Article Text

Abstract
Objectives To update the evidence for the efficacy of biological disease-modifying antirheumatic drugs (bDMARD) in patients with rheumatoid arthritis (RA) to inform the European League Against Rheumatism(EULAR) Task Force treatment recommendations.
Methods Medline, Embase and Cochrane databases were searched for articles published between January 2009 and February 2013 on infliximab, etanercept, adalimumab, certolizumab-pegol, golimumab, anakinra, abatacept, rituximab, tocilizumab and biosimilar DMARDs (bsDMARDs) in phase 3 development. Abstracts from 2011 to 2012 American College of Rheumatology (ACR) and 2011–2013 EULAR conferences were obtained.
Results Fifty-one full papers, and 57 abstracts were identified. The randomised controlled trials (RCT) confirmed the efficacy of bDMARD+conventional synthetic DMARDs (csDMARDs) versus csDMARDs alone (level 1B evidence). There was some additional evidence for the use of bDMARD monotherapy, however bDMARD and MTX combination therapy for all bDMARD classes was more efficacious (1B). Clinical and radiographic responses were high with treat-to-target strategies. Earlier improvement in signs and symptoms were seen with more intensive initial treatment strategies, but outcomes were similar upon addition of bDMARDs in patients with insufficient response to MTX. In general, radiographic progression was lower with bDMARD use, mainly due to initial treatment effects. Although patients may achieve bDMARD- and drug-free remission, maintenance of clinical responses was higher with bDMARD continuation (1B), but bDMARD dose reduction could be applied (1B). There was still no RCT data for bDMARD switching.
Conclusions The systematic literature review confirms efficacy of biological DMARDs in RA. It addresses different treatment strategies with the potential for reduction in therapy, particularly with early disease control, and highlights emerging therapies.
- Rheumatoid Arthritis
- DMARDs (biologic)
- Treatment
- Anti-TNF
Statistics from Altmetric.com
Introduction
Systematic literature reviews (SLR) on biological disease modifying drugs (bDMARDs)1 and treatment strategies including bDMARDs in rheumatoid arthritis (RA)2 were performed in 2010 to provide evidence that informed a European League Against Rheumatism (EULAR) Task Force for the development of the 2010 EULAR recommendations for the management of RA with DMARDs.3 Since then, several additional bDMARD studies have been published, as well as a number of studies evaluating different approaches and strategies, biosimilar DMARDs4 and tofacitinib, the first of a new class of targeted synthetic DMARDs that inhibit Janus kinase. Some studies have also addressed the use of bDMARDs at the earlier stages of the disease, during the undifferentiated inflammatory arthritis (UA) phase. The aim of this SLR was therefore to provide an update of the available evidence for the 2013 EULAR RA treatment recommendations.5 Where appropriate, we have used the recently proposed nomenclature for DMARDs that takes into account biosimilars (bsDMARDs) and also differentiates between conventional synthetic (cs) and targeted synthetic (ts) DMARDs.6
Methods
The Steering Group outlined the scope of the literature search on the role of bDMARDs in the treatment of RA, which, once performed, was discussed by a subgroup of the Task Force and subsequently the whole Task Force. Studies evaluating nine bDMARDs: infliximab (IFX), etanercept (ETN), adalimumab (ADA), certolizumab-pegol (CZP), golimumab (GLM), anakinra (ANA), abatacept (ABT), rituximab (RTX) and tocilizumab (TCZ) were included. Information on bsDMARDs in phase 3 development and tsDMARDs in the context of bDMARD therapy was also sought. The previous SLR included studies to 2009.1 This updated literature search was therefore performed for the period between January 2009 and February 2013 using Medline, Embase and Cochrane databases. Abstracts were also obtained from the 2011–2012 American College of Rheumatology (ACR) and 2011–2013 EULAR conferences. Where full papers of these abstracts were published online until mid-2013, the latter were obtained and used for data extraction. Relevant articles published after this time-point were also included.
The criteria for study selection were (1) randomised controlled trials (RCT) (double-blind stipulated for RCTs evaluating bDMARDs or bsDMARDs vs a csDMARD; for strategy-type trials and head-to-head studies open-label studies were also included as in the previous SLR2); (2) patients with RA (1987 ACR7 or 2010 ACR/EULAR RA classification criteria8) or UA at risk of developing RA; (3) studies evaluating one of the nine bDMARDs mentioned above or bsDMARDs in phase 3 or tsDMARDs in comparison with a bDMARD; (4) trials of ≥6 months’ duration; (5) studies with ≥50 patients; (6) publications in English. Published meta-analyses and SLRs were also reviewed and included where relevant.
As in the previous SLR, studies were grouped according to the following patient categories reflecting current clinical practice and trial design: (1) no prior DMARD use (DMARD naive); (2) no prior MTX use (MTX naive); (3) inadequate response to MTX (MTX-IR); (4) incomplete response to any csDMARD, which may not necessarily include MTX (mixed DMARD-IR); (5) inadequate response to tumour necrosis factor-inhibitor (TNFi; TNFi-IR). Levels of evidence were assigned according to the Oxford Centre for Evidence-based Medicine levels of evidence (http://www.cebm.net/index.aspx?o=1025).
Quality of published studies was assessed using the Cochrane risk of bias assessment tool for RevMan 5.1.9 Efficacy outcomes included those relating to signs and symptoms (ACR and EULAR responses), radiographic outcomes, physical function (Health Assessment Questionnaire Disability Index (HAQ)),10 quality-of-life measures (using the Physical Component Score and Mental Component Score of the Short Form-36)11 and fatigue (measured by the FACIT score12 ,13 and fatigue visual analogue scale (FAS)).
A meta-analysis of RCTs was performed comparing (1) bDMARD+csDMARDs versus csDMARD (2) bDMARD monotherapy versus csDMARD/placebo and (3) bDMARD+MTX versus bDMARD monotherapy. This was done for all patient populations where more than one new RCT was identified. This was not done for strategy trials due to the heterogeneity of the studies in terms of design, inclusion criteria, target and methodology, or for the individual head-to-head and bsDMARD studies, for which results have been described in tabulated form. Details of the search, the studies included and details of efficacy outcome measures extracted can be found in the online supplementary material.
The heterogeneous nature of the studies introduced significant challenges in the analysis and interpretation of the results; with the increasing number of therapies evaluated as well as treatment strategies adding to this complexity. When drawing conclusions from this initiative, we have acknowledged and taken careful consideration of the inherent biases associated with comparing different patient populations and different compounds, in studies using different statistical plans and powered for different endpoints.
Results
The initial search yielded 10 265 articles for titles and abstracts for screening of which 134 were selected for detailed review. Together with the additional conference, abstracts and full papers obtained from a hand search (including relevant articles found after the main search), 51 full papers and 57 abstracts met the inclusion criteria.
Overall risk of bias for the majority of studies evaluated was low. Several were not blinded and were therefore classed as ‘high risk of bias’ in terms of ‘blinding of participants and personnel’14–17 and ‘blinding of outcome assessment’.16 In some, under-recruitment was a noted concern, and studies were, therefore, also classed as high risk in the ‘incomplete outcome data’ category.16 ,18 ,19 Details can be found in the online supplementary section.
The efficacy data are summarised by addressing four main areas of bDMARD use: (1) bDMARD efficacy (in combination therapy with csDMARDs or as monotherapy, head-to-head bDMARD studies and bDMARD switching); (2) treatment strategies including bDMARDs; (3) bDMARD stopping or dose reduction; and (4) studies including bDMARDs and new therapies (bsDMARDs and tsDMARDs).
Biological DMARD efficacy
Outcomes in this group will focus on those relating to signs and symptoms with ACR responses for ACR70 responses shown by way of example. The ACR response, which was used by way of example in the original SLR, remained the most frequently reported measure demonstrating overall efficacy. Of the ACR responses, the ACR70 was chosen as it was felt to be the most clinically meaningful response, most closely representing low disease activity.20 Details of other efficacy outcomes including measures of low disease activity and remission can be found in the online supplementary section.
Biological DMARD±conventional synthetic DMARD versus conventional synthetic DMARD
Biological DMARD+MTX combination versus conventional synthetic DMARD
While there were no studies fulfilling inclusion criteria for DMARD-naive patients in the previous search, this update identified one study (‘HIT HARD’),21 which confirmed efficacy at 6 months for ADA+MTX versus moderate dose MTX (15 mg weekly) in this group. In the MTX-naive RA group, there was further evidence for efficacy for ADA22 and TCZ,23 and new data for RTX from the IMAGE study.24 In the MTX-IR group, there was data for all nine bDMARDS. Additional studies for this and the mixed DMARD-IR groups have been published for ANA,25 CZP26 ,27 and GLM.28–31 All confirm enhanced efficacy of a bDMARD+MTX versus placebo+MTX in MTX-naive RA (RR (95% CI) 1.68 (1.54 to 1.84) for ACR 70 responses) (figure 1A), bDMARD+MTX versus placebo+MTX in MTX-IR (RR (95% CI) 4.07 (3.21 to 5.17)) (figure 1B) and bDMARD+csDMARD versus csDMARD in mixed DMARD –IR (RR (95% CI) 4.74 (2.63 to 8.56)) (figure 1C) (level of evidence 1B). In a SLR and meta-analysis of four RCTs in TNFi-IR,32–35 which were included in our previous SLR,1 the mean pooled OR for ACR 70 (95% CI) was 7.43 (3.77 to 14.61)36 (level of evidence 1A). Although there were no new RCTs fulfilling inclusion criteria for this group, the 12-week REALISTIC RCT in which approximately 40% were TNFi-IR and subanalysed accordingly, confirmed clinical efficacy of CZP.37



(A) Risk ratios for the ACR 70 responses comparing a biological disease modifying antirheumatic drug (bDMARD) plus methotrexate (MTX) versus MTX monotherapy in patients with early rheumatoid arthritis who are MTX naive. ACR, American College of Rheumatology; *additional study since the 2010 systematic literature review1; † ACR 70 responses at 6 months for Kavanaugh 2013 OPTIMA, Emery 2009 GO-BEFORE and Burmester EULAR 2013 FUNCTION; all other ACR 70 responses are at 12 months. (B) Risk ratios for the ACR70 responses comparing the use of a biological disease-modifying antirheumatic drug (bDMARD) plus methotrexate (MTX) versus MTX monotherapy in patients with rheumatoid arthritis (RA) who are MTX-incomplete responders. ACR, American College of Rheumatology; *additional study since the 2010 systematic literature review1; †ACR 70 response at 12 months for Kremer 2011 LITHE; all other ACR 70 responses are at 6 months. (C) Risk ratios for the ACR70 responses comparing the use of a biological disease-modifying antirheumatic drug (bDMARD) plus synthetic disease-modifying antirheumatic drug (csDMARD csDMARD) versus csDMARD monotherapy in patients with rheumatoid arthritis for whom a csDMARD (not necessarily MTX) has failed. ACR, American College of Rheumatology; *additional study since the 2010 systematic literature review.1; † ACR 70 response at 12 months for Klareskog 2004 TEMPO; all other ACR 70 responses are at 6 months.
Biological DMARD monotherapy versus conventional synthetic DMARD
Our previous SLR failed to confirm clear efficacy of bDMARD monotherapy versus a csDMARD. Results once again have varied for this group with no clear benefit seen in subassessments of these patients in three more recent GLM RCTs.28 ,38–40 In the FUNCTION study, which aimed to assess the efficacy and safety of TCZ±MTX versus MTX in MTX- naive early RA, the TCZ 8 mg/kg monotherapy group met its primary endpoint (DAS28 ESR remission at 6 months: 38.7% vs 15% in the TCZ 8 mg/kg monotherapy vs MTX monotherapy groups, respectively, p≤0.0001). This endpoint, however, favours agents that, like tocilizumab, interfere with the acute-phase response, while ACR response rates (ACR20, ACR 50 and ACR70) and changes in physical function, which do not, were similar between the two groups. Radiographic progression at 12 months was lower in those receiving TCZ than MTX, being lowest in the TCZ 8 mg/kg+MTX combination group.23
Biological DMARD+MTX combination versus biological DMARD monotherapy
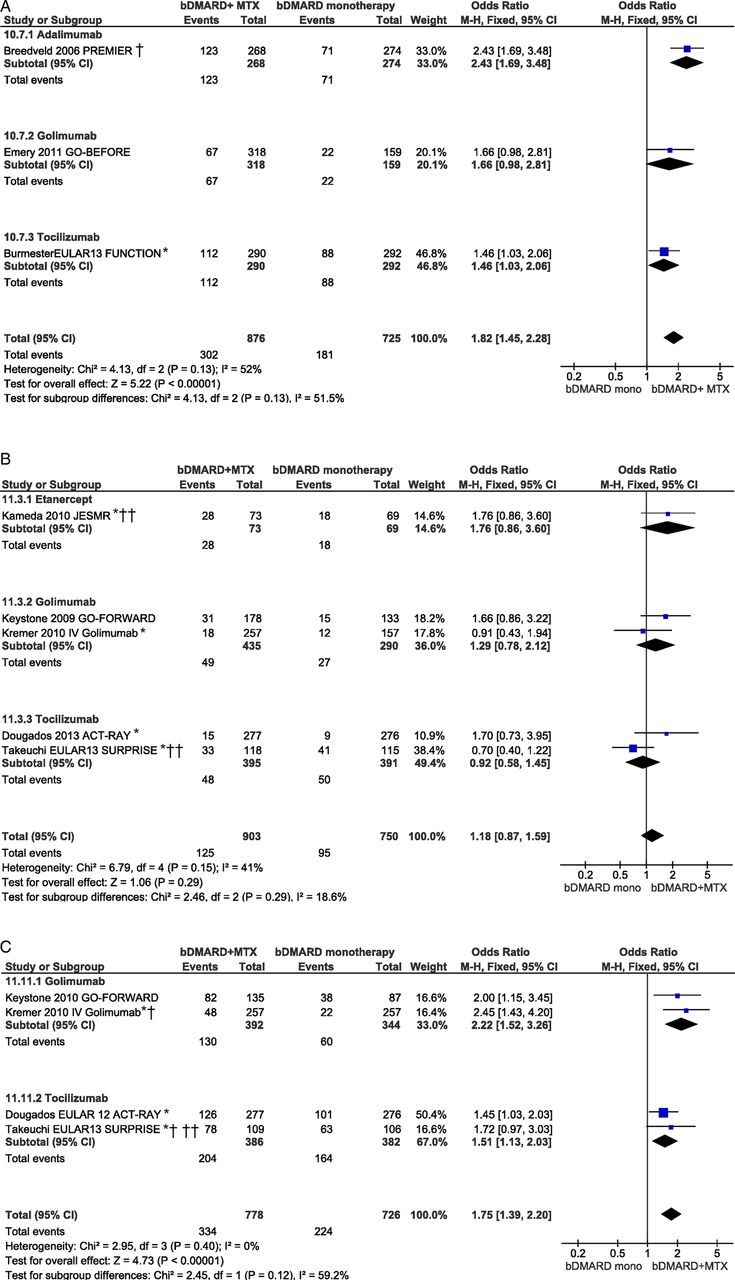
In several previously published RCTs in which bDMARD monotherapy was compared to MTX, better clinical and radiographic outcomes were seen with bDMARD+MTX than with a bDMARD alone.41 ,42 Data from RCTs with MTX-naive patients which include bDMARD+MTX and bDMARD monotherapy groups confirm clinical (and also structural) superiority of combination therapy (figure 2A).23 ,43

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Risk ratios for the ACR70 responses comparing the use of a biological disease-modifying antirheumatic drug (bDMARD) plus methotrexate (MTX) versus bDMARD monotherapy in patients with rheumatoid arthritis who are MTX-naive. ACR, American College of Rheumatology; *additional study since the 2010 systematic literature review1; † ACR 70 response at 12 months for Breedveld 2006 PREMIER; all other ACR 70 responses are at 6 months. (B) Risk ratios for the ACR70 responses comparing the use of a biological disease-modifying antirheumatic drug (bDMARD) plus methotrexate (MTX) versus bDMARD monotherapy in patients with rheumatoid arthritis who are MTX-incomplete responders. ACR, American College of Rheumatology; *additional study since the 2010 systematic literature review1; ACR 70 responses are at 6 months; †† open-label studies. (C) Risk ratios for the DAS28 remission comparing the use of a biological disease-modifying antirheumatic drug (bDMARD) plus methotrexate (MTX) versus bDMARD monotherapy in patients with rheumatoid arthritis who are MTX-incomplete responders. *Additional study since the 2010 systematic literature review.1; † DAS28 remission at 6 months for Kremer 2010 IV Golimumab and Takeuchi EULAR 2013 SURPRISE and ACR 70 at 12 months for Keystone 2010 GO-FORWARD and DOUGADOS EULAR 2012 ACT-RAY; †† open-label study.
A 16-week open-label study in MTX-IR RA, however, showed similar clinical and patient-reported outcomes with ETN+MTX versus ETN monotherapy.44 ,45 In this SLR, three studies were found, all in the MTX-IR group, directly comparing starting bDMARD+MTX combination therapy versus bDMARD monotherapy. In the open-label JESMR study, ETN+MTX was superior to ETN monotherapy for clinical outcomes. Although less radiographic progression was seen with combination therapy, the between-group difference was not statistically significant.14 ,46 Two studies compared the addition of TCZ with MTX (combination) with switching from MTX to TCZ monotherapy (MTX-withdrawal). In the non-inferiority SURPRISE study47 and in the ACT-RAY study, similar ACR 70 responses were seen for both groups at 6 months.48 (figure 2B) By contrast with the 6-month outcomes, however, 12-month data from the ACT-RAY study showed higher proportions of DAS28 remission and radiographic non-progression with combination TCZ+MTX (DAS28 remission 37% vs 46%, p=0.03 and radiographic non-progression 86% vs 92%, p=0.007 in the TCZ monotherapy and TCZ+MTX groups, respectively).49 (figure 2C)
One study has addressed the possibility of stepping down from bDMARD+MTX to bDMARD monotherapy. In the COMET study, patients were randomised at baseline for a 2-year period to MTX monotherapy for 1 year then continuing or adding ETN, or MTX+ETN for 1 year then continuing or stopping MTX.50 DAS 28 remission at 2 years in the group continuing MTX+ETN (EM/EM) and the step down to ETN monotherapy (EM/E) were 45% and 37%, respectively. Radiographic non-progression was high in both groups, but higher with combination therapy than with monotherapy (EM/EM vs EM/E 90% vs 75%, p 0.008).
Head-to-head biological DMARD studies
Two studies, both in MTX-IR RA, have evaluated two bDMARDs in a direct (‘head-to-head’) comparison. The AMPLE study compared ABT+MTX versus ADA+MTX combination therapy in an early RA cohort (less than 2 years).15 In this non-inferiority study, the primary endpoint (ACR20 response at 12 months) was met. Similar results were also seen for the ACR50 and 70 responses (ACR20, 50 and 70 response rates of 65, 46 and 29% vs 63, 46 and 26% in the ABT+MTX and ADA+MTX groups, respectively). The ADACTA study evaluated bDMARD monotherapy, comparing TCZ versus ADA.51 This superiority study showed a significantly greater change in DAS28 from baseline to 6 months in the TCZ 8 mg/kg monotherapy versus ADA 40 mg SC monotherapy group (difference (95% CI): −1.5 (−1.8 to −1.1), p<0.0001). ACR responses at 6 months were also higher in the TCZ monotherapy group (ACR20, 50 and 70 response rates of 65, 47 and 33% vs 49, 28 and 18% in the TCZ and ADA monotherapy groups, respectively), as were changes in the clinical disease activity index (CDAI) (which does not comprise an acute-phase reactant) (table 1).
Randomised controlled trials (RCT) of head-to-head biological DMARDs (bDMARD) and bDMARD RCTs including biosimilar and targeted synthetic DMARDs—American College of Rheumatology (ACR) responses
Switching between biological DMARDs
There were no RCTs fulfilling inclusion criteria for switching between bDMARDs.
Strategy trials
Several strategy trials have been published since the last EULAR SLR2 (tables 2 and 3) aiming to address the place of bDMARD therapy in the treatment of RA. These have mainly compared (1) step-up to a bDMARD versus step-up to csDMARD combination therapy after MTX failure (SWEFOT,16 TEAR,18 RACAT19); (2) bDMARD+MTX versus csDMARD (MTX) monotherapy as induction therapy (HIT HARD,21 TEAR,18 OPTIMA,22 COMET50); (3) induction therapy with bDMARDs versus combination csDMARDs (TEAR18) and (4) evaluated bDMARD therapy versus csDMARD within a treat-to-target approach, in which patients were seen at regular intervals with treatment changes if a treatment outcome (eg, low disease activity or remission) was not met (Neo-RACo,52 OPERA,53 IDEA,54). A number of RCTs comparing bDMARD+MTX versus MTX monotherapy have incorporated a cross-over arm from MTX monotherapy to MTX+bDMARD combination therapy, providing further information on therapy with initial bDMARD+MTX versus step-up to bDMARD+MTX therapy (30 ,31 ,39 ,55). Several studies have also aimed to look at the use of bDMARD therapy in patients at earlier stages of inflammatory arthritis, presenting as UA or including patients that fulfil the 2010 ACR-EULAR RA,8 but not all fulfilling the 1987 ACR RA classification criteria7 (ADJUST,56 EMPIRE,57 IMPROVED,17 STREAM58).
Biological DMARD strategies studies without a treat-to-target approach—study outcomes
Biological DMARD strategy studies* with a treat-to-target approach—study outcomes
In essence, earlier improvement in signs and symptoms was seen with the more intensive strategies, however, outcomes were similar once bDMARDs were added in patients with insufficient response to MTX.16 ,18 ,50 ,59–61 Studies addressing the use of combination csDMARD therapy with MTX, SSZ+HCQ as step-up therapy in MTX-IR also reported similar clinical efficacy to step up bDMARD therapy.18 ,19 ,60 Low recruitment (and thus possibly insufficient power) was noted in several of these studies. Nevertheless, greater depth of response (higher proportions achieving ACR 70 responses (essentially equivalent to reaching low disease activity20) or remission, today's treatment goals) was seen with bDMARD therapy.52 ,53 ,62 Moreover, less radiographic progression and higher proportions of non-progression were noted with combination therapies that included a bDMARD,50 ,59 ,61 ,63 mainly due to early treatment effects.50 ,64 High proportions of clinical response rates and less radiographic progression were seen in studies using treat-to-target strategies, many of which also included glucocorticoids within their treatment strategies.52–54
Biological DMARD stopping or dose reduction
Eleven studies evaluated bDMARD stopping or bDMARD dose reduction after achieving low disease activity or remission.21 ,54 ,57 ,65–73 In DMARD-naive patients, the BeSt study reported that bDMARD discontinuation was possible but more likely in those receiving IFX+MTX as induction therapy compared to those receiving delayed IFX+MTX combination therapy (56% vs 29%, p=0.008 in the initial vs delayed groups, respectively.63 In the HIT HARD study, however, stopping ADA in an open label manner after ADA+MTX induction therapy for 6 months resulted in similar clinical outcomes to those on MTX monotherapy from the outset at 1 year (DAS28 :3.2±1.4 vs 3.4±1.6, p=0.41).21 In the OPTIMA study, a high proportion of patients who achieved low disease activity (LDAS28) at 6 months were able to maintain this outcome even after withdrawing the TNF-inhibitor. Maintenance, however, was somewhat higher in those continuing ADA compared to those who subsequently stopped bDMARD (18 month LDAS28: 91% vs 81% in the ADA-continue vs the ADA-stop groups, p=0.004, respectively).67 Studies have also addressed the possibility of dose reduction. In MTX-naive RA, the PRIZE study reported approximately two-thirds of early RA patients who achieved DAS28-remission (DAS28<2.6) after 1 year with ETN 50 mg weekly+MTX were able to maintain this response at 2 years with ETN 25 mg weekly+MTX (sustained DAS 28 remission (DAS28<2.6 at weeks 76 and 91 with no steroid boost): 23.1% vs 40% vs 63.5% in the placebo vs MTX monotherapy vs ETN 25 mg weekly+MTX groups, respectively).68 Thus, in this study, withdrawal of ETN was followed by a reduction in response in approximately 60% of the patients compared with ETN full dose continuation, while in OPTIMA, the reduction in targeted outcome was only about 10% following withdrawal of ADA. Maintenance of response in the majority of patients who reduced ETN dose was similarly shown in a MTX-IR group in the PRESERVE study69 after achieving LDAS28 at 9 months (DAS28 remission at 21 months was 35% vs 66% vs 71% with MTX continuation after ETN withdrawal vs ETN25 mg weekly+MTX vs ETN50 mg+MTX) and in studies in established RA (STRASS and DOSERA).72 ,73 (table 4)
Biological DMARD strategy studies addressing biological DMARD dose reduction or stopping—study outcomes
Biosimilar DMARDs
The PLANETRA study, was a phase 3 RCT comparing the bsDMARD CTP-13 to IFX demonstrating similar efficacy between the two treatment groups (ACR20 response at week 30 61% vs 59% (95% CI −6% to 10%) for CT-P13+MTX vs IFX+MTX, respectively).74 ACR50 and ACR70 responses were also similar with no significant between-group differences at 1 year75 (table 1).
Discussion
The increasing use of bDMARDs, particularly in different treatment strategies, as well as the introduction of newer therapies and emerging bsDMARDs, warranted a further review of the literature. The purpose of this SLR was to inform the update of the treatment recommendations being formulated by the EULAR Task Force.
This systematic literature review confirms the efficacy of bDMARDs particularly in combination with MTX. In the rather rare situation that patients treated with csDMARDs long-term may not tolerate MTX or another csDMARD, bDMARD monotherapy may be considered.23 ,50 ,51 However, with superior long-term clinical and superior radiographic outcomes, combination therapy with a bDMARD+a csDMARD remains the optimal approach.
This review also evaluated head-to-head bDMARD studies. These data, among other evidence, have important implications for clinical practice. While filling a gap in comparative studies, however, new challenges arise, particularly as several meta-analyses have shown similar efficacy among bDMARDs (except anakinra), and that bDMARD combinations with csDMARDs convey superior efficacy to bDMARD monotherapy.
This SLR also highlights the different study populations and designs employed and providing important new information when considering first-line bDMARD therapy. Studies addressing different treatment strategies have shown earlier improvement in signs and symptoms with a more intensive initial treatment approach, with similar clinical outcomes achieved upon addition of bDMARDs in patients with insufficient response to MTX compared with initial bDMARD use. Nevertheless, effects on radiographic progression tend to be superior with initial bDMARD use. Additionally, use of treat-to-target strategies has demonstrated high clinical and radiographic responses. Several studies have shown similar outcomes with initial combination csDMARD and step-up to combination csDMARDs compared to initial bDMARD therapy. Under-recruitment and methods of data analysis have been noted to be of concern in some16 ,18 ,19 and need to be taken into consideration when interpreting these findings as they may have potentially important impact on the study results.77
Although maintenance of low disease activity states is better with bDMARD continuation, there is some evidence for bDMARD dose reduction without loss of efficacy. With early bDMARD use, bDMARD and drug-free remission also seems more of a possibility. This highlights the need for more studies investigating the added benefit of initial induction therapy with a bDMARD compared to step-up to bDMARD following a csDMARD strategy. Related areas for research include the search for predictors of response to targeted therapies (which patient is likely to respond to which targeted therapy); the search for prognostic risk factors (eg, the presence of baseline radiographic erosions59) identifying those patients who may benefit most from a more intensive, initial bDMARD treatment strategy; and the search for predictive factors that permit successful drug withdrawal.21 ,68 ,78 ,79
This SLR confirmed that there is still an absence of RCT evidence-base to guide optimal approach when switching from one bDMARD to another after TNFi failure.
Since the last review, newer therapies have emerged with studies demonstrating efficacy of the IFX bsDMARD CT-P13 and the tsDMARD tofacitinib. Drug development in the area of bsDMARDs continues with several other agents on the horizon.80 ,81
Our literature review has its limitations. In particular, the inherent challenges in ensuring accurate interpretation when analysing heterogeneous studies is acknowledged. Although key clinical outcomes were addressed, other outcomes including the impact of bDMARDs on work ability was beyond the scope of this review. Standard definitions of disease activity states (eg, DAS28 ≤3.2 for LDA) have been used although more recent insights suggest that such patients may still have ongoing disease activity, highlighting the deficiencies of such measures. The SLR also focused solely on RCTs. While these are regarded as the highest level of evidence, they reflect a more selected patient population, making data less applicable to a real-life population. In this regard, non-randomised studies and evidence from real-life clinical practice (eg, national registries) provides valuable information that complements RCTs. Synthesis of data from both sources is needed for optimal application of evidence base into daily practice.
Safety is another aspect of bDMARD therapy that needs consideration. Given the importance of this aspect, this topic has been reviewed in a separate SLR.82 New evidence on the csDMARDs, glucocorticoid use as well as the tsDMARD has also been dealt with separately.83
In summary, review of the literature confirms the efficacy of bDMARDs, particularly in combination with a csDMARD, addresses their use in different treatment strategies with the potential for reduction in therapy particularly when early disease control is achieved and highlights new targeted and bsDMARDS in the treatment of RA. Finally, this review also identified some research agenda questions in the field of bDMARDs and RA which the updated EULAR recommendations5 will address.
Acknowledgments
The authors would like to thank Liz Neilly, University of Leeds, for help with the literature search; Liz Hensor, LIRMM University of Leeds and NIHR LMBRU Leeds Teaching Hospitals NHS Trust, for advice on the data and EULAR for funding support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Handling editor Francis Berenbaum
-
Contributors Each author has contributed to one or more of the following aspects of the manuscript—conception and design, acquisition, analysis and interpretation of data, drafting and revising the article.
-
Funding EULAR.
-
Competing interests These are summarised below as remuneration for consultation and/or speaking engagements (‘R’), research funding (‘F’) or ‘none’. JLN—R: UCB. SR—R: Fundação para a Ciência e Tecnologia. CGV—R: Abbvie, BMS, MSD, Pfizer, Roche-Chugai, UCB; F: Expanscience, Nordic Pharma, Pfizer. KT-none. ML-G- none; PE- R: MSD, Pfizer, Abbvie, Novartis, UCB, Roche, BMS, Lilly, Takeda, Janssen; F: MSD, Roche. LG—R: Abbvie, BMS, Chugai, Pfizer, Roche, UCB. RL—R: Abbott/AbbVie, Ablynx, Amgen, Astra-Zeneca, Bristol Myers Squibb, Centocor, Glaxo-Smith-Kline, Novartis, Merck, Pfizer, Roche, Schering-Plough, UCB, Wyeth; F: Abbott, Amgen, Centocor, Novartis, Pfizer, Roche, Schering-Plough, UCB, Wyeth. JSS—R: Abbott/Abbvie, Amgen, Astra-Zeneca, BMS, Celgene, Glaxo, Infinity, Janssen, Lilly, Medimmune, MSD, Novo-Nordisk, Pfizer, Roche, Samsung, Sandoz, Sanofi, UCB, Vertex; F: Abbott, BMS, MSD, Pfizer, Roche, UCB. MHB—R: Abbott/Abbvie, Bristol Myers-Squibb, Chugai, Pfizer, Roche; F: Pfizer.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Recommendation
- Clinical and epidemiological research
- Clinical and epidemiological research
- Correction