Article Text

Abstract
Objectives To synthesise the available evidence on pharmacological and non-pharmacological interventions recommended for fibromyalgia syndrome (FMS).
Methods Electronic databases including MEDLINE, PsycINFO, Scopus, the Cochrane Controlled Trials Registry and the Cochrane Library were searched for randomised controlled trials comparing any therapeutic approach as recommended in FMS guidelines (except complementary and alternative medicine) with control interventions in patients with FMS. Primary outcomes were pain and quality of life. Data extraction was done using standardised forms.
Results 102 trials in 14 982 patients and eight active interventions (tricyclic antidepressants, selective serotonin reuptake inhibitors, serotonin noradrenaline reuptake inhibitors (SNRIs), the gamma-amino butyric acid analogue pregabalin, aerobic exercise, balneotherapy, cognitive behavioural therapy (CBT), multicomponent therapy) were included. Most of the trials were small and hampered by methodological quality, introducing heterogeneity and inconsistency in the network. When restricted to large trials with ≥100 patients per group, heterogeneity was low and benefits for SNRIs and pregabalin compared with placebo were statistically significant, but small and not clinically relevant. For non-pharmacological interventions, only one large trial of CBT was available. In medium-sized trials with ≥50 patients per group, multicomponent therapy showed small to moderate benefits over placebo, followed by aerobic exercise and CBT.
Conclusions Benefits of pharmacological treatments in FMS are of questionable clinical relevance and evidence for benefits of non-pharmacological interventions is limited. A combination of pregabalin or SNRIs as pharmacological interventions and multicomponent therapy, aerobic exercise and CBT as non-pharmacological interventions seems most promising for the management of FMS.
Statistics from Altmetric.com
Introduction
Key symptoms of fibromyalgia syndrome (FMS) are chronic widespread pain associated with cognitive dysfunction, sleep disturbances and physical fatigue.1 ,2 Patients often report high levels of disability and poor quality of life, and an extensive use of medical care.3 In the absence of suitable laboratory tests, diagnosis is established by a history of key symptoms and the exclusion of somatic diseases sufficiently explaining these symptoms.2 ,4 The estimated overall prevalence of FMS is 2.9% in the general population of five European countries.5 The definite aetiology of FMS remains unknown.4 Since specific treatment aimed at altering the pathogenesis is not possible, the therapeutic focus is on symptom reduction.
Systematic reviews and evidence-based guidelines provide healthcare professionals and patients with a guide through the large variety of pharmacological and non-pharmacological treatment options offered to and used by patients with FMS.6 The American Pain Society7 and the Association of Scientific Medical Societies in Germany4 strongly recommend a pharmacological intervention (amitriptyline) and several non-pharmacological treatments (aerobic exercise, cognitive behavioural therapy (CBT), multicomponent therapy). Conversely, the European League Against Rheumatism (EULAR) have given only a strong recommendation for a variety of pharmacological therapies (eg, tricyclic antidepressants (TCAs), serotonin-noradrenaline reuptake inhibitors (SNRIs), serotonin reuptake inhibitors (SSRIs), gamma-amino butyric acid analogues (GABA) such as pregabalin) but weak recommendations for non-pharmacological therapies such as aerobic exercise, CBT and multicomponent therapy.8 Recommendations for first-line treatment options of FMS, however, are hampered by the lack of head-to-head comparisons of pharmacological versus non-pharmacological treatments.
Network meta-analyses allow a unified coherent analysis of all randomised controlled trials comparing pharmacological and non-pharmacological treatments head-to-head or with a control intervention, while fully respecting randomisation.9–11 We performed a systematic review with network meta-analysis of randomised trials in patients with FMS evaluating effects of pharmacological and non-pharmacological interventions recommended in FMS guidelines on pain and quality of life. We provide an overall synthesis of available data that can be used to guide treatment decisions and examined the potential for bias due to methodological flaws or small-study effects.12–15
Methods
Literature search and trial selection
We searched MEDLINE, PsycINFO, Scopus, the Cochrane Controlled Trials Registry and the Cochrane Library, all from inception through 31 December 2011. The search strategy has been previously described.16–21 We included treatment options approved by the Food and Drug Administration for FMS or recommended by evidence-based guidelines on the management of FMS:4 antidepressants, GABA-analogues, aerobic exercise, balneotherapy, CBT and multicomponent therapies (at least one exercise component and at least one psychological component). Therapeutic interventions were excluded if they had been studied in fewer than four trials or were classified as alternative and complementary medicine according to National Institutes of Health (NIH) criteria (http://nccam.nih.gov/health/whatiscam/). We included randomised controlled trials in patients with FMS defined according to established criteria,22–24 comparing any of these pre-specified therapeutic approaches with control interventions. Waiting list or treatment as usual were classified as non-intervention control, drug placebo or sham intervention as placebo control and interventions deemed a priori to be only minimally active (such as relaxation, education or passive physical therapy) as minimally active control. No language restrictions were applied. Two reviewers independently evaluated reports for eligibility and contacted a third reviewer to resolve disagreements.
Outcomes
Pain and quality of life were pre-specified as primary outcomes whereas the remaining key domains of FMS,25 sleep and fatigue were specified as secondary outcomes. Drop-outs, defined as patients who terminated the trial early for any reason during the treatment period, were extracted as a measure of acceptability.11 When there was more than one measure for a specific outcome, we gave preference to measures recommended by OMERACT.25
Data extraction
We used standardised forms of previous reviews to extract data on publication status, trial design, patients, characteristics and treatment regimens16–19 and to assess components of methodological trial quality (generation of randomisation sequence, allocation concealment, blinding of patients and handling of incomplete outcome data; for definitions see Methods S1 in the online supplement)12 ,26 independently by two reviewers. Results of the outcomes at the end of the treatment period were extracted by one reviewer (WH) and cross-checked by another (EN). We contacted corresponding authors of trials with incomplete outcome data. When necessary, means and measures of dispersion were approximated from figures in the reports.
Data synthesis
Whenever available we used results from intention-to-treat analyses. We expressed treatment effects as standardised mean differences (SMD) by dividing the difference in mean values between treatment groups at the end of treatment by the pooled standard deviation. If information for the calculation of pooled standard deviations was unavailable or ambiguous in a trial, we used the median pooled standard deviation from other trials using the same scale. Negative SMDs indicate a beneficial effect of the experimental intervention throughout. An SMD of −0.20 indicates small differences between groups whereas −0.50 suggests moderate and −0.80 large differences.27 Treatment effects for acceptability were expressed as risk ratios of dropouts.
Details of the statistical methods used for meta-analysis are provided in Methods S2 and S3 in the online supplement. In short, we used Bayesian hierarchical random effects models which fully preserve randomised treatment comparisons within trials.10 ,28 ,29 Pooled SMDs or risk ratios comparing different active and control interventions were estimated from the median of the posterior distribution, corresponding 95% credibility intervals (95% CrI) from the 2.5th and 97.5th percentiles. Credibility intervals can be interpreted similarly to conventional CI. We examined heterogeneity between trials, goodness of model fit and inconsistency between direct and indirect estimates30 ,31 and performed conventional Bayesian random effects meta-analyses for all available direct comparisons.32
For primary outcomes we drew funnel plots of trials comparing any active intervention with non-intervention or placebo controls,33 enhanced by contours dividing the plots into areas of significance and non-significance at a two-sided p=0.05,34 ,35 and added lines of predicted treatment effects derived from univariable random effects meta-regression models using the standard error as explanatory variable.36 ,37 Funnel plot asymmetry was assessed with Egger's test.38
We stratified analyses according to adequate generation of random sequence, concealment of allocation, blinding, intention-to-treat analysis, sample size and exclusion of patients with inflammatory rheumatic disorders or mental disorders and derived p values for interaction between trial characteristics and treatment effect as previously described.39 ,40 We pre-specified a cut-off of an average of 100 randomised patients per treatment group to distinguish between small and large trials.14 Since no large trials were available for most of the interventions and there was evidence for small-study effects, we explored the impact of trial size by a stepwise restriction of the analysis to trials of increasing sample size, with cut-offs of 25, 50 and 100 patients per treatment arm; 2×25 patients will yield more than 80% power to detect a large SMD of −0.80, 2×50 patients will yield more than 80% power to detect a moderate to large SMD of −0.60, and 2×100 patients more than 80% power to detect a small to moderate SMD of −0.40 at a two-sided α=0.05. Networks of pharmacological and non-pharmacological treatments failed to connect at cut-offs of 2×50 and 2×100 patients. We therefore used differences between non-intervention control and placebo observed in overall analyses to connect the two networks through combination of placebo and non-intervention control groups.
Results
Selection and characteristics of included trials
Figure 1 shows the flowchart for the selection of randomised trials in FMS. One hundred and two trials with 14 982 patients were eligible and contributed to the network meta-analysis (table 1 and supplementary online table S1). The trials included a median of 69 randomised patients (range 14–1196) and were published between 1986 and 2011. Fifteen trials evaluated TCAs (1026 patients), 10 trials SSRIs (644 patients), 10 trials SNRIs (5980 patients) and 4 trials the GABA analogue pregabalin (2625 patients). Thirty-three trials evaluated aerobic exercise (2266 patients), 9 trials balneotherapy (387 patients), 20 trials CBT (1712 patients) and 15 trials multicomponent therapy (1751 patients). Thirty-eight trials had a non-intervention control (2689 patients), 40 trials had a placebo control (10 545 patients) and 23 trials had a minimally active control (2129 patients). Forty-two trials (41%) reported an adequate randomisation schedule to allocate patients, 34 (33%) trials adequately concealed treatment allocation, 35 (34%) reported adequate blinding of patients and 20 (20%) reported analyses according to the intention-to-treat principle. The average age of the patients was 47 years, most were women and of Caucasian origin and had an average disease duration of 8.8 years. Figure 2 shows networks of analysed comparisons for the primary outcomes.
Characteristics of included randomised trials

Flowchart for the selection of randomised trials.

Network of analysed comparisons in the network meta-analyses of the primary outcomes. Numbers denote numbers of trials (number of analysed patients) per comparison for pain (normal type) and quality of life (italics). CBT, cognitive behavioural therapy; SNRIs, serotonin noradrenaline reuptake inhibitors; SSRIs, selective serotonin reuptake inhibitors; TCAs, tricyclic antidepressants.
Pain
Figure 3 (left) shows the effects on pain in 89 trials including 12 979 patients between active interventions and placebo. Balneotherapy showed very large effects, SSRIs, aerobic exercise, CBT and multicomponent therapy showed moderate to large effects and TCAs, SNRIs and pregabalin showed small to moderate effects compared with placebo. For all interventions, 95% CrIs did not overlap the null effect line. We found no clear difference between non-intervention controls and placebo (SMD 0.00, 95% CrI −0.31 to 0.30) but a small difference between minimally active controls and placebo (SMD −0.22 favouring minimally active controls, 95% CrI −0.54 to 0.09). Heterogeneity was high with an estimate of between-trial variance τ2 of 0.10 (95% CrI 0.06 to 0.17). Results of analyses stratified according to methodological and clinical characteristics of included trials are shown in supplementary online table S2. Heterogeneity between trials was much reduced when restricted to trials with adequate randomisation, allocation concealment or patient blinding and large trials with at least 100 patients per arm, but there was no clear pattern for effects depending on trial characteristics and tests for interaction between effects and characteristics were all non-significant (p≥0.54).

Estimates of standardised mean differences (SMDs) with 95% credibility intervals (95% CrI) in pain for therapeutic interventions compared with placebo from overall network meta-analyses and network meta-analyses restricted to trials with ≥25, ≥50 and ≥100 patients per group and corresponding between-trial heterogeneity variance estimates τ2 (95% CrI). Negative SMDs indicate benefit of therapeutic interventions compared with placebo. *Non-intervention control and placebo groups were combined to connect networks after correction for the SMD between non-intervention control and placebo of 0.00. CBT, cognitive behavioural therapy; SNRIs, serotonin noradrenaline reuptake inhibitors; SSRIs, selective serotonin reuptake inhibitors; TCAs, tricyclic antidepressants.
The scatter of effect estimates and the prediction lines observed in funnel plots for pain indicated asymmetry for both pharmacological and non-pharmacological interventions, with higher asymmetry for non-pharmacological interventions (figure 4, upper panel). Figure 3 (middle and right) shows results from network meta-analyses restricted to trials with ≥25 patients per group (53 trials, 11 746 patients), ≥50 patients per group (25 trials, 9784 patients) and ≥100 patients per group (14 trials, 8534 patients), respectively. In general, effects compared with placebo became less pronounced with increasing sample size of trials. The difference between balneotherapy and placebo was reduced in trials with ≥25 patients only (SMD −0.92, 95% CrI −1.60 to −0.26) and no trials with ≥50 patients were available for this intervention. When the network was restricted to trials with ≥50 patients per group the effects of TCAs (SMD −0.32, 95% CrI −0.66 to 0.02), aerobic exercise (SMD −0.37, 95% CrI −0.72 to −0.03) and CBT (SMD −0.32, 95% CrI −0.52 to −0.11) compared with placebo were reduced to small to moderate differences. The effects of pregabalin and multicomponent therapy were unaffected by the restriction. Heterogeneity between trials decreased from τ2=0.10 in the overall analysis to τ2=0.01 in the analysis restricted to ≥50 patients per group and, accordingly, the precision of estimates increased. Only SNRIs, pregabalin and CBT were evaluated in large trials with ≥100 patients per group and showed small to moderate effects compared with placebo. Heterogeneity was low with τ2 of 0.00 (95% CrI 0.00 to 0.03).
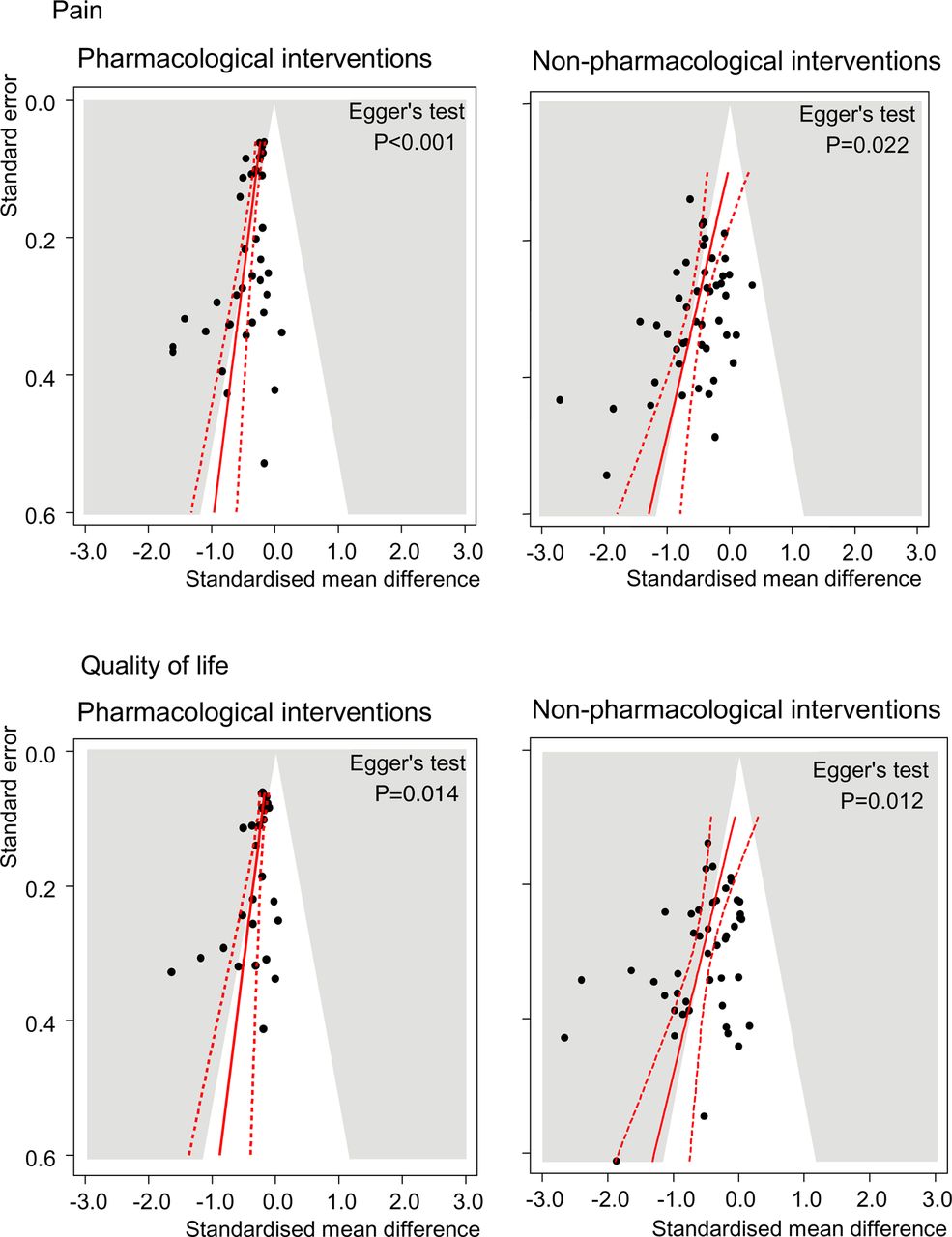
Contour-enhanced funnels plots for pain (top) and quality of life (bottom) comparing pharmacological (left) and non-pharmacological (right) with non-intervention control or placebo. Numbers on the x-axis are standardised mean differences (SMDs) and numbers on the y-axis are standard errors of SMDs. Areas of statistical significance at p=0.05 are shown in grey and prediction lines from univariable meta-regression models with the standard error as explanatory variable are shown in red. p Values are derived from regression tests for asymmetry.
Quality of life
Funnel plots for quality of life indicated asymmetry for both pharmacological and non-pharmacological interventions, again with higher asymmetry for non-pharmacological interventions (figure 4, bottom). Figure 5 shows results from the network meta-analysis overall (78 trials, 12 283 patients) and after stepwise restriction to trials with ≥25 patients per group (55 trials, 11 491 patients), ≥50 patients per group (26 trials, 9415 patients) and ≥100 patients per group (14 trials, 8120 patients). In the overall network, moderate to large effects for quality of life were found for all non-pharmacological interventions whereas pharmacological interventions showed small to moderate effects compared with placebo. Again we found no clear difference between non-intervention controls and placebo (SMD −0.13, 95% CrI −0.54 to 0.28) and a small to moderate difference between minimally active controls and placebo (SMD −0.34, 95% CrI −0.75 to 0.06). Heterogeneity between trials was high with a τ2 estimate of 0.14 (95% CrI 0.08 to 0.23). Results of stratified analyses were similar to those observed for pain except for a significant interaction between treatment effect and intention-to-treat analysis (p=0.016, see supplementary online table S3).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Estimates of standardised mean differences (SMDs) with 95% credibility intervals (95% CrI) in quality of life for therapeutic interventions compared with placebo from overall network meta-analyses and network meta-analyses restricted to trials with ≥25, ≥50 and ≥100 patients per group and corresponding between-trial heterogeneity variance estimates τ2 (95% CrI). Negative SMDs indicate benefit of therapeutic interventions compared with placebo. *Non-intervention control and placebo groups were combined to connect networks after correction for the SMD between non-intervention control and placebo of −0.13. CBT, cognitive behavioural therapy; SNRIs, serotonin noradrenaline reuptake inhibitors; SSRIs, selective serotonin reuptake inhibitors; TCAs, tricyclic antidepressants.
In general, the effects became smaller with restrictions to increasing sample size of trials and between-trial heterogeneity decreased from τ2=0.14 in the overall analysis to τ2=0.00 in the analysis restricted to ≥50 patients and ≥100 patients per group, respectively. We found moderate effects for multicomponent therapy (SMD −0.56, 95% CrI −0.76 to −0.36) after restriction to trials with ≥50 patients per group, moderate effects for CBT (SMD −0.60, 95% CrI −0.91 to −0.29) and small effects for SNRIs (SMD −0.21, 95% CrI −0.29 to −0.14) and pregabalin (SMD −0.21, 95% CrI −0.34 to −0.07) after restriction to trials with ≥100 patients per group. All other interventions were not significantly different from placebo with 95% CrI overlapping the null effect.
The results of network meta-analyses of secondary outcomes, sensitivity analyses, model fit and network consistency are shown in supplementary online tables S4–S10.
Discussion
In this systematic review and network meta-analysis of pharmacological and non-pharmacological interventions including 102 trials in 14 982 patients with FMS, most of the trials were very small and hampered by low methodological quality. We found evidence for small-study effects and high heterogeneity and inconsistency introduced by small trials. In network meta-analyses restricted to moderate or large-sized trials, we found advantages of pharmacological interventions over placebo on pain and quality of life, which were either statistically non-significant (SSRIs and TCAs) or of questionable clinical relevance despite statistical significance (SNRIs and pregabalin). Among non-pharmacological interventions, multicomponent therapy followed by aerobic exercise and CBT was most promising for reducing pain and improving quality of life. Of the non-pharmacological interventions, only CBT was evaluated in one large trial, for which it remained unclear whether allocation was adequately concealed.41 In general, treatment effects were slightly larger for pain than for quality of life.
To our knowledge, this is the first network meta-analysis to combine pharmacological and non-pharmacological interventions in FMS. We could analyse effects of pharmacological and non-pharmacological interventions reported in different trials in a single model irrespective of the control intervention used,42 which allowed us to estimate relative effects of two interventions that have not been compared directly. This single model assumes that relative treatment effects comparing two interventions in different trials originate from a common distribution. This, however, only holds in our networks restricted to medium-sized and large trials where heterogeneity and inconsistency were low.
Our study is based on extensive literature searches and we consider it unlikely that we have missed important trials. Nevertheless, for some interventions we identified only small trials of questionable methodological quality. Stepwise restriction to trials with larger sample size led to decreases of between-trial heterogeneity and network inconsistency and, generally, to a decrease in estimated benefits of interventions compared with placebo. We consider the results of network meta-analyses restricted to moderately-sized (≥50 patients per trial arm) or large trials (≥100 patients per arm) more credible than the overall analysis. However, the number of interventions available in the network decreased and, of the non-pharmacological interventions, only CBT remained in the network of large trials, which we consider one of the most important limitations. We deem estimates of CBT, balneotherapy and SSRIs most problematic as benefits changed by factors of 2–3 after restrictions of networks to larger trials. Since a moderate benefit of CBT was estimated in a single large trial with unclear allocation concealment,41 it is unclear whether this benefit can be confirmed in future adequately powered trials with appropriate design and conduct. Another limitation of our study is that some interventions, although widely used for the treatment of FMS in clinical practice (eg, tramadol), were not included in our analysis because they were studied in fewer than four trials.
The presence of small-study effects with large residual between-trial heterogeneity after stratification according to trial characteristics resulted in low power of interaction tests and non-significant p values, and should be interpreted with caution. Conversely, statistical and visual examination of funnel plots indicated asymmetry suggestive of small-study effects.15 Although true clinical heterogeneity may explain this asymmetry,15 ,43 it is more plausible that asymmetry arises from the cumulative effect of various biases at the level of design, conduct, analysis and publication. As previously suggested in the field of osteoarthritis,14 sample size could therefore be viewed as a proxy for the cumulative effect of various biases prevalent in randomised FMS trials.
In clinical practice, different effectiveness on key symptoms of FMS other than pain and quality of life might lead to the selection of a combination of various treatment modalities, both pharmacological and non-pharmacological. However, we did not find any intervention for which there was conclusive evidence for clinically relevant benefits on our secondary outcomes of fatigue, sleep disturbance or acceptability. Limited data are available from randomised trials about other clinical dimensions such as coping or patients’ beliefs, and we cannot make any conclusions about these. The generalisability of our findings derived from randomised trials to the clinical FMS population is limited, especially by the participation of selected FMS patients in randomised trials.16–21 ,44 Generalisability may also be hampered by protocol mandated repetitive follow-ups with extensive assessments and completion of multiple questionnaires. This would not be part of standard management and may themselves be considered as management strategies.
A recently published network meta-analysis of licensed dosages of pregabalin and the SNRIs duloxetine and milnacipran found similar benefits of these drugs over placebo on pain and quality of life, with evidence comparably robust to our network meta-analyses of large trials.45 Although statistically significant, differences in pain between pregabalin and placebo were approximately 0.6 cm on a 10 cm visual analogue scale corresponding to an SMD of 0.25.45 We consider the small advantages of pregabalin and SNRIs over placebo of questionable clinical relevance.40 Our results do not necessarily support EULAR recommendations currently favouring drug therapy over other treatment options.8 In our analysis restricted to moderate and large-sized trials, we found potentially important benefits of aerobic exercise, CBT and multicomponent therapy in the management of FMS, which is in line with recommendations of the American Pain Society and the Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften in Germany.4 ,7
In conclusion, evidence about effective and clinically relevant treatments for FMS is limited. Additional large-scale randomised trials of high methodological quality of promising non-pharmacological interventions such as CBT, aerobic exercise and multicomponent therapy are warranted. In view of the currently available evidence, a combination of pregabalin or SNRIs as pharmacological interventions and multicomponent therapy, aerobic exercise or CBT as non-pharmacological interventions seems most promising.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online Methods
- Data supplement 2 - Online Table 1
- Data supplement 3 - Online Tables 2 to 10
Footnotes
-
Contributors All authors had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. EN and WH contributed equally to the study. EN, WH and PJ contributed to the study concept and design and drafted the manuscript. WH and KB contributed to data collection. EN contributed to preparation and analysis of the data. All the authors contributed to the interpretation of the data and critically reviewed the manuscript for publication.
-
Funding EN was a recipient of a Marie Curie Intra-European Fellowship for Career Development (grant No FP7-PEOPLE-2010-IEF-273673). WH received honoraria for one educational lecture from Janssen-Cilag in the previous 3 years. KB was supported by the Rut- and Klaus-Bahlsen Foundation in Hannover, Germany. JB and PJ received a grant (No. 105314-118312/1) from the Swiss National Science Foundation. The funding bodies had no role in the design or conduct of the study; collection, management, analysis, or interpretation of the data; or preparation, review, or approval of the manuscript, or the decision to submit the manuscript for publication.
-
Provenance and peer review Not commissioned; externally peer reviewed.