Article Text

Abstract
Background After inadequate response to an antitumour necrosis factor (aTNF) agent for treatment of rheumatoid arthritis (RA), rheumatologists can choose an alternative aTNF or a biological agent with another mode of action (non-aTNF biological (non-aTNF-Bio)).
Objective To compare drug retention rates of non-aTNF-Bio with alternative aTNF.
Methods All patients within the Swiss RA cohort (SCQM-RA) treated with an alternative biotherapy after a prior inadequate response to aTNF were analysed. The drug retention of alternative aTNF was compared with non-aTNF-Bio using Cox proportional hazards models, adjusted for potential confounders.
Results 1485 treatment courses after aTNF failure were available for analysis, 853 with alternative aTNF and 632 with non-aTNF-Bio. The median drug retention was 32 months (IQR 14–54) on non-aTNF-Bio versus 21 months (IQR 8–53) on alternative aTNF, or a 50% reduction drug discontinuation risk in favour of non-aTNF-Bio (adjusted hazard ratio (HR) for non-aTNF-Bio: 0.50 (95% CI 0.41 to 0.62)). This effect appears to be modified by the type of prior aTNF failure, with a larger difference in favour of non-aTNF-Bio in patients having experienced a primary failure with a previous aTNF (HR: 0.33 (95% CI 0.24 to 0.47), p<0.001).
Conclusion After inadequate response to aTNF, and particularly after primary failure, patients on a non-aTNF-Bio agent have significantly higher drug retention rates.
Statistics from Altmetric.com
Introduction
In the last decade, the prognosis of severe rheumatoid arthritis (RA) patients has improved owing to the development of biological disease modifying antirheumatic drugs (DMARDs) such as tumour necrosis factor (TNF) inhibitors (antitumour necrosis factor (aTNF)).1,–,3 However, growing experience with aTNF has also demonstrated that these drugs are often not the final step in RA treatment. Indeed, drug retention of these therapies remains modest, long term remissions are rare and loss of efficacy frequent.
In the last 5 years, biological agents with different modes of action (non-aTNF biological (non-aTNF-Bio)), such as rituximab (RTX), tocilizumab (TCZ) and abatacept (ABA), have been developed and added to the therapeutic arsenal of RA. Encouraging data have been reported on their clinical efficacy and on their ability to limit progression of joint erosions.4,–,6
Hence, after inadequate response to a first aTNF agent, there is a choice to use either an alternative aTNF or to switch to a non-aTNF-Bio. Several observational studies have suggested a better effectiveness of non-aTNF-Bio when compared with a second aTNF after failure to a previous aTNF treatment, in particular after primary inefficacy.7 8 Moreover, another aTNF course given after a first aTNF failure tends to be stopped for much the same reason as the first treatment discontinuation.9
Two different types of aTNF failure—primary or secondary—have been distinguished in the literature. Although consensus is lacking, most consider primary failure as complete lack of efficacy, whereas secondary failure refers to a loss of treatment efficacy after an initial clinical response of variable duration. Recent data suggest a difference in the treatment response to a second aTNF depending on the type of treatment failure.10 So far, no consensus exists on the sequence of biological agent prescription after a failure to a prior aTNF.
The aim of this study was to compare overall effectiveness of non-aTNF-Bio with an alternative aTNF after inadequate response to prior aTNF in the treatment of RA. We further explored potential effect modification by terms of primary versus secondary failure to the previous aTNF.
Patients and methods
This is a nested cohort study within the Swiss RA registry (SCQM-RA), a population-based, observational cohort study of RA patients. All patients from the SCQM-RA cohort who failed at least one aTNF and subsequently received ABA, RTX, TCZ or one of the three original aTNF agents were included in this analysis. Due to the extremely low number of patients who have received certolizumab, pegol and golimumab at the time of analysis, these agents were not included in our study. Patients on their first course of aTNF and patients with missing information concerning dates of initiation or discontinuation of treatment were excluded from the analysis.
The primary outcome of this analysis was drug retention, which can be considered a proxy for treatment effectiveness and treatment safety. Treatment exposure was defined as the interval between initiation and the date of the last administration plus the usual duration of effect for each drug. Treatment exposure for RTX can be controversial because of its open-ended duration of effect. In our primary analysis, treatment exposure for RTX was operationally defined as the time between the first and the last RTX infusions plus 6 months or the discontinuation date was given specifically by the physician in charge. In the first alternative for RTX discontinuation, we used the date of a major change in antirheumatic therapy, which included the start of another biological agent, the initiation of a new DMARD co-therapy or the initiation of a glucocorticoid therapy at 10 or more mg/day. In yet another alternative definition of RTX exposure, we defined RTX exposure until the last RTX administration without adding a 6-month period of usual duration effect. In sensitivity analyses, we have varied this definition to test the solidity of our assumptions. We further explored the effect modification in terms of primary versus secondary failure of prior aTNF therapy. Because a validated definition of primary inefficacy is lacking, we operationally defined primary aTNF failure as a treatment discontinuation occurring within 6 months of initiation, except when another specific cause was reported.
Statistical analysis
Baseline characteristics were compared using conventional descriptive statistics. All analyses were two tailed, with an alpha error level at 0.05. The STATA version XI software was used for the analysis.
Drug discontinuation is strongly associated with the number of previous treatment failures;11 thus, we decided to stratify our analysis by the number of previous biological agents received. Furthermore, individual patients could have received several consecutive biological agents over time; therefore, we analysed time until discontinuation using a Cox proportional hazard model modified for the multiple failures per subject data (Anderson-Gill model). A priori, we considered age, sex, rheumatoid factor, baseline disease activity score in 28 joints, health assessment questionnaire and rheumatoid arthritis disease activity index scores, concomitant use of glucocorticoids, methotrexate, leflunomide or other DMARDS, concomitant use of prednisone >7.5 mg/day, duration of disease, number of previous biologic failures and calendar year of treatment initiation as potential confounders. Subsequent analyses were adjusted for these variables using multivariate Cox regression models. Crude drug retention was displayed using a Kaplan Meier survival curve.
Results
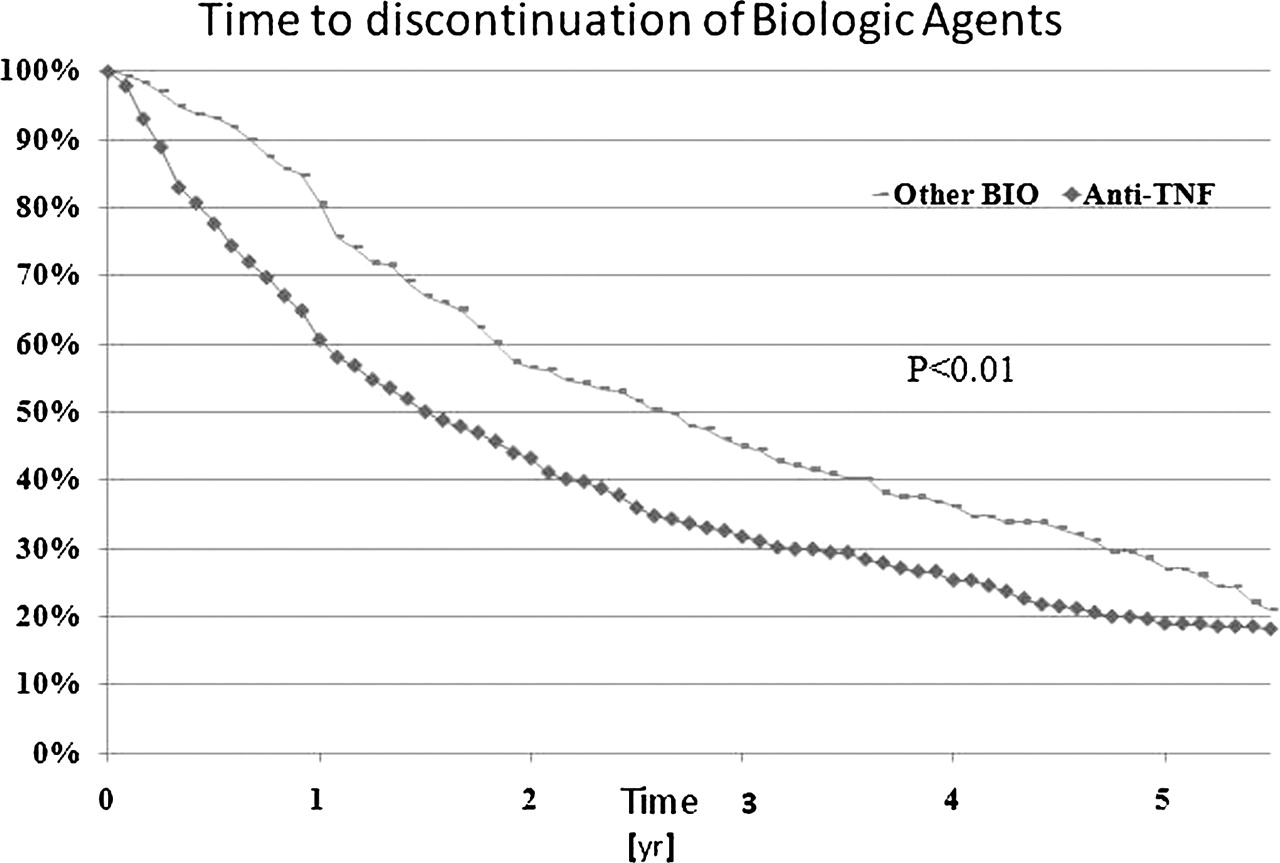
A total of 1485 biologic treatment courses in aTNF inadequate responders were retrieved, of which 853 were with an alternative aTNF and 632 with a non-aTNF-Bio (table 1). A second biological agent was administrated 1046 times, a third 331 times, a fourth 88 times and a fifth 20 times, contributing altogether to 2142 patient-years on biological agents. We did not find significant differences in baseline disease characteristics between the two groups, except for the rheumatoid factor, the number of previously failed biological agents and concomitant DMARDs (table 1). The multivariate analysis was adjusted for these parameters. The crude median duration on a non-aTNF-Bio was 31 months (IQR 13–63) vs 21 months (IQR 7–53) on alternative aTNF (figure 1).The drug retention rate was significantly higher with non-aTNF-Bio compared with an alternative aTNF (crude hazard ratio (HR): 0.75 (95% CI 0.63 to 0.89), adjusted HR: 0.50 (95% CI 0.41 to 0.62)). When we varied the definition for RTX exposure, the sensitivity analyses did not substantially change the results and conclusions remained qualitatively the same (data not shown). The benefit of switching to a non-aTNF-Bio was present for all three individual agents, but due to lower numbers, not necessarily always in a statistically significant manner. We found no evidence for effect modification by number of previous failures (p=0.69); the HR for non-aTNF-Bio was 0.48 (95% CI 0.37 to 0.62) after a single aTNF failure, and 0.51 (95% CI 0.33 to 0.77) after two or more failures.
{kind=link}
Time to discontinuation of biologic agents.
Study population
After primary failure with aTNF therapy, the difference of treatment retention in favour of the non-aTNF-Bio (HR: 0.33 (95% CI 0.24 to 0.47, p<0.001)) was even larger. HRs of treatment failure increased with the number of switches due to failed biological agents (third biologic HR: 1.32 (95% CI 1.07 to 1.62), fourth biologic: HR: 1.6 (95% CI 1.06 to 2.42), fifth biologic HR: 2.8 (95% CI 1.22 to 6.62)). A time trend for increasing rates of drug discontinuation exists in recent years, with HRs increasing after 2005 from 1 to 1.31 (95% CI 1.02 to 1.67) in 2005–2007, from 1 to 1.83 (95% CI 1.45 to 2.32) in 2007–2009 and from 1 to 2.12 (95% CI 1.55 to 2.89) after 2009.
Discussion
Drug retention is a useful composite measure of effectiveness, tolerance and patient satisfaction. In our study, we report longer treatment retention after switching to a biologic with an alternative mode of action (non-aTNF-Bio) compared with switching to another aTNF. Moreover, in case of primary failure to an aTNF, the difference between the two groups was even more in favor of the non-aTNF-Bio.
To the best of our knowledge, this is the first study that directly compares switching to an alternative aTNF with a non-aTNF-Bio, while distinguishing primary from secondary failure. As such, it provides new insights about potential strategies to consider after inadequate response to an aTNF. A recent cohort study suggested a better effectiveness of switching to an alternative aTNF after secondary failure than primary failure which supports our findings. However, it did not compare aTNF with non-aTNF-Bio discontinuation rates.12 Pathophysiological mechanisms of primary failure remain unclear. Secondary failure has been linked to immunogenicity and development of antidrug antibodies for the monoclonal antibodies, providing a rational for switching to an alternative aTNF.13 However, it has also been demonstrated that patients with antibodies against one anti-TNF have a higher risk of developing antibodies against a second aTNF,14 which supports an argument for switching to a non-aTNF-Bio. Limitations of this analysis include the absence of a clear definition of RTX drug exposure and an ad hoc definition of primary versus secondary drug failure. Moreover, no data on drug levels or antidrug antibodies are available. As in most observational studies, some covariates were missing and some patients were lost to follow-up. We addressed this by using the population mean for the sporadically missing covariates and used survival analyses, which is a robust outcome in case of right censorship, as long as the censorship is ‘non-informative’.15 We were not able to exclude potential confounding by mode of administration, unmeasured confounding and selection bias. There are currently no formal guidelines available on what biological to use and in which sequence after failure with an aTNF agent. Hence we believe that confounding by indication is unlikely.
The major strength of this study is the large population-based cohort of RA patients, reflecting ‘real world’ practice.
Conclusion
In patients with at least one inadequate response to a previous aTNF agent, we demonstrate significantly higher drug retention for biological agents with a different mode of action compared with alternative aTNF agents, particularly in patients with primary failure. These data suggest that switching to a biologic with a different mode of action might be more effective than switching to an alternative aTNF after prior failure with an aTNF.
Acknowledgments
The authors are grateful to the participating physicians and patients who made this study possible. A list of rheumatology offices and hospitals that are contributing to the SCQM registries can be found at www.scqm.ch/institutions.
References
Footnotes
-
Funding Rheumasearch Foundation Switzerland.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Correction notice This article has been corrected since it was published Online First. The layout of “Table 1” has been amended and extra text has been added to the footnotes of the table.