Article Text

Abstract
Objectives To compare the clinical manifestations, disease activity and disease burden between patients with radiographic (r-axSpA) and non-radiographic axial spondyloarthritis (nr-axSpA) over a 5-year follow-up period in the Devenir des Spondylarthropathies Indifferénciées Récentes (DESIR) cohort.
Methods Patients from the DESIR cohort who had X-ray images of the sacroiliac joints available at baseline and did not leave the study during the 5-year follow-up period because of a diagnosis other than axSpA were included. A unilateral rating of ‘obvious sacroiliitis’ by the local reader was considered sufficient for classification as r-axSpA. The incidence of first episodes of peripheral and extra-rheumatic manifestations was compared between the two groups using the incidence rate ratio and Cox regressions adjusted for sex, age and tumour necrosis factor blocker (TNFb) intake. Mean values of patient-reported outcomes (PROs) and days of sick leave over 5 years of follow-up were compared using mixed models adjusted for sex, age, TNFb intake and baseline values.
Results In total, 669 patients were included, of whom 185 (27.7%) and 484 (72.3%) were classified as r-axSpA and nr-axSpA, respectively. At baseline, the r-axSpA patients showed a significantly higher prevalence of males. After adjusting for age, sex and TNFb intake, Cox regressions for peripheral and extra-rheumatic manifestations did not show any significant differences between groups. Mixed models also showed similar mean levels in PROs and days of sick leave between groups over time.
Conclusion The incidence of peripheral and extra-rheumatic manifestations as well as the disease burden over time remained similar between r-axSpA and nr-axSpA groups after adjusting for intermediate variables.
Trial registration number NCT01648907
- axial spondyloarthritis
- peripheral manifestations
- patient-reported outcomes
Statistics from Altmetric.com
Key messages
What is already known about this subject?
A debate exists concerning the concept of non-radiographic axial spondyloarthritis (nr-axSpA): some people suggest that patients with nr-axSpA might actually be suffering from a disease different from radiographic axSpA (r-axSpA), while others consider that nr-axSpA could be a self-limited form of axSpA with a rapidly favourable course or an early stage of the same spectrum.
What does this study add?
This study suggests that both r-axSpA and nr-axSpA behave similarly over time since the incidence of peripheral and extra-rheumatic manifestations as well as the disease burden are not different after 5 years of follow-up.
How might this impact on clinical practice or future developments?
These results confirm the concept of axSpA as one single disease, which implies that both r-axSpA and nr-axSpA patients should be treated with equal priority. For this reason, the distinction between r-axSpA and nr-axSpA should only have implications for clinical research and not for clinical practice.
Introduction
Axial spondyloarthritis (axSpA) is a chronic inflammatory rheumatic disease that encompasses patients with radiographic axSpA (r-axSpA; also known as ankylosing spondylitis—AS, with advanced structural damage on X-ray) and non-radiographic axSpA (nr-axSpA; no definitive signs of structural damage on X-ray).1 The fact that only 5.1% of patients with recent axSpA shifts from nr-axSpA to r-axSpA over 5 years2 prompts a debate concerning the concept of nr-axSpA: some people suggest that patients classified as nr-axSpA might actually be suffering from a disease different from r-axSpA, while others suggest that nr-axSpA could be a self-limited form of axSpA with a rapidly favourable course. This debate is particularly important in North America, where the Food and Drug Administration expressed several concerns about the incompletely characterisation of the natural history of axSpA, which led to the non-approval of several biological disease-modifying antirheumatic drugs (bDMARDs) to treat patients with nr-axSpA.3 These questions resulted in the publication of some studies that compare these two groups of patients, showing a similar disease burden but a higher prevalence of males and smokers, a larger mean disease duration and a higher level of acute phase reactants in r-axSpA patients.4–8 However, most of these studies have a cross-sectional design which does not allow us to understand the natural history of these two subgroups. Only a few studies have evaluated the course of the disease with a longitudinal and prospective approach, but most of them focused on radiographic progression and/or the effectiveness of bDMARDs as the main outcome.9–12 In 2015, two independent studies that compared the clinical course (ie, patient-reported outcomes (PROs) and acute phase reactants) of r-axSpA and nr-axSpA were published: the first study reported no between-group differences in pain and quality of life over 3 years, while mean C reactive protein (CRP) levels remained higher in the r-axSpA group13; the second study reported a similar disease activity (measured with the Bath AS Disease Activity Index—BASDAI) and functional status (measured with the Bath AS Function Index—BASFI) in both groups, but higher mean CRP levels in r-axSpA patients after a 2-year follow-up.14 However, none of these studies compared the incidence of peripheral and extra-rheumatic manifestations between groups.
DESIR (Devenir des Spondylarthropathies Indifferénciées Récentes) is a prospective cohort of patients with recent onset axSpA. We conducted this study with the aim of comparing the clinical manifestations and disease burden between r-axSpA and nr-axSpA patients over 5 years of follow-up. By estimating the risk of extra-spinal manifestations, we planned to determine whether nr-axSpA can be considered as the same disease as r-axSpA. By estimating the level of activity/severity over time, we intended to explore whether nr-axSpA can be considered as a self-limited disease.
Methods
Patients
For this analysis, 5-year follow-up data from the DESIR cohort were used. Patients who had X-ray images of the sacroiliac joints (SIJ) available at baseline were included. The DESIR cohort has been previously described.15 Briefly, consecutive patients aged 18–50 years from 25 centres in France who had inflammatory back pain (evaluated by either the Calin or the Berlin criteria)16 17 that lasted ≥3 months but <3 years were included if the treating rheumatologist considered the symptoms suggestive of axSpA (a score ≥5 on a scale from 0 to 10). Moreover, we excluded patients who had a different diagnosis than that of axSpA after at least 2 years of follow-up according to the treating rheumatologist. Visits were scheduled every 6 months during the first 2 years and yearly thereafter.
The study was conducted according to good clinical practice guidelines and was approved by the appropriate local medical ethical committees.
Patient and public involvement
Patients were not involved in the design of the study, conduct of the study, development or dissemination of study results.
Definitions of r-axSpA and nr-axSpA
Pelvic radiographs collected at baseline were used to define r-axSpA and nr-axSpA. Local radiologists or rheumatologists read all available baseline radiographs of the SIJ in their own centre, hereafter called ‘local reading’. Local readers were asked to rate each SIJ as either ‘normal’, ‘doubtful sacroiliitis’, ‘obvious sacroiliitis’ or ‘SIJ fusion’.18 According to this scoring method, a unilateral rating of ‘obvious sacroiliitis’ was considered sufficient for the classification as r-axSpA in this study, while the remaining patients were classified as nr-axSpA. We used this scoring system because it more closely resembles common clinical practice than does the modified New York (mNY) criteria and because it has been used in previous studies.19
Moreover, a sensitivity analysis was performed using the results from the central readings. Baseline radiographs of the SIJ were read independently by three trained readers. Each reader evaluated each SIJ according to the mNY grading method (ie, at least a unilateral grade 3 sacroiliitis or at least a bilateral grade 2 sacroiliitis). A radiograph of the SIJ was considered positive for sacroiliitis if two of the three central readers agreed on fulfilment of the mNY criteria, and hereafter referred to as ‘central reading’.
Collected data
Baseline information about sociodemographics, smoking status, alcohol, HLA-B27, axial symptom duration, good non-steroidal anti-inflammatory drugs (NSAIDs) response, Assessment of Spondyloarthritis International Society (ASAS) axial, European Spondylarthropathy Study Group (ESSG) and AMOR criteria fulfilment were used.20 21
At baseline and during the follow-up (at 0, 6, 12, 18, 24, 36, 48 and 60 months), the following data were analysed: peripheral arthritis (either detected via physical examination or considering patients who reported having received intra-articular corticosteroids between visits), dactylitis, enthesitis at any location, uveitis, psoriasis, inflammatory bowel disease (IBD), CRP, Ankylosing Spondylitis Disease Activity Score (ASDAS-CRP), SpondyloArthritis Research Consortium of Canada (SPARCC) score on the SIJ,22 BASDAI, BASFI, SF-36 questionnaire23 and days of sick leave. Treatment intake, including NSAIDs by the ASAS-NSAID score,24 conventional synthetic disease modifying antirheumatic drugs (csDMARDs) and TNFb were also analysed.
Statistical analysis
Baseline characteristics
Baseline clinical characteristics of patients with and without at least unilateral ‘obvious sacroiliitis’ according to the local reading were compared using χ2 and t-test (or Fisher and Mann-Whitney U test for non-parametric data). In order to confirm that differences across r-axSpA and nr-axSpA were similar regardless the use of local and central reading, the same analysis was conducted using the central reading definition (ie, fulfilment of mNY criteria according to two of the three central readers).
Peripheral and extra-rheumatic manifestations over 5 years of follow-up
Three types of statistical models were conducted to compare peripheral and extra-rheumatic manifestations between r-axSpA and nr-axSpA: (1) a cross-sectional model at baseline; (2) a pseudo-longitudinal model, in which the prevalence of these manifestations at 5-year time-point as well as the incidence rate ratio (IRR) between the r-axSpA and nr-axSpA groups were compared; (3) a longitudinal model (Cox regressions) in which data from intermediate visits was used to compare the time-to-event of these manifestations (firstly as a crude analysis and thereafter adjusted by age, gender and TNFb intake over follow-up) between both groups.
csDMARDs and TNFb initiation over 5 years of follow-up
The same three analysis as that used for peripheral and extra-rheumatic manifestations were conducted for csDMARDs and TNFb initiation.
Disease activity, PROs and days of sick leave over 5 years of follow-up
Disease activity (CRP and SPARCC-SIJ), PROs and days of sick leave over the 5 years of follow-up were compared between the r-axSpA and nr-axSpA using a crude mixed model with random effects (here, the subject was considered a random effect and the absence of ‘obvious sacroiliitis’ based on the local reading a fixed effect) and also adjusting for baseline values, age, sex and time-changing variables (TNFb use).
Exploratory analysis of the variables influencing disease activity over time
In order to determine which variables had an impact on the disease activity over the 5 years of follow-up, a multivariate linear regression was performed to determine the different factors that may explain the change in mean BASDAI and ASDAS-CRP over time.
Handling of missing data
For the cross-sectional analysis, baseline missing data were not imputed. For the IRR analysis, the last observation carried forward (LOCF) method was used (ie, a patient with at least one episode in the follow-up was considered positive at the end of the study). For the longitudinal analysis, LOCF was used for Cox models, while continuous variables were imputed via the use of mixed models.
Results
Of the 708 patients included in the DESIR cohort, a total of 25 patients were excluded for this analysis because they had a different diagnosis other than axSpA after at least 2 years of follow-up (figure 1). Among the remaining 683 patients, 669 and 659 had local and central X-ray reading data available, respectively.
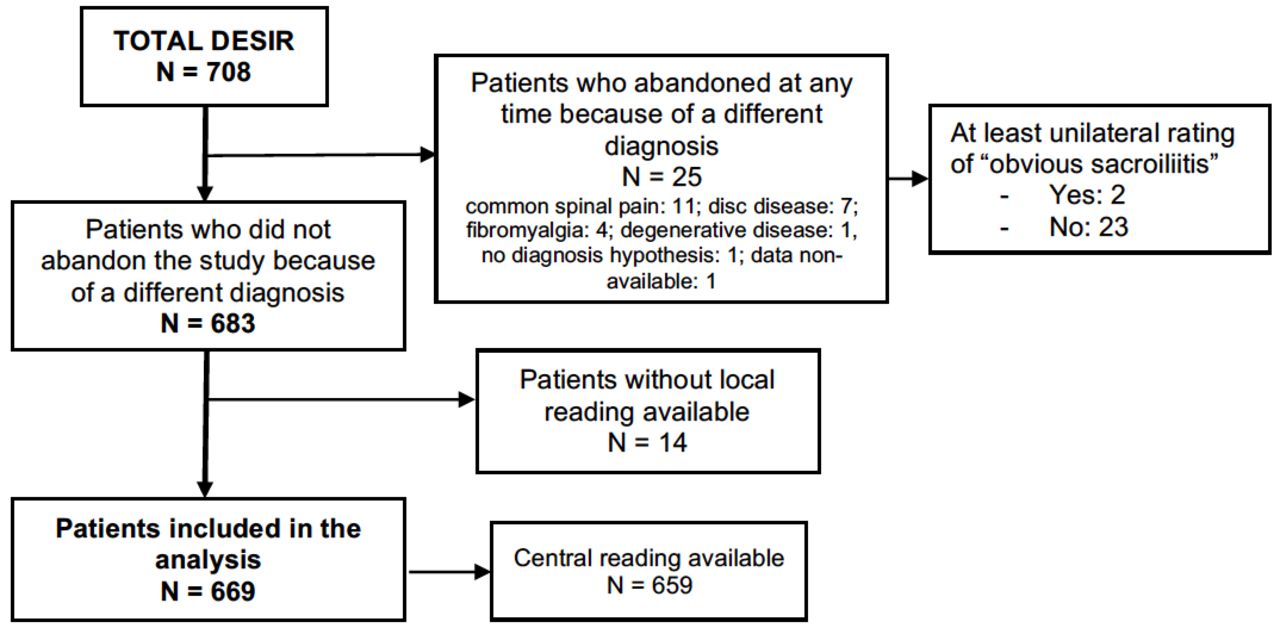
Flow-chart with regard to the patients included in the analysis. DESIR, Devenir des Spondylarthropathies Indifferénciées Récentes.
Among the 669 patients evaluated by local readers, 185 (27.7%) had at least a unilateral rating of ‘obvious sacroiliitis’, and 484 (72.3%) were classified as either ‘normal’ or ‘doubtful sacroiliitis’. Of the 659 patients with central reading data available, 92 (14.0%) fulfilled the mNY criteria according to two of the three central readers, and 567 (86.0%) did not fulfil the mNY classification criteria.
Baseline characteristics
Baseline characteristics and differences between r-axSpA and nr-axSpA patients according to the local reading definition are shown in table 1. A sensitivity analysis was performed using the mNY classification from the central reading (online supplementary table S1) showing similar results.
Supplemental material
Baseline characteristics of the 669 patients with local X-ray reading available
Peripheral and extra-rheumatic manifestations over 5 years of follow-up
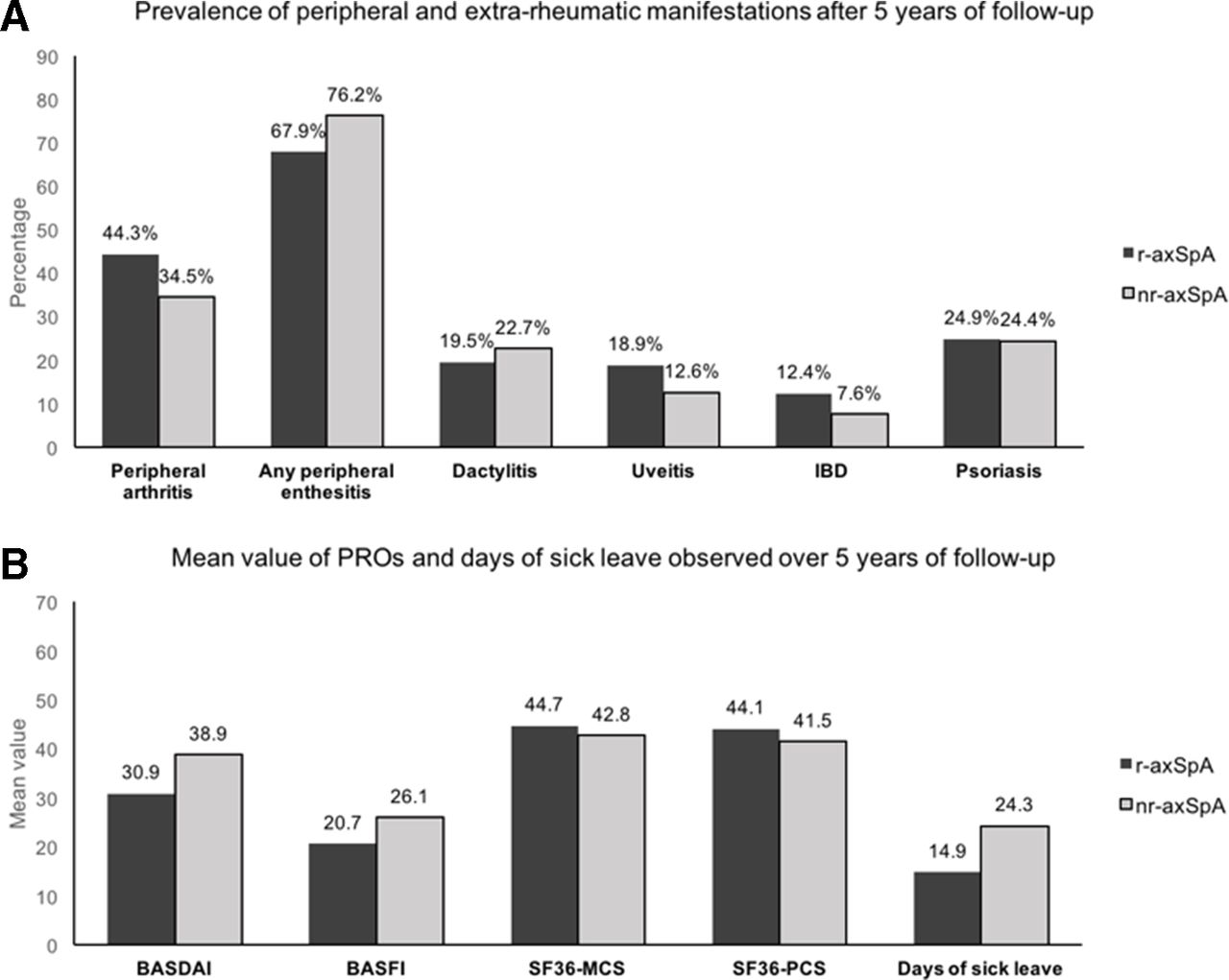
Using r-axSpA and nr-axSpA definition from the local reading, we compared the prevalence of peripheral and extra-rheumatic manifestations at baseline and after 5 years follow-up between the two groups, as well as the IRR by excluding patients who had a positive event at baseline (table 2). At baseline, r-axSpA patients showed a significantly lower prevalence of ‘ever’ peripheral enthesitis than nr-axSpA patients, while the prevalence of ‘ever’ peripheral arthritis, dactylitis and extra-rheumatic manifestations were similar between the two groups. Overall, all peripheral and extra-rheumatic manifestations showed a higher prevalence in the whole population after 5 years (figure 2).

{kind=link}
{kind=link}
Main outcomes after 5 years of follow-up. BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; BASFI, Bath Ankylosing Spondylitis Function Index; IBD, inflammatory bowel disease; PRO, patient-reported outcome; SF36-MCS, Mental Component Score from the SF-36 questionnaire; SF36-PCS, Physical Component Score from the SF-36 questionnaire; nr-axSpA, non-radiographic axial spondyloarthritis; r-axSpA, radiographic axial spondyloarthritis.
Prevalence and incidence of peripheral and extra-rheumatic manifestations, as well as treatment initiation
The incidence of first episodes of peripheral arthritis was higher in r-axSpA than in nr-in axSpA patients, with a significant IRR of 1.75 (95% CI 1.14 to 2.67) for r-axSpA versus nr-axSpA. Uveitis, IBD and psoriasis also showed a higher incidence of first episodes in r-axSpA, while peripheral enthesitis and dactylitis were more incident among nr-axSpA patients, although these differences were not significant.
Cox regressions comparing the incidence of peripheral and extra-rheumatic manifestations over time are shown in table 3. R-axSpA patients showed a significantly higher risk for the development of peripheral arthritis than nr-axSpA (crude HR 1.73, 95% CI 11.13 to 2.64), but these differences were no longer significant after adjusting for age, sex and TNFb intake. Similarly, peripheral enthesitis, dactylitis and extra-rheumatic manifestations did not show any differences after both adjusting and not adjusting for intermediate variables, reflecting a similar risk of appearance of these manifestations between r-axSpA and nr-axSpA patients.
Cox regressions to compare the incidence of peripheral and extra-rheumatic manifestations over 5 years of follow-up between r-axSpA and nr-axSpA
csDMARDs and TNFb initiation over 5 years of follow-up
Regarding TNFb (table 2), at baseline per protocol, not a single patient had been exposed to or was receiving TNFb, while 252 initiated TNFb after 5 years of follow-up, with significant differences between r-axSpA and nr-axSpA groups. The incidence of TNFb initiation was also different between r-axSpA and nr-axSpA (IRR 1.59, 95% CI 1.23 to 2.07).
The prevalence of patients under csDMARDs at baseline and after 5 years was similar between the r-axSpA and nr-axSpA groups.
Cox regressions (online supplementary table S2) showed a significantly higher risk of TNFb initiation among r-axSpA patients after adjusting for sex, age and CRP mean levels.
Disease activity, PROs and days of sick leave over 5 years of follow-up
Table 4 shows the results of the mixed model with random effects for disease activity variables, PROs and days of sick leave. Mean CRP over time was significantly higher among r-axSpA patients, even after adjusting for intermediate variables. MRI-SIJ inflammation evaluated with SPARCC was higher among the r-axSpA than among nr-axSpA group, but these differences disappeared after adjusting for intermediate variables.
Mixed models with random effects to compare disease activity, PROs and days of sick leave over 5 years of follow-up between r-axSpA and nr-axSpA
Compared with r-axSpA, nr-axSpA patients showed significantly higher levels of BASDAI and BASFI, poorer scores in the SF-36 questionnaire and a larger number of days of sick leave over time. However, these differences disappeared after adjusting for intermediate variables.
Exploratory analysis of the variables influencing disease activity over time
Finally, multivariate linear regressions (online supplementary tables S3 and S4) showed that the variability of BASDAI over the 5 years was explained by age, sex, level of education, radiographic sacroiliitis, TNFb and mean CRP, while ASDAS-CRP was explained by sex, level of education and TNFb.
Discussion
This study permitted to evaluate the natural history of patients with recent IBP classified as r-axSpA or nr-axSpA in daily clinical practice.
In the DESIR cohort, the probability of observing structural damage on the SIJ (at least unilateral rating of ‘obvious sacroiliitis’) in patients with recent IBP suspicious of axSpA was 27.6%, while the probability of observing patients fulfilling the mNY criteria was 14.0%. We decided to use the ‘local reading’ scoring system because it closely reflects the procedure in clinical practice; that is, even if a patient does not fulfil the mNY criteria, a rheumatologist or radiologist usually classifies the patient as r-axSpA if he/she has obvious unilateral structural damage.
At baseline, the results showed similarities between patients with r-axSpA and nr-axSpA (especially in extra-rheumatic manifestations and disease burden) with some differences mainly in relation to the clinical presentation and inflammation. A larger number of r-axSpA patients were smoking males and had higher CRP and SPARCC levels compared with nr-axSpA patients. These characteristics have been classically described as risk factors for structural damage in the SIJ and the spine,25 which lead to a higher probability of TNF initiation. In fact, in this study we demonstrated that inflammation measured with CRP was permanently higher among r-axSpA despite the greater use of TNFb in this group; however, this can be partly explained because 31% of r-axSpA patients in the DESIR cohort did not received a TNFb treatment despite a high disease activity over 5 years of follow-up.26 HLA-B27 positivity and alcohol intake were also more frequent among nr-axSpA, being these results consistent with previous studies in the DESIR cohort.2 19 We also found a higher prevalence of heel enthesitis and other peripheral enthesitis among the nr-axSpA group at baseline. However, these peripheral manifestations might be artificially overrepresented among nr-axSpA patients because they help to diagnose nr-axSpA in the absence of radiographic sacroiliitis.
In this study we aimed to evaluate the incidence of first episodes of peripheral and extra-rheumatic manifestations between the two groups after diagnosis. For this reason, in the longitudinal analysis (ie, IRR and Cox regressions), we decided to remove patients with a positive event at baseline to avoid the bias caused by the prevalence at the inclusion visit. Although the nr-axSpA group showed a higher prevalence of peripheral enthesitis at baseline, the incidence was similar between groups after the exclusion of patients with a positive event at the inclusion visit, confirming the theory that peripheral manifestations might be overestimated among nr-axSpA patients at the time of diagnosis. The incidence of dactylitis and extra-rheumatic manifestations were also similar, demonstrating a clinical pattern that is comparable between these two groups with regard to these manifestations. These data suggest that axSpA should be considered a single disease entity.
Because r-axSpA patients showed higher CRP levels over time, we expected to find a greater disease burden in this group. Curiously, and contrary to our expectations, nr-axSpA patients presented higher scores in the BASDAI and BASFI, a poorer quality of life and a larger number of days of sick leave at the follow-up. We have two theories that can explain these results. One theory is that a percentage of nr-axSpA patients may have concomitant fibromyalgia, as this phenomenon has been described in a study published by Moltó et al: patients without radiographic sacroiliitis more frequently had concomitant fibromyalgia according to the American College of Rheumatology (ACR) 1990 criteria than did r-axSpA patients.27 The second hypothesis is that other factors and patient characteristics influence disease activity and disease burden. Thus, we adjusted the mixed models using variables that might lead to the higher scores observed among nr-axSpA group (ie, age, sex and TNFb use). The rationale to adjust for these variables was based on the fact that they were, a priori, clinically relevant to differentiate both groups. These variables could be considered as ‘intermediate’ variables since they could influence the pathological pathway between the ‘exposure’ (ie, axSpA subgroup) and the outcomes; on the other hand, TNFb can be associated with both the outcome and the ‘exposure’ (eg, prescription rates were more important in the r-axSpA group), and as such it could also be considered as a ‘confounder’ variable. In any case, differences between r-axSpA and nr-axSpA were no longer evident after adjusting for these variables. To test the hypothesis that the answering to these questionnaires depend not only on the presence of sacroiliitis, and in an exploratory approach, we decided to evaluate factors that explain the mean level of BASDAI over time in these patients through the use of a multivariate linear regression. Interestingly, the mean BASDAI over the 5 years was explained by age, sex, education, radiographic sacroiliitis, TNFb and mean CRP. These results suggest that several factors influence the association between axSpA subgroups and the PROs.
This study has some weaknesses and strengths. One weakness is that we did not use central reading to classify r-axSpA and nr-axSpA patients. However, in the protocol, we planned to not use central reading in order to mimic clinical practice, in which only one rheumatologist or radiologist evaluates X-ray images. It should be noted that we did not separately analyse patients who switched from nr-axSpA to r-axSpA during the follow-up for two reasons: first, because as described by Dougados et al in this same cohort, only 5.1% of patients shifts from nr-axSpA to r-axSpA over 5 years2; and second, because we wanted to understand the behaviour of patients classified either as nr-axSpA or r-axSpA at baseline, regardless of the development of structural damage over time. Another limitation is the difficulty of precisely evaluating peripheral and extra-rheumatic manifestations that occur between two study visits. Thus, we used variables based on physical exploration and clinical interviews and accumulated information from previous study visits. Moreover, we considered the occurrence of the first episode of each manifestation as a primary outcome because we did not have information about flares between visits. One strength of this study is that we removed from the analysis patients who left the DESIR cohort because of a diagnosis other than axSpA according to the rheumatologist’s opinion; thus, all patients included in this study were diagnosed as patients with axSpA.
In summary, in this study we observed that both r-axSpA and nr-axSpA seem to behave similarly over time since the incidence of peripheral and extra-rheumatic manifestations are not different after 5 years of follow-up. Although the nr-axSpA group showed a greater disease burden, these differences disappeared after adjusting for intermediate variables, suggesting the influence of multiple factors on questionnaires scores. These highlighted results confirm the concept of axSpA as a single disease, which implies that both r-axSpA and nr-axSpA patients should be treated with equal priority.
Acknowledgments
These results were presented at the 2019 ACR/ARP Annual Meeting (Atlanta, USA) and published as a conference abstract (abstract number 609). The DESIR cohort was sponsored by the Département de la Recherche Clinique et du Développement de l'Assistance Publique–Hôpitaux de Paris. This study is conducted under the umbrella of the French Society of Rheumatology and INSERM (Institut National de la Santé et de la Recherche Médicale). The database management is performed within the department of epidemiology and biostatistics (Professor Paul Landais, D.I.M., Nîmes, France). An unrestricted grant from Pfizer was allocated for the first 10 years of the follow-up of the recruited patients. The authors thank the different regional participating centers: Professor M Dougados (Paris—Cochin B), Professor A Kahan (Paris—Cochin A), Professor P Dieudé (Paris—Bichat), Pr L Gossec (Paris—Pitié-Salpetrière), Professor F Berenbaum (Paris—Saint Antoine), Professor P Claudepierre (Créteil), Professor M. Breban (Boulogne Billancourt), Dr B. Saint-Marcoux (Aulnay-sous-Bois), Professor P Goupille (Tours), Professor J-F. Maillefert (Dijon), Dr E Dernis (Le Mans), Professor D Wendling (Besançon), Professor B Combe (Montpellier), Professor L Euller-Ziegler (Nice), Professor P Orcel, Professor P Richette (Paris—Lariboisière), Professor P Lafforgue (Marseille), Dr P Boumier (Amiens), Professor M Soubrier (Clermont-Ferrand), Dr N Mehsen (Bordeaux), Professor D Loeuille (Nancy), Professor R-M Flipo (Lille), Professor A Saraux (Brest), Dr S Pavy (Kremlin Bicêtre), Professor A Cantagrel (Toulouse), Professor O Vittecoq (Rouen). The authors also thank URC-CIC Paris Centre for the coordination and monitoring of the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Contributors The author and co-authors contributed equally to this paper: design of the work, analysis and/or interpretation of data, drafting the work or revising it critically, and final approval of the version to be published. The corresponding author certifies that all authors approved the entirety of the submitted material and contributed actively to the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Comitte de Protection des Personnes Ile de France III.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data sets generated and/or analysed during the current study are not publicly available due to consent restrictions. Programming codes used for statistical analysis during the current study are available from the corresponding author upon reasonable request.