Article Text

Abstract
Background Suppression of the immunoinflammatory cascade by targeting interleukin 6 (IL-6) mediated effects constitutes a therapeutic option for chronic inflammatory diseases. Tocilizumab is the only IL-6 inhibitor (IL-6i) licensed for rheumatoid arthritis (RA) and juvenile idiopathic arthritis (JIA), but also other agents targeting either IL-6 or its receptor are investigated in various indications.
Objective To review published evidence on safety and efficacy of IL-6i in inflammatory diseases.
Methods We performed systematic literature searches in Medline and Cochrane, screened EULAR and American College of Rheumatology meeting-abstracts, and accessed http://www.clinicaltrials.gov.
Results Comprehensive evidence supports the efficacy of tocilizumab in RA in DMARD-naïve patients, and after DMARD- and TNFi-failure. Randomised comparisons demonstrate superiority of tocilizumab in JIA, but not ankylosing spondylitis (AS). Other indications are currently investigated. Additional IL-6i show similar efficacy; safety generally appears acceptable.
Conclusions IL-6i is effective and safe in RA and JIA, but not in AS. Preliminary results in other indications need substantiation.
- Rheumatoid Arthritis
- Juvenile Idiopathic Arthritis
- Treatment
- DMARDs (biologic)
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Introduction
Therapeutic options for rheumatoid arthritis (RA) and other inflammatory diseases are rapidly increasing. In addition to synthetic disease modifying anti-rheumatic drugs (DMARDs), biological agents that selectively target either cell-bound structures or cytokines are now available. Among those, suppression of the IL-6 mediated pathway has been the most recently introduced treatment principle, confirming the role of IL-6 in the pathophysiology of inflammation.1 The only agent currently approved for IL-6- inhibition is tocilizumab, an antibody to the IL-6-receptor, but other compounds targeting this structure or its ligand IL-6 are currently in development. In this review, we assemble the state of knowledge regarding IL-6 blocking therapy in inflammatory rheumatologic diseases.
Methods
Data Sources and Searches: We performed a systematic literature research of electronic databases. Our initial search included publications of Medline and Cochrane, each from their inception to January 2012. We also searched abstract archives of European League Against Rheumatism (EULAR)2 (2010–2012) and American College of Rheumatology (ACR)3 (2010 and 2011) conferences and accessed the National Institutes of Health database on clinical trials4 for preliminary results from on-going trials.
Study selection
By title and abstract screening, we evaluated all retrieved publications according to the inclusion-criteria. Online supplementary table S1 enlists the search terms and describes our approach regarding the population, intervention, control and outcomes.
Data synthesis
We performed meta-analyses of comparable randomised controlled trial (RCT) data, using Meta-Analyst software.5 We tested for heterogeneity among the included trials (Cochrane's Q) and present the results of a random effects model (DerSimonian Laird). We provide descriptive comparisons of non-randomised prospective trials and observational data.
Data Extraction, Quality Assessment: We extracted efficacy data on clinical, functional and radiographic outcomes as well as safety data from all included studies. We evaluated all RCTs according to the Jadad scoring system6 and followed PRISMA reporting guidelines.7 Some of the results are shown in the online supplementary file which is part and parcel of this publication.
Results
We initially retrieved 3935 Medline and 39 Cochrane publications for screening, and selected 166 fulltext papers for inclusion in this review. Furthermore, we found 293 eligible abstracts from recent scientific meetings and incorporated results from four ongoing trials (http://www.clincialtrials.gov) (figure 1).

Search and selection process.AoSD, adult onset Still's disease; ACR, American College of Rheumatology conference, CLE, cutaneous lupus erythematosus; EULAR, European League Against Rheumatism; IBD, inflammatory bowel disease; inhib., inhibitors, JIA, juvenile idiopathic arthritis; N, number; PMR, polymyalgia rheumatica; RA, rheumatoid arthritis, SpA, spondyloarthropathy; SLE, systemic lupus erythematosus; SSc, systemic sclerosis.
Here we focus primarily on RA and tocilizumab, but also address other licensed and off-label indications and other compounds.
Efficacy
Rheumatoid arthritis (RA)
Randomised comparisons demonstrated the efficacy of tocilizumab in DMARD-naïve patients,8 in insufficient responders (IR) to DMARDs,9–19 and in IR to TNF-inhibitors (TNFi).20–22 If not indicated otherwise, results of the 8 mg/kg dose, given intravenously 4-weekly, are reported. Outcomes are summarised in table 1. Quality scoring of RCTs is provided in online supplementary table S2.
Tocilizumab: pivotal randomised controlled trials in rheumatoid arthritis
Clinical outcomes
ACR20/50/70 responses at 24 weeks were 69/45/27% using tocilizumab monotherapy in DMARD-naïve patients, compared with 54/33/14% on methotrexate (MTX) monotherapy, and 56–80/30–64/4–44% (ACR20/50/70) in DMARD-IR, when compared with placebo-arms (usually continued or de novo MTX therapy, with ACR20/50/70 response rates of 17–34/21–26/2–20%). Finally, in TNFi-IR, tocilizumab achieved 50/27–29/10–12% (ACR20/50/70) at 24 weeks versus 10/4/1% in the MTX plus placebo-arm (tables 1 and S2). In a recently published small prospective study of patients receiving tocilizumab after failure of ≥2 DMARDs, one TNFi, and rituximab, 49/20% achieved EULAR good/moderate response.23 Efficacy was sustained during long-term extensions (LTE) of several RCTs.24–27 Drug-free DAS28 remission rates were 35% 24 weeks after withdrawing tocilizumab and 13% 52 weeks thereafter28 and tocilizumab re-treatment upon flares was successful in the Japanese DREAM- and RESTORE studies.29 ,30 Patients can also maintain tocilizumab-free remission rates with continued MTX, as recently reported in sub-analyses of the OPTION-study.31
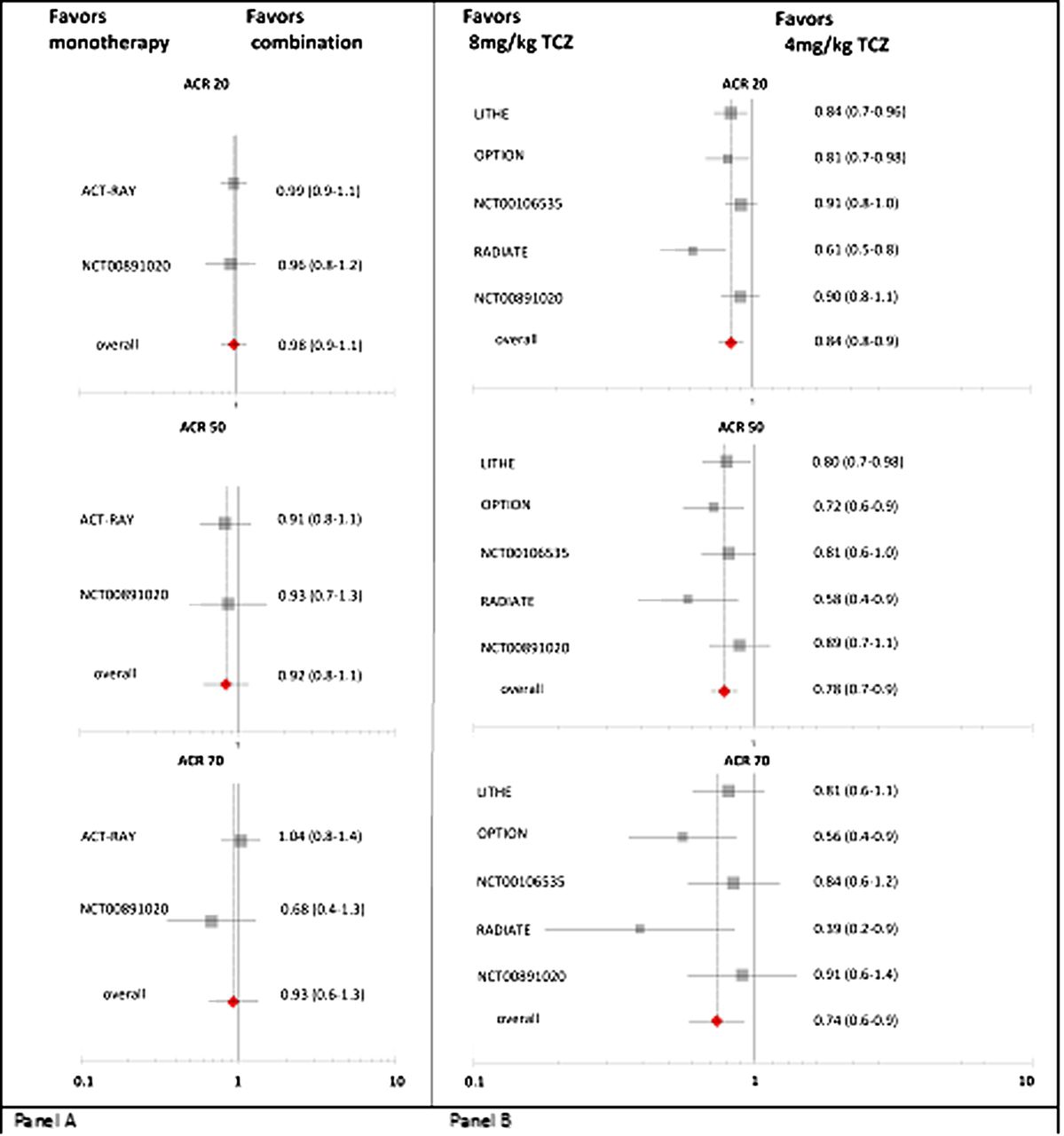
In the ACT-RAY-trial,17 MTX-IR were randomised to either tocilizumab monotherapy (withdrawing MTX), or tocilizumab added to MTX. A superior efficacy of the combination treatment could not be demonstrated in any of the clinical, functional or radiographic endpoints. These results have been confirmed in TNFi-IR.22 Figure 2A displays the risk ratios (RR) and CIs comparing tocilizumab monotherapy versus combination therapy in RCTs. Several non-randomised, open-label studies support the finding that mono- and combination therapy are similarly effective.32–35
{kind=link}
{kind=link}
ACR20/50/70 response rates. (A) Comparison of tocilizumab monotherapy versus combination of tocilizumab with DMARDs. (B) Comparison of 4 mg/kg versus 8 mg/kg 4-weekly. Risk ratios and 95% CIs are displayed. RR>1 favour combination therapy (in panel A) or the 4 mg/kg TCZ dose (in panel B). ACR, American College of Rheumatology
Physical function also improved significantly on tocilizumab as monotherapy8 ,12 ,14 ,17 or combined with DMARDs:11 ,17 ,20 59–60% of patients achieved minimal clinical important difference of Health Assessment Questionnaire (HAQ) (defined ≥0.3 or 0.22) after 24 weeks,8 ,10 ,11 ,14 ,17 ,20 52% after 52 weeks,12 ,13 compared with 34–53% in the respective placebo groups (table 1).
Radiographic outcomes are available from the LITHE-,13 SAMURAI-12 and ACT-RAY-17 trials: tocilizumab in combination with MTX13 ,17 or monotherapy12 ,17 retarded radiographic progression after 2417 or 52 weeks.12 ,13 MRI data showed early and sustained suppression of synovitis and osteitis.36–38 During long-term follow-up, no radiographic progression after 3 years occurred in 67–69%.39 Radiographic benefit was linked to decreased C-reactive protein and cartilage turnover markers.40 Preliminary results indicate that tocilizumab also improves bone mineral density in RA41 ,42 (table 1).
Dose
Superior efficacy of the 8 mg/kg 4-weekly dose was seen with regard to clinical responses in DMARD-IR11 ,13 ,18 and TNFi-IR.20 ,22 Figure 2B depicts the risk ratio (RR, and 95% CI) of ACR-responses with 8 mg/kg tocilizumab versus 4 mg/kg; overall, this difference is significant. Nevertheless, radiographic outcome was similar at both doses.13 This could indicate a dissociation between inflammation and damage by tocilizumab.43
Some meta-analyses of trial data and observational studies suggest superior efficacy of tocilizumab combination with MTX in DMARD-IR when compared with TNFi, abatacept, and rituximab.44–47 However, one network meta-analysis reported higher response rates for etanercept and certolizumab.48 In a meta-analysis of trials including TNFi-IR, outcomes of tocilizumab and abatacept, golimumab, and rituximab were similar.49 Observational data confirmed these analyses showing similar efficacy of biologics combination therapy in TNFi-IR.50 In the first available direct randomised comparison of biologicals as monotherapy,51 tocilizumab was superior to adalimumab in DMARD-IR; however, TNFi monotherapy in general and particularly adalimumab are inferior to combination with MTX.52
In conclusion, RCTs unanimously confirm efficacy of tocilizumab in RA, and non-randomised prospective studies35 ,53 ,54 observational studies45 ,55–59 and registry data60 ,61 corroborate this. Recently published reviews of tocilizumab in RA also confirm this conclusion.62 Tocilizumab is also effective as subcutaneous formulation.63 ,64
Another substance directed against the IL-6-receptor, sarilumab, is in early phase trials.65 ,66 Agents that directly target IL-6 also show promising preliminary results, among those, sirukumab,67–69 B-E8,70 and BMS-945429, that demonstrated rapid and sustained ACR-response in MTX-IR.71–73 Lastly, olokizumab, a humanised IL-6 antibody, is currently investigated in phase II dose-ranging studies74 ,75 for RA. Data are compiled in online supplementary table S4.
Juvenile Idiopathic Arthritis (JIA)
A number of randomised trials show efficacy in systemic JIA. These are summarised in online supplementary table S3. Clinical response (ACR30pedi/50/70) to tocilizumab 8 mg/kg q2 weeks was 85/85/71% after 12 weeks;76 sustained efficacy was seen during LTE with 88/89/65% ACR response rates after 1 year77 and 88% (ACR70) and 71% (ACR90) after 2 years.78 Remission rates were 67% over 3.5 years,79 and 38% of patients had drug-free remission at 6 years.80 Several studies also addressed IL-6i in poly- or oligoarticular JIA, and reported clinical success,81–85 however, no randomised comparison in this patient population is available to date.
Other Indications
In ankylosing spondylitis, no benefit could be shown in randomised comparisons. Results are further elaborated in the online supplement. In this document, also data on case reports or small studies for various indications are expanded. Indications include adult onset Still's disease, polymyalgia rheumatica, multi-refractory vasculitis, relapsing polychondritis, Castleman's disease, systemic lupus erythematosus and systemic sclerosis. In Crohn's disease, tocilizumab was clinically superior to placebo.
Safety
A Cochrane review of tocilizumab in RA reported 1.2x more frequent adverse events (AE) than for pooled placebo patients (74% vs 65%).86 No significant difference in serious AE (SAE), or withdrawals due to AE was reported.86 Retention rates have been repeatedly confirmed to be high,55 ,58 also suggesting acceptable safety. Cumulative safety data from RA trials, evaluating a total tocilizumab exposure of 8580 patient-years (PY),87 yielded an AE rate of 278/100 PY and SAE rate of 14/100 PY. These results are consistent with LTEs and postmarketing surveillance showing incidence rates of 43–44%88 ,89 or 167 events/100 PY90 (AE), and 9–10%88 ,89 or 27/100 PY27 ,90 (SAE). SAE increased with longer disease duration.89 Comparing the safety profile of tocilizumab to other biologicals, a meta-analysis investigated TNFi, anakinra, abatacept, rituximab, and tocilizumab91 and showed similar rates of SAE, serious infections, lymphoma, and congestive heart failure. An indirect comparison of abatacept, golimumab, and rituximab with tocilizumab in RA following TNFi-IR showed similar safety.53
AE of tocilizumab and other IL-6i primarily comprise infections, neutropenia, thrombocytopenia, hyperlipidaemia, gastrointestinal AEs and liver enzyme increases; details are presented in the online supplement.
Myocardial Infarction and Stroke
Myocardial infarction and stroke rates of pooled RCT treatment groups were 0.25/100 PY and 0.19/100 PY versus 0.49/100 PY and 0.24/100 PY in the pooled control group; without increase over time.87
Pregnancy
No complications were noticed in registries.92 ,93 Recently, outcomes of all pregnancies occurring in any of the pivotal RA-RCTs or LTEs, covering 10 994 PY, were presented: 33 pregnancies resulted in 7 spontaneous and 13 therapeutic abortions and 11 normal deliveries.94
Discussion
Tocilizumab is an efficacious biologic agent and is acceptably safe in RA and JIA. The efficacy data relate to clinical and functional aspects of these diseases. In ankylosing spondylitis (AS), randomised comparisons did not show beneficial effects. In other diseases, preliminary data highlight the need for future research: inhibition of the IL-6 pathway seems to become an option for the treatment of several other inflammatory diseases, but conclusive RCT data are still lacking. Antibodies against the ligand IL-6 could soon augment the armamentarium for targeted treatment of RA and JIA and appear to have similar efficacy and safety profiles as IL-6 receptor inhibition.
Acknowledgments
This study was made possible by a grant from Roche. However, no representative of the company attended the meetings or was involved in the literature search.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
-
Funding None.
-
Contributors All authors contributed and finally approved the current manuscript.
-
Competing interests DvdH: Consulting and/or speaking activities for and/or research grants from Roche/Chugai, BMS, Sanofi and Aventis; GB has been a consultant and speaker for Roche and BMS and has received grant support from Roche, BMS and Sanofi; MD received grant support from and has participated at advisory board meetings and symposia organised by Roche; PE has provided expert advice for Roche, BMS, Lilly, Sanofi and undertaken clinical trials for Roche and BMS; GFF has received speaking fees and research grants from Roche; CG received consultant/speakers fees from Roche and BMS; AG has been a consultant and speaker for Roche/Genentech and holds shares of BMS; JJGR received grant support from and has participated at advisory board meetings and symposia organised by Roche; GJ has received grant support given talks and served on advisory boards for Roche; TKK received grant support from and/or has participated at advisory board meetings and/or symposia organised by Roche, BMS, UCB; NN has received speaking, consulting fees and/or research grants from Chugai/Roche and BMS; NB's company has received income for services delivered to Roche; JSS received grant support from and has participated at advisory board meetings and symposia organised by Roche/Chugai/Genentech, BMS, Janssen, Sanofi and UCB. MS, FB, and MM declare no conflict.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Linked Articles
- Corrections