Article Text

Abstract
Objectives Mortality in patients with rheumatoid arthritis (RA) is higher than in the general population. We investigated mortality in the COBRA-trial cohort after 23 years follow-up, compared with a reference sample of the Dutch population.
Methods The COBRA-trial randomised patients with early RA to sulfasalazine monotherapy (SSZ, n=79) or a combination of SSZ, low-dose methotrexate and initially high, step-down prednisolone (COBRA, n=76). We compared the mortality in the COBRA-trial up to 2017 to a reference sample of the general population in the Netherlands (standardised mortality ratio, SMR), and its relation to early prognostic factors through stepwise Cox regression.
Results Duration of follow-up in patients alive was mean 23 (range 22–24) years. In total, 44 patients died (28%, SMR=0.80 [95% CI 0.59 to 1.06]); 20 of 75 COBRA patients (27%, SMR 0.75 [0.47 to 1.14]) and 24 of 79 SSZ patients (30%, SMR 0.85 [0.56 to 1.25]); p=0.61). In the reference sample of the general population, 55 people (36%) died. 5 factors were significantly associated with increased mortality hazard: damage progression at 28 weeks; high Health Assessment Questionnaire (HAQ) score and absence of HLA-DR 2 or 3; disease duration from start of complaints was also significant, but showed an uninterpretable pattern.
Conclusions This prospective trial cohort study of early RA is one of the first to show similar mortality compared with the general population after 23 years of follow-up. It confirms that early, intensive treatment of RA has long-term benefits and suggests that treating to target is especially important for patients with poor prognosis.
- early rheumatoid arthritis
- epidemiology
- corticosteroids
- dmards (synthetic)
- outcomes research
- arthritis
- rheumatoid
- epidemiology
- mortality
- randomized clinical trial
Statistics from Altmetric.com
- early rheumatoid arthritis
- epidemiology
- corticosteroids
- dmards (synthetic)
- outcomes research
- arthritis
- rheumatoid
- epidemiology
- mortality
- randomized clinical trial
Key messages
What is already known about this subject?
Mortality in patients with rheumatoid arthritis (RA) is higher than that of the general population, especially in patients with disease duration >10 years.
What does this study add?
This prospective cohort study in patients with early RA is one of the first to show a normalisation of RA mortality after 23 years of follow-up.
Several well-known prognostic factors were related to mortality.
How might this impact on clinical practice or future developments?
The study confirms that early and intensive treatment of RA has long-term benefits and suggests that treating to target is especially important for patients with poor prognosis.
Introduction
Mortality in patients with rheumatoid arthritis (RA) is higher than that of the general population.1 In recent studies, the adverse effect of RA appears to have decreased, but in some there is an indication that long follow-up (>10 years) is necessary for the full adverse effect to become apparent.2 3 Whether early and intensive treatment can improve this mortality is still uncertain.
The COBRA (Combinatietherapie bij Reumatoide Artritis) multicentre, double-blind randomised trial compared the combination of sulfasalazine (SSZ), methotrexate (MTX) and prednisolone (COBRA) to SSZ monotherapy. COBRA combination therapy was superior to SSZ in disease control (activity and damage) with less adverse events.4 Subsequently, patients in the COBRA study arm retained better disease control in the 5 years following the trial independent of subsequent therapy;5 after 11 years, these patients had a numerically lower mortality and similar prevalence of comorbidity compared with patients originally in the SSZ arm.6
The present study extends mortality follow-up in this COBRA trial cohort to 23 years and explores associations between mortality and well-known prognostic factors.
Methods
The COBRA double-blind clinical trial ran between 1993 and 1995. A total of 155 patients with early and mostly DMARD naïve RA (disease duration median 4 months, maximum 2 years; 22% prior treatment with antimalarials) were randomly allocated: 76 patients received COBRA combination therapy and 79 patients SSZ monotherapy. COBRA combination therapy comprised SSZ (2 g/day), MTX (7.5 mg/week) and prednisolone (60 mg in the first week tapered to 7.5 mg in week 7). Prednisolone was withdrawn after 28 weeks, MTX after 40 weeks. Patients in the active control group received SSZ (2 g/day) and double placebos.
In addition, all patients received folic acid (1 mg/day), calcium (500 mg/day) and if necessary 25-hydroxyvitamin D (400 IU/day). Patients who experienced a flare started treatment with the drug that was most recently withdrawn. After study completion at 56 weeks, further treatment decisions were at the discretion of the treating rheumatologist, but physicians were asked not to (re)start prednisolone or MTX for another 6 months to prevent unblinding. All patients gave written informed consent for the study including follow-up.
In 2017, we retrieved mortality data of the COBRA cohort through scrutiny of the centralised Dutch mortality register of the Centrum of Familiegeschiedenis (CBG); where necessary, we contacted the rheumatologist for missing data.
We compared the mortality in the cohorts to each other and to a hypothetical reference sample of the general population in the Netherlands matched for age, gender and calendar period of start of follow-up. In more detail, to form the reference sample, we created a hypothetical ‘non-RA twin’ for each trial participant, that is, a person of the same sex and age. We then applied the Dutch population level yearly actuarial death rates to this sample until the end of study follow-up . Statistics Netherlands (Centraal Bureau voor Statistiek) provided these rates for the years 1994 to 2016. Finally, we calculated the standardised mortality ratio (SMR): observed deaths divided by the expected deaths in 2017. SPSS for Mac V.24.0 (SPSS, Chicago, Illinois, USA) performed the statistical analyses.
To compare our results with that of recent literature, we first performed a scoping search on Pubmed for systematic reviews with various combinations of the keywords: arthritis; rheumatoid; epidemiology and mortality (online supplementary appendix 1). We found two dated 20131 and 2016.7 Then, we searched for full size publications published in or after 2010 (the closing year of the first review) with these same keywords and found 532 hits. From these, we selected the seven articles that compared mortality of inception cohorts of patients with RA to that of the general population and a follow-up exceeding 10 years. From the literature lists of the selected articles, we found two additional abstracts (no new full-size articles). We contacted the authors but full-size publications were not yet available.
Supplemental material
We performed exploratory stepwise forward and backward Cox regression with the following variables as possible hazards: smoking, education level, disease duration defined from start of complaints, from first clinic visit and from diagnosis; disease activity score (DAS-44 joints); functional disability (Health assessment questionnaire); rheumatoid factor; Sharp van der Heijde damage score; rheumatoid factor (anti-citrullinated protein antibody (ACPA) not available at that time); presence of HLA-DR1, 2, 3 or 4; treatment group; change in DAS44 at 16 weeks; change in damage score at 28 and at 56 weeks. We also explored models that included only baseline data, only routine baseline data (ie, excluding HLA-DR) or only routine baseline and follow-up data.
To study representativeness of the trial cohort, we retrieved an unpublished analysis performed in Maastricht (one of the including centres) before publication of the main results. In this analysis, we checked the screening log of 1051 consecutive patients seen in the rheumatology outpatient department while the trial was running. The screening was applied to all patients visiting the clinic and set up to quickly rule out ineligible patients, so the form only needed to be completed until the first exclusion criterion was met. The exclusion sequence was: (1) no RA; (2) age; (3) prior treatment; (4) disease duration; (5) severe comorbidity; (6) American College of Rheumatology (ACR) criteria; (7) inactive disease.
Results
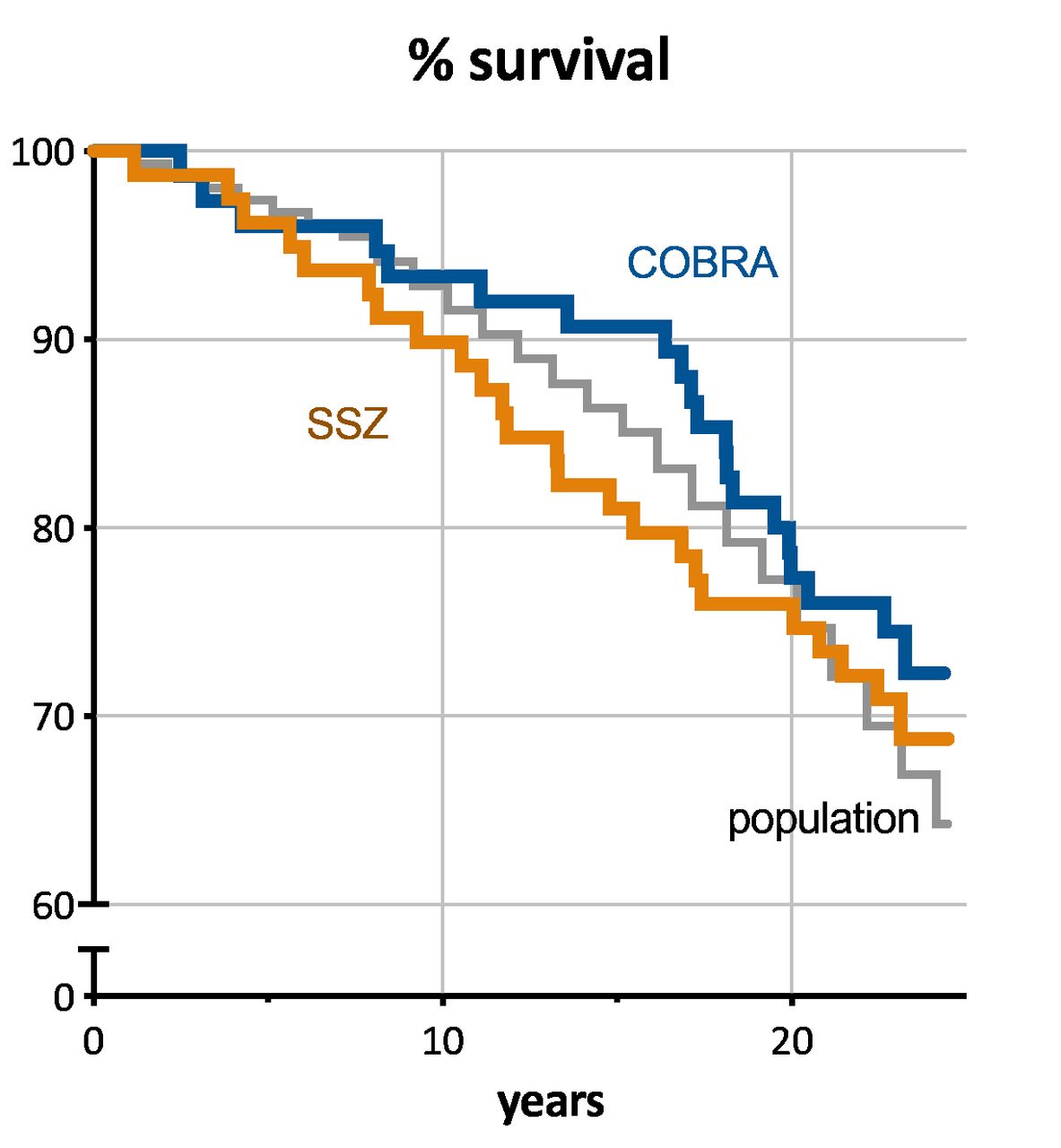
Follow-up was nearly complete with only 1 out of the 155 patients missing (from the COBRA group); this patient was already missing in earlier reports. Mean follow-up in patients alive was 23 (range 22–24) years. In total, 44 patients (28%, SMR=0.80 [95% CI 0.59 to 1.06]) of the cohort died during follow-up; 20 of the 75 patients of the COBRA-group (27%, SMR 0.75; [0.47 to 1.14]) and 24 out of 79 in the SSZ-group (30%, SMR 0.85 [0.56 to 1.25]). The difference in mortality was not significant (p=0.61). In the reference sample of the general population, 55 of 154 persons (36%) died. The mortality rates for COBRA over SSZ moved closer together over time (figure 1).
{kind=link}
Survival curves of the COBRA trial cohort by treatment. COBRA, n=75 (1 patient missing); SSZ, n=79. Survival of the reference cohort from the general population in grey. Note that all living patients have now been followed for 22–24 years, so the proportion of survivors equals the proportion at risk.
In exploratory stepwise forward Cox regression, five factors were significantly associated with increased mortality hazard: damage progression at 28 weeks; high HAQ score; shorter disease duration from start of complaints and absence of HLA-DR 2 or 3 (online supplementary appendix 1). The same factors were selected in backward stepwise regression (data not shown). In the models restricted to baseline variables, only the presence of HLA-DR1 or 4 was associated with an increased hazard; when only routine baseline variables were offered, none were associated with increased hazard.
In the models restricted to routine and follow-up data, shorter disease duration from start of complaints and damage progression at 28 weeks were associated with an increased mortality hazard (data not shown).
Plots of survival curves of subgroups split at the median or binary value of each factor showed results consistent with the regression results except for disease duration (online supplementary appendix 2). Survival risk did not consistently decrease with increasing duration, making the results for this factor difficult to interpret.
Supplemental material
Examination of the screening log of over 1000 patients visiting the outpatient clinic revealed that most were excluded for the following, sequentially applied criteria: no RA (39%), age (23%), prior treatment (17%) and disease duration (7%). Only 25 patients (2.4% of all patients and 3.9% of patients with RA) were excluded for serious comorbidity.
Discussion
This 23-year follow-up study shows normal mortality of the COBRA early RA trial cohort compared with that of the general population of the Netherlands. In fact, it is numerically lower than the reference cohort, with a CI still compatible with a 6% increase. The difference between the original trial groups was not significant. Compared with previous studies with follow-up exceeding 10 years, our results are the first to suggest that early treatment of RA may actually normalise mortality.
The exploratory Cox regression revealed interesting results: the impact of some, but not all traditional prognostic factors was confirmed. Of interest is also the number of factors showing statistical significance in this small sample size, and the strong effect of early damage progression, in the absence of an effect of baseline damage in this early RA cohort. These results must be seen in the light of the characteristics of early RA in the period 1993–1995, including high baseline damage and still substantial progression of damage; caution is also advised in view of the small sample size, and the fact that the overall survival curve suggests the constant hazard assumption may not be met. Nevertheless, the data suggest that it is worthwhile to intensively monitor patients with RA with poor prognostic indicators (high initial HAQ, rapid development of radiographic damage) and to strictly apply ‘treat to target’ goals.
A recent meta-analysis by Dadoun et al 1 covering the last 50 years showed that mortality in patients with RA remains higher than that of the general population, although the difference has decreased over the past decades. Minichiello et al 7 reviewed the literature with a focus on severity of RA and noted more improvement on life impact than on mortality.
We updated the existing systematic reviews by studying new published literature in or after 2010 and we see similar results as presented by the systematic reviews (table 1). In the largest study, Holmqvist et al 2 documented the mortality of RA in four different inception cohorts from 1997 onwards, covering over 80% of the Swedish population. Compared with the general population, they noted a decreased mortality rate in the first years, followed by increased rates after about 8 years of RA. The mortality increase of the cohort starting between 1997 and 2001 was somewhat lower (HR 1.09) compared with that seen in other, smaller RA studies (SMR/HR 1.23–1.66; table 1). In those studies, the increase in mortality was not always statistically significant.
Overview of recent studies on RA mortality in inception cohorts with more than 10 years of follow-up, and one recent systematic review*
We also found improvement of the increased mortality in several recent studies (ie, more recent than the Dadoun review) with a shorter follow-up.8–14 Radovits et al 3 and Abasolo et al 9 deserve separate mention: although the mean follow-up was less than 10 years, the range was wide and extended to 20 years or more. The former study reported an increased mortality risk only after 10 years of follow-up, whereas in the latter the increased risk was immediately apparent.3
Finally, Kiadaliri et al 15 had a different study focus that supports the above evidence: they studied the extreme of the distribution of RA-associated mortality, that is, cases where RA was reported as cause of death. They compared rates over time in 31 countries in databases of the WHO and the United Nations, and noted a decline overall, but with large disparities between countries.15
Altogether it appears that in the long term the increase in longevity seen in the general population is matched and perhaps surpassed by increases seen in the RA population, but a detrimental difference remains. It is likely that the improved prognosis is the sum of earlier detection and treatment, more aggressive treatment, and better handling of (especially cardiovascular) comorbidity. Differences between studies can be attributed to differences in study population (incidence or prevalence cohorts; trial or clinic; geographical location, management and follow-up duration). Our study represents a favourable extreme, showing normalisation of mortality in an inception trial cohort. Importantly, it confirms our earlier findings suggesting that initial treatment of RA with glucocorticoids does not lead to an excess of harm.
Strengths of our study include initially tightly protocolled treatment and a nearly complete follow-up that spans 23 years. Weaknesses include the lack of power due to the small sample size and lack of data on treatments and cause of death. However, our previous follow-up study already documented a pattern of comorbidity comparable to the general population, without differences in treatment or comorbidity between the treatment groups.6 In addition, recorded causes of death are notoriously unreliable when compared with autopsy results.16 Also, the peculiarities of a trial cohort hinder generalisability: the patients were selected for active RA disease and had several unfavourable prognostic characteristics related to RA (bad RA, worse prognosis than the patient with average RA) but were also selected for lack of severe comorbidity and perhaps other generally favourable factors associated with trial participation (better health, better prognosis than the general population). However, examination of a large screening log suggests that comorbidity was not an important reason for exclusion.
In conclusion, this is the first study with follow-up of more than 20 years that strongly suggests normal mortality of patients with RA in a trial cohort, and no difference between patients initially treated with a combination of conventional disease modifying drugs (including glucocorticoids) or SSZ monotherapy right from the start of the disease.
Acknowledgments
Reinier de Graaf Gasthuis, Delft, the Netherlands: A J Peeters; Centrum voor familiegeschiedenis, the Netherlands: J Hartman; Medisch Spectrum Twente, the Netherlands: M Van de Laar, H Moens; Leiden University Medical Center, Leiden, The Netherlands: C F Allaart; Maasstad Ziekenhuis, Rotterdam: H Han; Laurentius Ziekehuis, Roermond, The Netherlands: L Heuft; Ziekenhuis Saexneburgh Groep, the Netherlands; C E I Lebrun; Maastricht University Medical Center, Maastricht, the Netherlands: A Boonen.
References
Footnotes
Handling editor Josef S Smolen
Presented at This paper was presented in plenary session at EULAR 2018.
Contributors All authors contributed to design, collection of data, analysis and reporting.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data is available for sharing upon request.