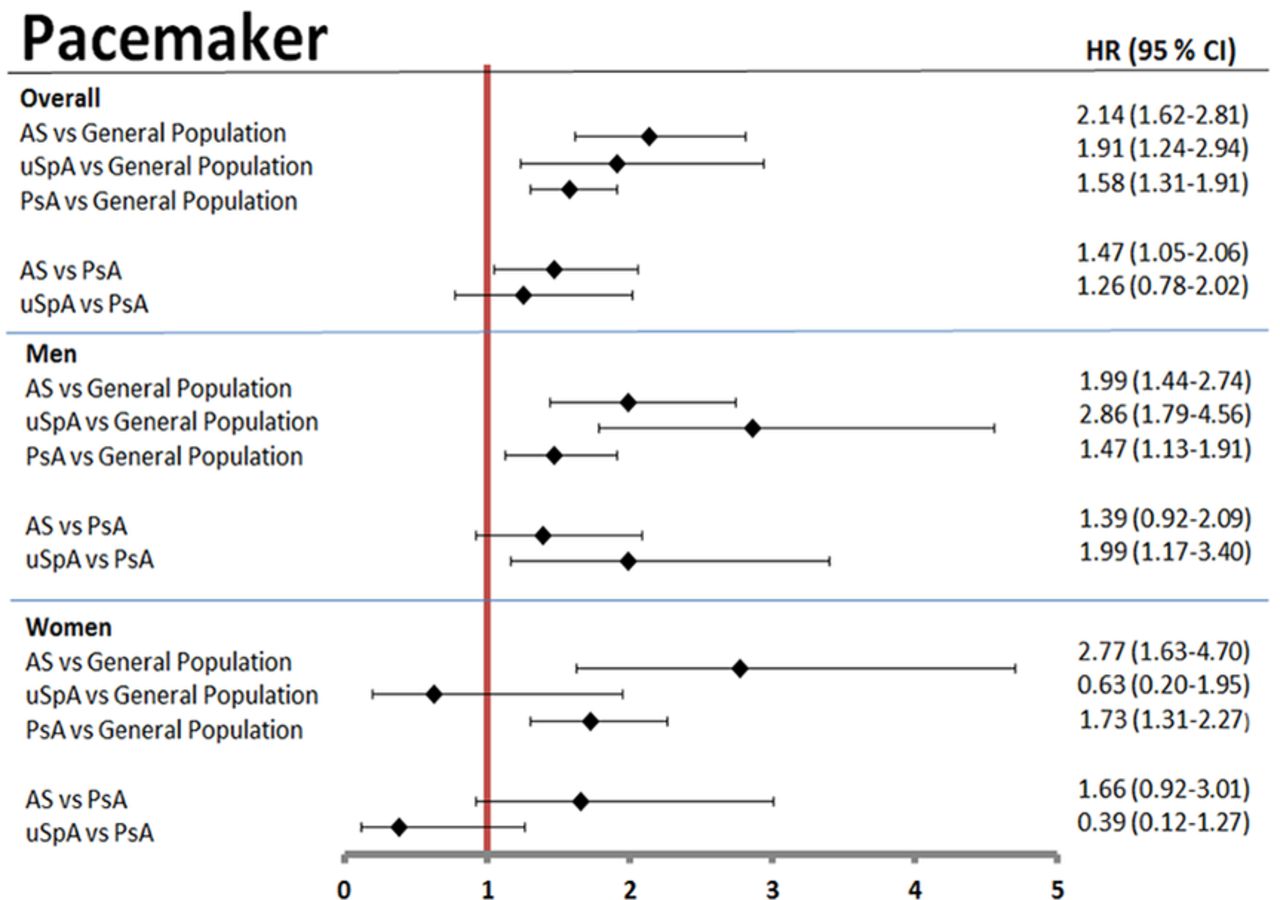
Age-adjusted and sex-adjusted HRs for pacemaker implantation, overall and stratified by sex, in patients with AS, uSpA and PsA using general population comparators and patients with PsA as reference. AS, ankylosing spondylitis; PsA, psoriatic arthritis; uSpA, undifferentiated spondyloarthritis.
As a sensitivity analysis, subjects with prior AF/AV block at baseline were excluded from the PM analysis, resulting in only slightly attenuated HRs (data not shown).
Aortic regurgitation
Based on 24, 13 and 62 aortic regurgitation events in the AS, uSpA and PsA cohorts, respectively, the standardised incidence rates were 0.7, 0.7 and 0.7 events per 1000 person-years at risk compared with 0.4 in the GP cohort (table 2). The age-adjusted and sex-adjusted HRs were significantly increased in AS (1.9 (1.3 to 2.9)), uSpA (2.0 (1.2 to 3.5)) and PsA (1.8 (1.4 to 2.4)) compared with the GP cohort. (figure 4)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Age-adjusted and sex-adjusted HRs for aortic regurgitation, overall and stratified by sex, in patients with AS, uSpA and PsA using general population comparators and patients with PsA as reference. AS, ankylosing spondylitis; PsA, psoriatic arthritis; uSpA, undifferentiated spondyloarthritis.
Supplementary data
Subjects (n=1931) excluded prior to study entry or censored during follow-up based on ICD codes for two or more different SpA subtypes were analysed separately (online supplementary tables S3 and S4). The majority (n=1169) had an overlap of AS and uSpA diagnoses. Incidence rates and HRs for the outcomes did not diverge substantially from the main results.
Characteristics of the subjects with AV block/AF/PM/aortic regurgitation and co-occurrence during follow-up are available in online supplementary tables S5–S8. For PM, the majority had an AV block or/and AF at baseline or during follow-up.
Overall HRs, adjusting for multiple confounders in addition to age/sex, resulted in slightly lower point estimates compared with the age/sex-adjusted main analyses (online supplementary table S9).
Discussion
In this nationwide prospective population-based cohort study, we found an increased risk of aortic regurgitation, AV block, AF and accordingly an increased risk of PM in all three studied SpA subtypes compared with GP. Patients with AS and uSpA had a twofold increased risk for PM compared with GP, and AS also had a significantly increased risk compared with PsA.
These results confirm the previously known association between AS and conduction disturbances and aortic regurgitation, likewise the presumed association with the other SpA subtypes, especially uSpA and to a lesser extent PsA. In similarity to our result, Szabo et al found an increased standardised PR (1.6 (1.3 to 1.9)) for aortic valvular heart disease in patients with AS compared with GP.22 Very limited data are available regarding PsA. One previous study identified subtle involvement of the AV node, measured by prolonged PR interval, in patients with PsA compared with controls.23
In the sex-stratified analyses, the risk of AV block was elevated in male but not female patients compared with GP and especially elevated in male patients with AS or uSpA. Our findings could be seen in the context of other recognised sex differences in AS, such as more radiographic alterations in male contra female patients.24 25 In a study of extra-articular manifestations in patients with AS compared with controls, men with AS had higher risk estimates than the women, especially for uveitis.26 In addition, Bergfeldt and Möller have previously demonstrated a sex difference in pacemaker-treated AV block, where male but not female patients had a significantly increased frequency of HLA-B27.27 Male sex is a risk factor for AV block in the GP, resulting in low numbers of AV block in the female cohorts, which may have hampered the statistical power.28
The increased risk of AF may partly explain the increased risk of stroke shown in patients with SpA.22 29–31 AF is therefore an important risk factor to identify and treat in these patients, and intervention could possibly reduce the occurrence of stroke.32 In patients with psoriasis, three previous studies have found an increased risk of AF with risk levels that are in agreement with our result, although results are not entirely consistent.33–36
According to a previous Swedish study, the most common aetiology for PM in the GP was conduction system fibrosis, followed by ischaemic heart disease. Electrocardiographical indications for PM were related to AV conduction disorders and AF in 38% and 15%, respectively.37 Another study demonstrated that first-degree AV block was associated with a threefold increased risk of future PM and also with an increased risk of AF.38 Based on these results, the increased risk of PM in SpA is likely to be attributable largely to the increased incidence of AV block and AF. This is in accordance with our own results, which show a considerable co-occurrence between PM and AV block/AF (online supplementary table S7).
In the present study, the low incidence rates and absolute risk differences between groups, especially for AV block and aortic regurgitation, may suggest limited clinical importance. On the other hand, the method used for detecting these outcomes in the present study by registered diagnoses is likely, except for PM, to underestimate the true occurrence. The increased HRs demonstrated for all the studied cardiac outcomes in the different SpA subtypes highlight the need of awareness in case of symptoms, both obvious and vague, that may be related to these cardiac manifestations.
Some limitations of the study need to be acknowledged. First, we cannot exclude misclassifications of the SpA diagnoses or the outcomes. However, the ICD codes used for identification of AS, PsA and uSpA as well as AF are validated before with high validity/PPVs.20 21 39 Second, patients with SpA who were solely followed in primary care, and presumably have less severe disease, were not included, and this may have influenced the generalisability of our results. In Sweden, patients with SpA without DMARDs may be monitored in primary care but are predominately diagnosed in rheumatology or internal medicine outpatient care and would thus have been identified in our study. Furthermore, outcomes diagnosed only in primary care are not identified. Third, we cannot exclude the possibility for a detection bias based on more thorough search for AV block and aortic regurgitation in patients with SpA. Fourth, due to the register-based design, we lack detailed information on an individual level (smoking habits, body mass index, SpA activity measurements, etc). We have deliberately avoided adjustments in the main analyses for other factors than age/sex, and the aim was to assess rather than try to explain what causes the increased risks of the studied outcomes. Finally, the association between conduction disturbances and the different SpA types should preferably been related to HLA-B27 status, which unfortunately was not available.
The present study also have several strengths. First, it is the first study to our knowledge that compares the risk of cardiac rhythm disturbances and aortic regurgitation in different subtypes of SpA in the same setting simultaneously. Second, the large study population made it possible to study also rare events. Third, it is a population-based study of healthcare registers, minimising problems with selection bias and with negligible loss of follow-up.
To conclude, patients with SpA are at increased risk of aortic regurgitation, cardiac rhythm disturbances and, as a probable consequence, also PM. Particularly for AF, the most common arrhythmia, increased caution is warranted, whereas AV block should be looked for especially in men with AS or uSpA.
Acknowledgments
We thank Jonas Söderling for helping us with the initial extraction of the register-linked data and statistician Tatiana Zverkova Sandström for preparation of the extracted data.
References
Footnotes
Handling editor Hans WJ Bijlsma
Contributors KB contributed to the design of the study, data acquisition, analysis and interpretation of data and drafting the manuscript. HF-dE contributed to the interpretation of data and drafting the manuscript. EL, EK, MD, SE and UL contributed to the interpretation of data and have revised the manuscript critically for important intellectual content. JA contributed to the design of the study, interpretation of data and has revised the manuscript critically for important intellectual content. LTHJ contributed to the design of the study, interpretation of data and drafting the manuscript. All authors have read and approved the final manuscript.
Funding This work was supported by grants from the University of Gothenburg, the Region Västra Götaland, Sahlgrenska University Hospital (agreement concerning research and educations of doctors), Stockholm County Council (ALF), the Medical Society of Gothenburg, Göteborg’s Association Against Rheumatism, Swedish Rheumatism Association, the Swedish Research Council, the Swedish Heart-Lung Foundation and the Swedish Foundation for Strategic research.
Competing interests HF-dE has received advisory board fees from Sandoz and Novartis and unrestricted grant from Novartis. EL has received consultancy and/or speaker honoraria from Abbvie, Celgene, Pfizer and UCB. JA has received research grants from Abbvie, AstraZeneca, Merck, Pfizer, Roche, Samsung and UCB in relation to work based on the Swedish Biologics Register ARTIS. JA reported participating in research projects fully or partly funded by Novo Nordisk. LJ has received advisory board fees from Abbvie, Pfizer and Novartis. All other authors declare that they have no competing interests.
Ethics approval Regional Ethics Committee, Stockholm, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data sets generated and/or analysed during the present study are not publicly available due to the Swedish legislation (the Personal Data Act). The authors have access to raw data for the present study and may be contacted for inquiries.
Author note Some of the preliminary results have been presented as an oral abstract at American Congress of Rheumatology 2015 and as abstract/poster at the Swedish Rheumatology Meeting 2016.40 41