Article Text

Abstract
Background Venous thromboembolism (VTE), including pulmonary embolism (PE) and deep venous thrombosis (DVT), can be life threatening. An increased frequency of VTE has been found in inflammatory conditions. To date, evidence assessing whether this risk is also greater in patients with ankylosing spondylitis (AS) is scarce.
Methods Using the provincial British Columbia, Canada healthcare database that encompasses all residents within the province, we conducted matched cohort analyses of incident PE, DVT and overall VTE among incident cases of AS and compared them with individuals randomly selected from the general population without AS. We calculated incidence rates (IRs) of VTE and multivariable analyses after adjusting for traditional risk factors using Cox models.
Results Among 7190 incident cases of AS, 35 developed PE and 47 developed DVT. IRs of PE, DVT and overall VTE per 1000 person-years for patients with AS were 0.79, 1.06, 1.56 compared with 0.40, 0.50, 0.77 in the control cohort. Corresponding fully adjusted HRs (95% CI) of PE, DVT and VTE were 1.36 (0.92 to 1.99), 1.62 (1.16 to 2.26) and 1.53 (1.16 to 2.01), respectively. The risks of PE, DVT and VTE were highest in the first year of diagnosis with HR (95% CI) of 2.88 (0.87 to 9.62), 2.20 (0.80 to 6.03) and 2.10 (0.88 to 4.99), respectively.
Conclusions These findings demonstrate an increased risk of VTE in the general AS population. This risk appears the most prominent in the first year after diagnosis.
- spondylitis
- ankylosing
- spondyloarthritis
- venous thromboembolism
- deep venous thrombosis
- pulmonary embolism
- thromboembolism
- risk
Statistics from Altmetric.com
- spondylitis
- ankylosing
- spondyloarthritis
- venous thromboembolism
- deep venous thrombosis
- pulmonary embolism
- thromboembolism
- risk
Key messages
What is already known about this subject?
Increased risk of cardiovascular mortality, mainly arterial events (myocardial infarction and stroke), has been widely demonstrated in inflammatory diseases, including ankylosing spondylitis (AS).
There is limited evidence on the risk of venous thromboembolism (VTE) including deep venous thrombosis (DVT) and pulmonary embolism (PE) inpatients with AS.
What does this study add?
Using a large general population of patients with newly diagnosed AS, we demonstrated a 53% and 63% increased risk of VTE and DVT, respectively. The risk of PE was increased by 36%, but this was not statistically significant.
Our time-trend analysis suggested the highest risk was in the first year after AS diagnosis (threefold) but this did not achieve statistical significance.
How might this impact on clinical practice or future developments?
Clinicians should have an increased awareness of this rare but potentially life-threatening complication.
Future studies will be needed to identify patients at higher risk for this preventable complications. Moreover, further research should assess the potential role of treatment on the risk of VTE is needed.
Introduction
Venous thromboembolism (VTE), which includes deep venous thrombosis (DVT) and pulmonary embolism (PE), is a life-threatening disease1–3 with an estimated 1-year mortality rate exceeding 20%.3 Several studies have demonstrated an increased risk of VTE among patients with chronic inflammatory and autoimmune diseases.4–10
Ankylosing spondylitis (AS) is a chronic inflammatory arthritis that characteristically affects the spine. A number of studies have demonstrated an increased risk of cardiovascular and overall mortality in patients with AS11–14 but there is a paucity of literature on the incidence of VTE in this population. Previous reports are based on case reports15–17 and hospital administrative data,18–20 limiting generalisability. To the best of our knowledge, only one population-based study using the Swedish National Patient Register has assessed the risk of VTE in patients with AS and found a 50% increased risk of VTE in patients with AS when compared with the general population.21
The aim of this study was to evaluate the risk of incident VTE among patients with newly diagnosis of AS in a general population context. Moreover, we explored the impact of time trends on the risk of VTE during follow-up.
Methods
Data source
Universal healthcare coverage is available for all residents of British Columbia, Canada (population ~4.5 million). Population Data BC captures all provincially funded healthcare services data since 1990, including: all outpatient medical visits,19 hospital admissions and discharges,20 interventions,19 investigations,19 demographic data,22 cancer registry23 and vital statistics.24 Furthermore, Population Data BC encompasses the comprehensive prescription drug database PharmaNet,25 which includes all dispensed medications for all BC residents since 1996. Several other studies have been successfully conducted using Population Data BC databases.26–31
Study design
Using Population Data BC, we conducted matched cohort analyses of incident PE, DVT and both outcomes combined (VTE) among incident cases of AS (AS cohort) and compared them with individuals randomly selected from the general population without AS (comparison cohort). The comparison cohort was created by matching up to 10 individuals without AS to each AS case based on age, sex and calendar year of study entry.
Incident as cohort
An incident AS cohort included individuals diagnosed for the first time between January 1996 and December 2012 with no previous recorded history or diagnosis of AS in the preceding 6 years. Patients with AS were defined based on the following algorithm: ≥2 International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes for AS (ICD-9-CM 720.X) and/or ICD-10 code M45.X, ≥2 months apart but within a 2-year period. Codes were counted either from outpatient physician visit or hospitalisation with AS in the primary position.
Ascertainment of PE and DVT
Incident VTE cases were defined with a recorded ICD-9-CM (PE: 415.1, 673.2 or 639.6, DVT: 453) or ICD-10-CM (PE: O88.2 or I26; DVT: I82.4 or I82.9) code during the follow-up and a prescription for anticoagulants (heparin, enoxaparin, warfarin, Coumadin or similar agents) 1 month prior or 6 months after a VTE diagnosis. Patients with a previous ICD-9-CM code for VTE prior to entry into the cohort were excluded as well. Previous studies have demonstrated that these definitions have a positive predictive value of 94%.32
Assessment of covariates
Relevant covariates were recognised risk factors for VTE including alcoholism, hypertension, sepsis, varicose veins, inflammatory bowel disease, trauma, fracture, surgery, healthcare utilisation and medications such as glucocorticoids, hormone replacement therapy, contraceptives and cyclooxygenase 2 inhibitors.33 All covariates were assessed in the year prior to cohort entry (index date). The Charlson’s Comorbidity Index for administrative data34 35 was also calculated in the year before prior to cohort entry.
Cohort follow-up
Patients who met the inclusion and exclusion criteria from 1 January 1996 to 31 December 2012 were followed until they either developed an outcome, died, disenrolled from the health plan (ie, left the province; approximately 1% per year), or until follow-up ended, whichever occurred first.
Statistical analysis
We compared baseline characteristics between the AS and comparison cohorts. We identified incident cases of PE and DVT during the follow-up period and calculated incidence rates (IRs) of PE and DVT, both individually and in combination (ie, VTE), per 1000 person-years. We estimated the cumulative incidence of each event accounting for the competing risk of death by using the SAS macro CUMINCID and graphically presented these results.36 Furthermore, we used Cox proportional hazard regression models to assess the risk of PE and DVT associated with AS after adjusting for covariates. We entered covariates one at a time into the Cox models in a forward selection according to each confounder’s impact on the HR relative to the HR in the model selected in the previous step. Cut-off for the minimum important relative effect at each step was set to 5%.37 In order to evaluate the impact of duration of AS (ie, follow-up time after AS diagnosis), we estimated the HR yearly for the first 5 years. We used SAS V.9.3 (SAS Institute) for all analyses and we calculated 95% CIs for all HRs. Also, all p values were two sided.
We performed two sensitivity analyses. First, we estimated the cumulative incidence of each event accounting for the competing risk of death.38 We also determined the potential impact that a hypothetical unmeasured confounder might have on our estimates of the association between AS and the risk of VTE.39 We simulated unmeasured confounders, with their prevalence ranging from 10% to 20% in the AS and control cohorts, and ORs, ranging from 1.3 to 3.0 for the associations between the unmeasured confounder and both PE/DVT or VTE and the exposure (AS).
Role of funding
The funding sources had no role in the design, conduct or reporting of the study, or the decision to submit the manuscript for publication.
No personal identifying information was made available as part of this study. Procedures were in compliance with British Columbia’s Freedom of Information and Privacy Protection Act.
Results
Baseline characteristics
The overall cohort included 7190 incident AS and 71 900 age-matched, sex-matched and entry-time-matched comparison cases with a mean follow-up time of 6.2 years for all three outcomes. Baseline characteristics of these two cohorts are summarised in table 1. Compared with the comparison cohort, the AS cohort had more comorbidities at baseline (hypertension, sepsis, inflammatory bowel disease, fractures, surgery), higher use of medications, (glucocorticoids, hormone replacement therapy, oral contraceptive use, aspirin, cyclooxygenase 2 inhibitors) and higher resource utilisation (number of outpatient visits and hospitalisation) and higher Charlson’s Comorbidity Index scores.
Characteristics of ankylosing spondylitis (AS) and comparison cohorts at baseline
Association between a diagnosis of As and incident VTE
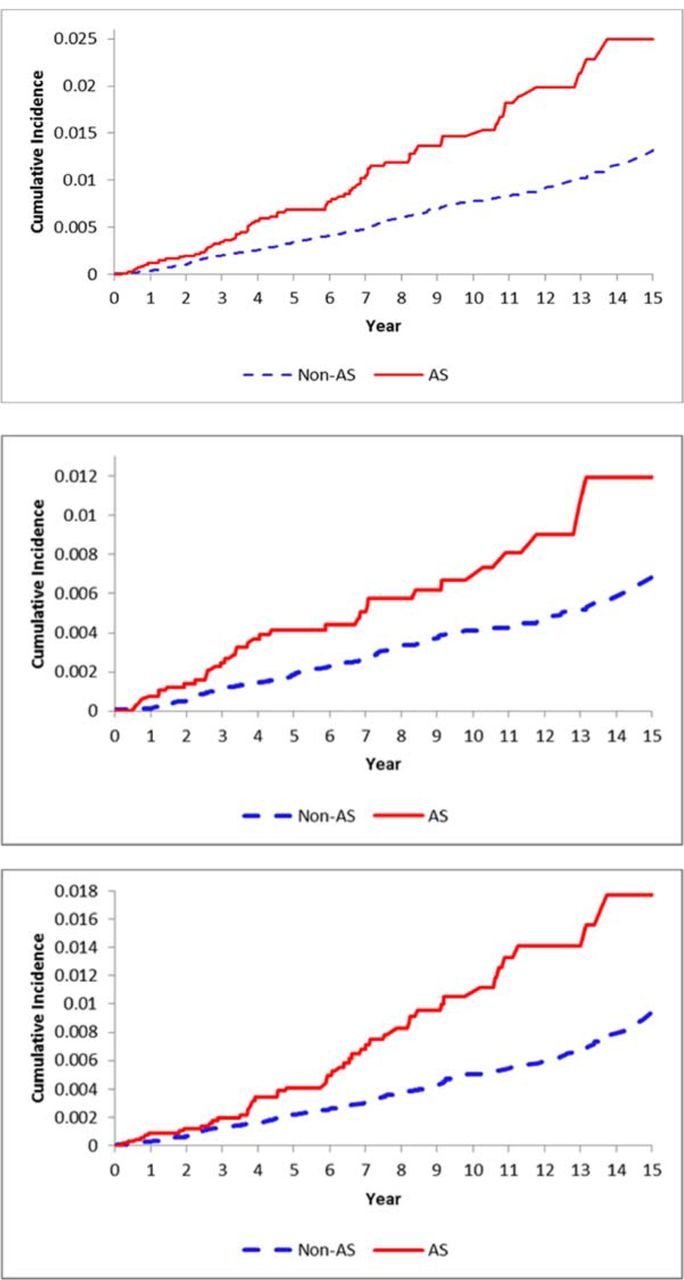
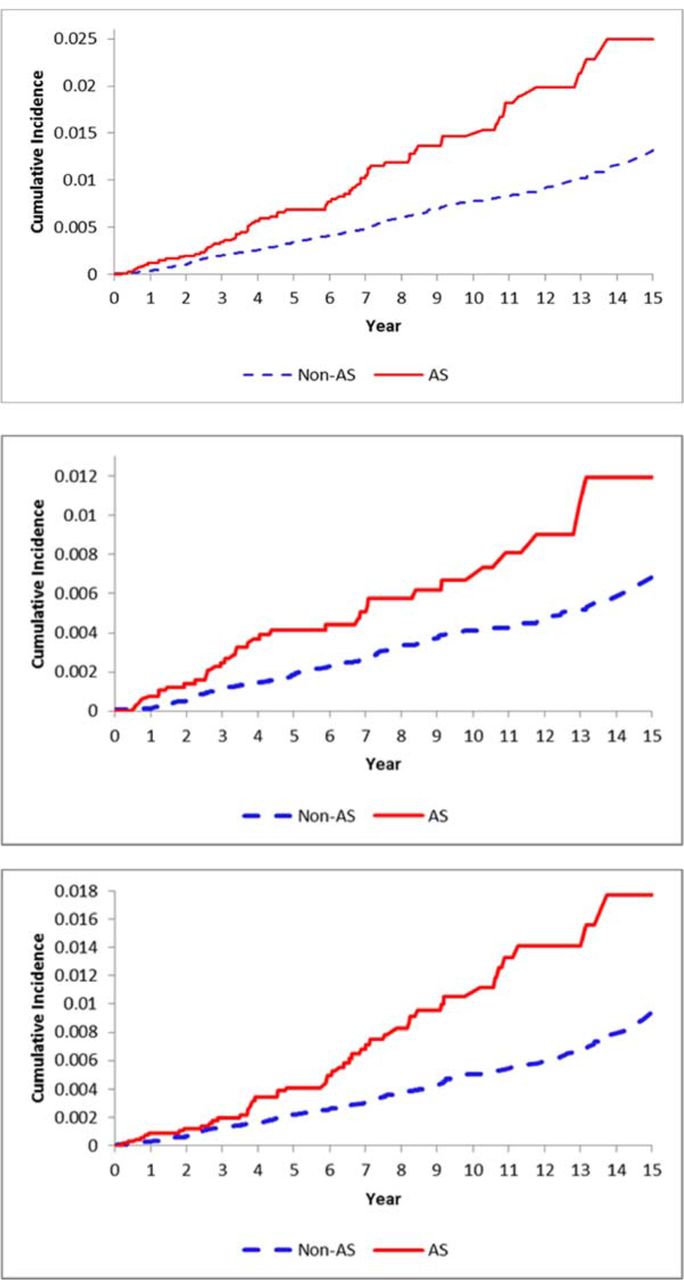
The IR per 1000 person-years was higher in the AS cohort for PE, DVT and VTE (0.79, 1.06, 1.56, respectively) compared with the comparison cohort (0.40, 0.50, 0.77, respectively) (table 2 and figure 1). The corresponding fully adjusted HRs for AS versus control were 1.36 (0.92 to 1.99), 1.62 (1.16 to 2.26) and 1.53 (1.16 to 2.01) for PE, DVT and VTE, respectively.
Relative risk of incident pulmonary embolism (PE) and deep venous thrombosis (DVT) according to ankylosing spondylitis (AS) status
{kind=link}
Cumulative incidence for venous thromboembolism (upper Panel), pulmonary embolism (middle Panel) and deep venous thrombosis (bottom Panel) in the 7190 cases with incident ankylosing spondylitis (AS) compared with the 71 900 age-matched, sex-matched and entry-time-matched non-AS subjects.
The adjusted risks of PE, DVT and VTE were highest in the first year after diagnosis with a greater than twofold increased risk, however, the CIs overall included one and therefore were not statistically significant (table 3). The relative risk (RR) appeared to remain relatively stable in subsequent years. When the total follow-up period was analysed, risks of DVT and VTE were significantly increased whereas risk of PE was not, with a fewer number of events than DVT.
Age-adjusted and sex-adjusted HRs for PE, DVT or both (VTE) in AS according to follow-up period
Sensitivity analysis
The HR for DVT and VTE remained significant when a simulated confounder with a 20% prevalence and OR of 1.3 was used but lost significance when the OR was increased to 3.0 (table 4). The HR for PE which has fewer event was only significant in the unadjusted results and the competing risk of death-Cox model.
Sensitivity analyses, HR (95% CI)
Primary analysis is the fully adjusted model; subdistribution models are adjusted for the same covariates as the primary analysis in addition to age and sex; simulated confounder models included additional covariates per the selection algorithm
Discussion
In this large population-based study, we have demonstrated that AS is associated with an increased risk of VTE. Though patients with AS had an increased prevalence of known risk factors of VTE, this effect remained significant even after adjustment for these baseline factors. Overall, there appeared to be a 50% increase in risk of VTE with a larger effect seen in DVT than in PE. After analysing this effect over time, there appeared to be a higher risk in the first year after diagnosis, although this stratification did not attain statistical significance.
An increased risk for VTE has been demonstrated in other inflammatory arthritis including psoriatic arthritis and rheumatoid arthritis with similar point estimates to ones observed in this current study.4–7 9 40 41 Furthermore, initiation of a biological disease-modifying antirheumatic drug (DMARD) seems to be associated with an increased short-term risk of VTE when compared with initiation of a non-biological DMARD.42 However, this has not been consistently demonstrated by others.43 Several previous studies have analysed the risk of VTE in AS with contrasting conclusions. A Chinese study assessed the risk of VTE in AS compared with OA patients undergoing total hip arthroplasty.44 Though the authors did not find a statistical significant difference, there were a number of issues with their study including a small sample size (n of AS cases=48) and an inappropriate control group with large differences in age, hypertension and body habitus between the two groups. Another study from Johannesdottir et al 20 used the Danish National Patient Registry to identify patients with autoimmune conditions among patients with a history of VTE. Similarly, they did not find a statistical difference after adjustment of classic VTE risk factors among patients with AS, due to their very small sample size of 20 patients with AS. Finally, Bengtsson et al used the Swedish National Patient registry to also demonstrate a 50% increased risk of VTE in patients with AS.21
Two previous inpatient studies of patients with AS drew similar conclusions to ours.18 19 A nationwide Swedish study18 19 found an over fourfold increase in VTE in the first year of follow-up although this risk lost statistical significance in subsequent years. The study by Ramagopalan et al 18 19 had also demonstrated an almost twofold increase in VTE overall. As both studies were drawn from hospital-based data, these results may not be generalisable to the entire AS population as hospitalised patients with AS may have more severe disease potentially resulting in a selection bias. As such, generalisability of these study findings to patients who do not require hospitalisation remained unclear. Our population-based study that included both outpatient and inpatient cases of AS was able to address this question and the risk estimates should be generalisable.
In our time-trend analyses on the risk of VTE, we found that the highest risk was on the first year after the AS diagnosis, however, our results did not achieve statistical significance due to the wide 95% CI. This suggests a possible power issue given that VTE is a rare outcome. An alternative explanation for the early increased risk of VTE in AS may be related to the reduced numbers of susceptible individuals over time or less likely a detection bias.
Virchow’s triad of hypercoagulability, endothelial dysfunction and venous stasis provides a framework for theoretical explanations of this increased risk. The chronic production of C reactive protein (CRP) and inflammatory cytokines such as tumour necrosis factor α and IL-6 may result in a hypercoagulable state.45 Additionally, some studies of patients with AS have demonstrated elevations in E-selectin, MCP-1 and (soluble vascular adhesion molecula-1 (sVCAM-1)46 suggesting possible endothelial dysfunction. Furthermore, there have been some conflicting data with regard to impaired endothelial function as measured by flow-mediated vasodilation, common carotid intima–media thickness and aortic pulse-wave velocity45 in patients with AS. Finally, many patients with AS have restricted mobility due to both pain from disease activity and the sequelae of previous inflammation resulting in spinal fusion. It seems apparent; however, that the relative risk of VTE in AS appears less severe than that observed in systemic lupus erythematosus (SLE), poly/dermatomyositis and systemic vasculitides.4–6 Additionally, as there is no ICD-9 or 10 code for non-radiographic axial spondyloarthritis, it is possible patients were misclassified as having AS rather than the broader term axial spondyloarthritis. This may explain the high female prevalence in our population.
Our study has a few limitations. Inherent to all observational studies is the risk of unidentified potential confounders. We adjusted for all known risk factors for VTE available in the data; however, some risk factors, such as body mass index and smoking history, were not available in the database. Additionally, non-steroidal antiinflammatory drugs (NSAIDs) are one of the mainstay of therapies for AS and over-the-counter use of these medications could not be accounted for. With any administrative database, there is a degree of uncertainty regarding the accuracy of ICD codes for AS. Previous studies assessing the diagnostic accuracy of ICD-9-CM billing codes compared with rheumatologist chart diagnosis demonstrated the use of one code for spondyloarthritis had a sensitivity of 91% and specificity of 99%.32 The diagnostic algorithm used in our study was more stringent requiring at least two codes for AS over a 2-year period or one code in addition to a hospitalisation for AS. However, it is possible that misclassification could still occur, but this would be a conservative bias where the observed effect would be biased towards the null hypothesis.
Our study has several strengths including the large dataset encompassing almost the entire population of BC. The vast majority of BC residents are covered through the public healthcare system resulting in comprehensive data with minimal loss of follow-up. Because these data include information from both inpatient and outpatient settings as well as primary care and specialist records, the entire spectrum of disease is likely to be captured allowing for generalisation to the AS population as a whole. Our use of a strict case definition for both incident AS and VTE enhances the accuracy of our findings. Furthermore, our administrative database includes detailed information on patients including medications, imaging investigations, cancer and other demographic data allowing us to adjust our analysis for multiple confounders.
In conclusion, we have reported an increased risk of VTE in AS in this general population-based study. These results expand on the findings of previous studies that implicate AS with vascular disease and add to the importance of controlling this inflammatory disease. Our results have important implications for people with AS and their treating physicians. These results call for awareness of this complication, increased vigilance and preventive intervention by controlling the inflammatory process or by anticoagulation in a high-risk AS population. Future investigation should clarify the relative contributions of treatment to the risks of PE and DVT in AS. Future studies should clarify if certain subsets of the AS population are at higher risk such as those with elevated CRP, bone marrow oedema on MRI or rapid radiographic progression of spinal fusion. These studies should also assess whether treatment of the inflammatory process can reduce the risk of VTE in AS.
References
Footnotes
Handling editor Josef S Smolen
Contributors JAA-Z (corresponding author) was responsible for applying and securing the funds for the project. He was also involved in the planning of the study design and statistical analysis, and he reviewed the study manuscript. He takes responsibility for the data and integrity of the paper. JC contributed to the project by taking part in the planning of the statistical analysis, as well as writing and compiling the study manuscript. MDV was involved in the planning of the study design and review of the study manuscript. ECS was the statistical analyst who carried out the analysis and reviewed the study manuscript. HC contributed to the fund application process and took part in the planning of the study design. He also reviewed the study manuscript. JE contributed to the fund application process and critically reviewed the manuscript.
Funding This study was funded by grants from the Canadian Arthritis Network, The Arthritis Society of Canada, the British Columbia Lupus Society (Grant 10-SRP-IJD-01) and the Canadian Institutes for Health Research (Grants MOP 125960 and THC 135235). JAA-Z is the British Columbia Lupus Research Scholar and holds a salary award from the Michael Smith Foundation for Health Research. MDV is a tier 2 Canada Research Chair in Medication Adherence, Utilization, and Outcomes and holds a salary award from the Michael Smith Foundation for Health Research.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethics approval was obtained from the University of British Columbia.
Provenance and peer review Not commissioned; externally peer reviewed.