Article Text

Abstract
Objective We analysed the incidence of, the specific outcomes and factors associated with COVID-19-associated organ failure (AOF) in patients with systemic lupus erythematosus (SLE) in France.
Methods We performed a cohort study using the French national medical/administrative hospital database for the January 2011–November 2020 period. Each patient with SLE diagnosed in a French hospital with a COVID-19-AOF until November 2020 was randomly matched with five non-SLE patients with COVID-19-AOF. We performed an exact matching procedure taking age ±2 years, gender and comorbidities as matching variables. COVID-19-AOF was defined as the combination of at least one code of COVID-19 diagnosis with one code referring to an organ failure diagnosis.
Results From March to November 2020, 127 380 hospital stays in France matched the definition of COVID-19-AOF, out of which 196 corresponded with patients diagnosed with SLE. Based on the presence of comorbidities, we matched 908 non-SLE patients with COVID-19-AOF with 190 SLE patients with COVID-19-AOF. On day 30, 43 in-hospital deaths (22.6%) occurred in SLE patients with COVID-19-AOF vs 198 (21.8%) in matched non-SLE patients with COVID-19-AOF: HR 0.98 (0.71–1.34). Seventy-five patients in the SLE COVID-19-AOF group and 299 in the matched control group were followed up from day 30 to day 90. During this period, 19 in-hospital deaths occurred in the SLE group (25.3%) vs 46 (15.4%) in the matched control group; the HR associated with death occurring after COVID-19-AOF among patients with SLE was 1.83 (1.05–3.20).
Conclusions COVID-19-AOF is associated with a poor late-onset prognosis among patients with SLE.
- lupus erythematosus
- systemic
- COVID-19
- epidemiology
Data availability statement
Data are available upon reasonable request.
This article is made freely available for personal use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Key messages
What is already known about this subject?
The interplay between COVID-19 and systemic lupus erythematosus (SLE) has yet to be defined.
Currently available data regarding the impact of COVID-19 in SLE sound reassuring, but most studies are based on a small number of patients.
What does this study add?
In this nationwide cohort study, we found that patients with SLE had a poor late-onset prognosis after COVID-19-associated organ failure compared with a matched control population.
The HR associated with SLE for risk of death between day 30 and day 90 after the first day in the hospital for COVID-19-associated organ failure was 1.83 (1.05–3.20; p=0.03).
How might this impact on clinical practice or future developments?
Anti-SARS-CoV-2 vaccination among the SLE population appears to be a priority.
Introduction
The interplay between COVID-19 and systemic lupus erythematosus (SLE) has yet to be defined. Indeed, many patients with SLE are exposed to immunosuppressive drugs, are more susceptible to viral infections and often suffer from chronic kidney or cardiovascular diseases, which are additional risk factors for severe COVID-19.1 On the other hand, glucocorticoids and hydroxychloroquine, the drugs most widely used in SLE treatment, have also been investigated to treat COVID-19.2 3 Moreover, type 1 interferon (IFN) such as IFNα and the antibodies anti-IFNα are involved both in SLE and severe COVID-19.4–7 Although currently available data regarding the impact of COVID-19 in SLE sound reassuring,8–11 most studies are based on a small number of patients. Finally, comparison between SLE, which mainly affects women of childbearing age, and the general population with regard to severe COVID-19 may be challenging.
We used a French nationwide medical and administrative database to analyse the incidence, the specific outcomes and the characteristics associated with COVID-19-associated organ failure (COVID-19-AOF) in patients with SLE.
Methods
Study population and data source
Data of all patients admitted to French hospitals from January 2011 to November 2020 with at least one diagnosis of infection associated with an organ failure and/or SLE were collected from the national medical administrative database, the PMSI (Programme de Médicalisation des Systèmes d’Informations, Information System Medicalization Program). The PMSI database provides a summary with diagnosis and individual medical conditions at discharge of any public or private French healthcare facilities. Information covers both medical and administrative data. Each facility produces its own anonymous standardised set of data, which are then compiled at the national level. Even though these data are anonymous, the system allows to follow all hospital stays for each individual patient. Routinely collected medical data include, among other data, main diagnosis, secondary diagnoses and the procedures performed. Administrative data include, among other data, age, gender, year, duration of hospital stay and location of the hospital. In-hospital death is also reported. Diagnoses identified during the hospital stay are coded according to the International Classification of Diseases, 10th Revision (ICD-10). Procedures performed during the hospital stay are coded according to the ‘Classification Commune des Actes Médicaux’ (French Common Classification of Medical Procedures). Since 2004, each hospital’s budget depends on the medical activity described in this specific programme. Regular checks are made by the social insurance authority to ensure that data are correctly imputed. To select the SLE population, we first extracted from the PMSI database all records of patients for whom at least one ICD-10 M32 diagnosis was reported. We excluded patients younger than 15 years old and patients admitted to hospital only for scheduled sessions (chronic haemodialysis, radiotherapy, chemotherapy).
Definitions
We defined COVID-19-AOF as the combination of at least one of the diagnosis codes of COVID-19 (ICD-10 codes ‘U071’, ‘U0710’, ‘U0711’, ‘U0712’, ‘U0714’, ‘U0715’), with one code referring to an organ failure diagnosis (listed in online supplemental materials). This definition, which matches the definition for sepsis, has been previously used and validated in medical administrative database studies.12–14 To be allocated in the SLE group, COVID-19-AOF had to follow or be concomitant with an SLE ‘M32’ code. For an exhaustive description of diagnosis and procedure codes used, see online supplemental materials. To determine patients’ phenotype, we used all the specific diagnostic codes reported during or before the COVID-19-AOF stay.
Supplemental material
Matching procedure
Each patient with SLE who experienced COVID-19-AOF during the period of study was randomly matched with five non-SLE control patients with COVID-19-AOF and one patient with SLE without evidence of COVID-19 infection. We used a random exact matching procedure (without replacement) using the following matching variables: age ±2 years, gender, chronic kidney disease, arterial hypertension, cardiovascular history, diabetes mellitus, chronic pulmonary disease and obesity. We verified matching accuracy and efficacy by calculating the standardised differences for the matching variables between the various matched populations.
Survival analysis
Kaplan-Meier method was used to present 90-day survival, taking day 0 as the first hospital admission for COVID-19-AOF. For the control SLE non-COVID-19 population, we used the first day of a randomly selected stay before 2020 (2011–2020 period) as day 0.
In order to calculate the HR of death after COVID-19-AOF according to SLE status, and because we cannot assume the proportional hazard hypothesis for the whole period between day 0 (D0) and day 90 (D90), we split this period into two parts: D0–D30 and D30–D90. For the second time period, we considered only the subgroups of patients who survived after 30 days of follow-up, taking D30 as the new day 0. We used standard univariable Cox proportional hazard model for the unmatched analysis and univariable marginal Cox proportional hazard model15 for the postmatching analysis.
Statistical statement
Categorical variables are presented as number (percentage). Quantitative variables are presented as median (first quartile–third quartile). HRs are presented with their 95% CI. We used Student’s t-test and χ2 test for univariable comparisons, as appropriate. All analyses were performed using SAS V.9.4 software. Kaplan-Meier curves were built with R V.4.0.3 software.
Results
Characteristics of patients with SLE experiencing COVID-19-AOF
From March to November 2020, 127 380 hospital stays in France matched the definition of COVID-19-AOF. Among them, there were 196 unique patients with SLE and 113 567 unique patients without SLE. A flow chart of these selected populations is presented in online supplemental figure S1. A comparison of SLE patients with COVID-19-AOF versus non-SLE patients with COVID-19-AOF is presented in table 1. The characteristics of patients with SLE admitted to hospital within the study period but without any evidence of COVID-19 are also presented for information. Briefly, SLE patients with COVID-19-AOF were younger (65 (52–76) years vs 76 (64–86) years; p<0.0001), less frequently male (n=50 (25.5%) vs n=56 601 (57.8%); p<0.0001) and had more comorbidities than the general population with COVID-19-AOF. Patients with SLE were also more frequently admitted to the intensive care unit (ICU) (n=83 (42.4%) vs n=40 304 (35.6%); p=0.04) and underwent more often renal replacement therapy for acute kidney injury (AKI; n=14 (7.1%) vs n=3744 (3.3%); p=0.003).

Survival at D90 of patients with SLE experiencing COVID-19-AOF in France (in red) from March 2020 to November 2020 compared with an unmatched control population without SLE (in blue) with COVID-19-AOF during the same period. For information, the survival of an unmatched SLE population admitted in France during the same period without any evidence of COVID-19 is shown in green. P value is given for the time periods D0–D30 and D30–D90 for comparison between SLE patients with COVID-19-AOF and non-SLE patients with COVID-19-AOF. AOF, associated organ failure; D, day; SLE, systemic lupus erythematosus.
Characteristics of patients with and without SLE experiencing COVID-19-AOF from March to November 2020 in France
Crude analysis of 30-day and 90-day survival of patients with SLE experiencing COVID-19-AOF
At D30, 43 (21.9%) in-hospital deaths occurred among SLE patients with COVID-19-AOF vs 31 274 (27.6 %) in the unmatched non-SLE patients with COVID-19-AOF. In the D0–D30 period, the HR of death associated with presence of SLE was 0.69 (0.51–0.93). At D90, there was no perceptible difference regarding in-hospital mortality between both groups: 59 deaths (30.1%) in the SLE group vs 35 130 (30.9%) in the control group. In the D30–D90 period, the HR of death associated with presence of SLE was 1.52 (0.93–2.47). A sensitivity analysis using Cox model adjusted for age and sex is presented in online supplemental figure S6.
The Kaplan-Meier curve of the 90-day survival of these populations is displayed in figure 1. The survival of an unmatched SLE population without any evidence of COVID-19 is also displayed for information.
Postmatching analysis of 30-day and 90-day survival of patients with SLE experiencing COVID-19-AOF
Based on the presence of comorbidities, we were able to match 908 non-SLE patients with COVID-19-AOF and 170 SLE patients without COVID-19 with 190 SLE patients with COVID-19-AOF.
The characteristics of these matched populations as well as the standardised differences for the matching variables are displayed in table 2. The rate of ICU admission was similar between patients with SLE and matched patients without SLE experiencing COVID-19-AOF: n=82 (43.2%) in the SLE group vs n=242 (43.3%) in the non-SLE matched control group.
Characteristics of matched patients with and without SLE experiencing COVID-19-SLE from March to November 2020 in France
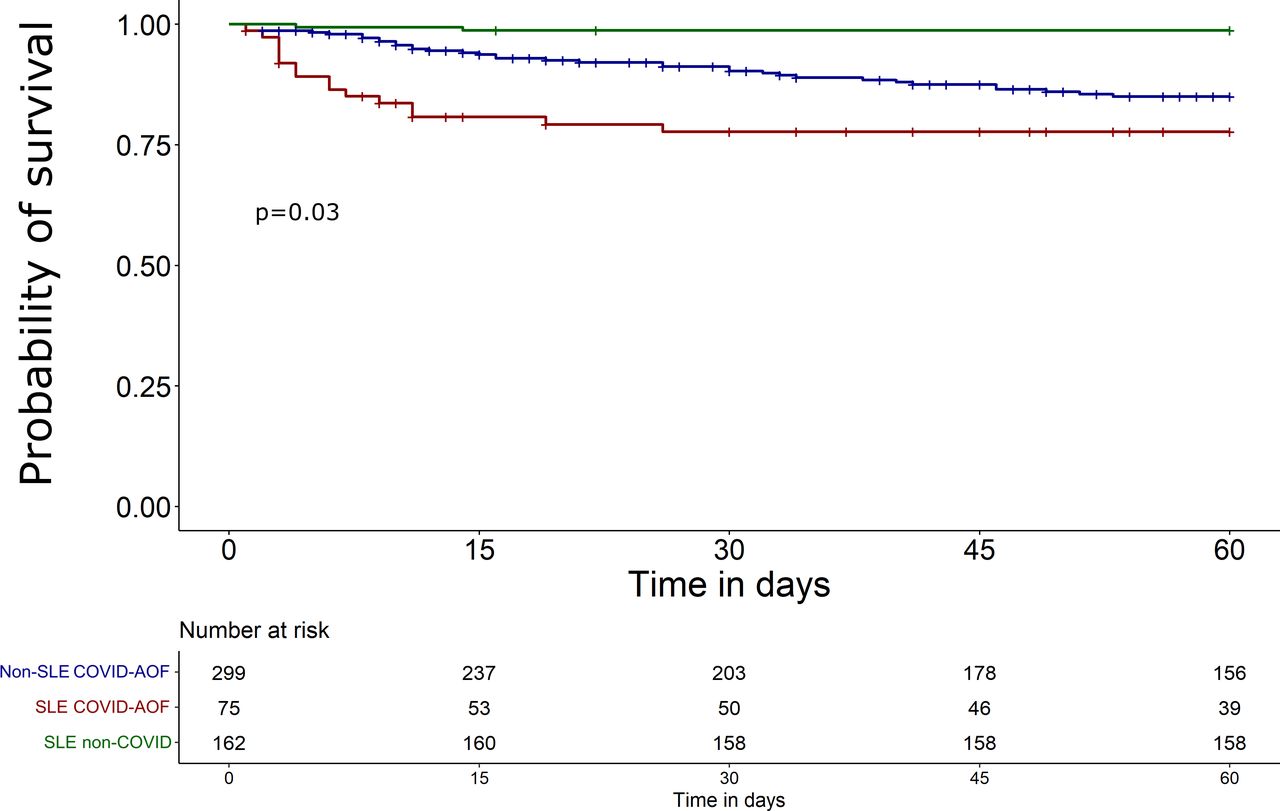
The Kaplan-Meier curve of the 90-day survival of these matched populations is displayed in figure 2. More details about the type of discharge after hospital stay following COVID-19-AOF are provided in online supplemental figure S3.

Survival at D90 of patients with SLE experiencing COVID-19-AOF in France (in red) from March 2020 to November 2020 compared with a matched control population (in blue) with COVID-19-AOF but without SLE admitted during the same period. For information, survival of a matched SLE population admitted in France during the same period without any evidence of COVID-19 is shown in green. P value is given for the time period D0–D30 for comparison between SLE patients with COVID-19-AOF and non-SLE patients with COVID-19-AOF. AOF, associated organ failure; D, day; SLE, systemic lupus erythematosus.

{kind=link}
{kind=link}
{kind=link}
D30–D90 survival of patients still alive at D30. Patients with SLE experiencing COVID-19-AOF in France from March 2020 to November 2020 (in red) compared with a matched control population without SLE (in blue) with COVID-19-AOF during the same period. For information, survival of a matched SLE population admitted in France during the same period without any evidence of COVID-19 is shown in green. P value is given for comparison between SLE patients with COVID-19-AOF and non-SLE patients with COVID-19-AOF. AOF, associated organ failure; D, day; SLE, systemic lupus erythematosus.
At D30, 43 deaths (22.6%) were observed within SLE patients with COVID-19-AOF vs 198 (21.8%) within the matched non-SLE patients with COVID-19-AOF. The HR of death associated with presence of SLE for this period was 0.98 (0.71–1.34).
A follow-up from D30 to D90 was possible for 75 SLE patients with COVID-19-AOF and 299 non-SLE patients with COVID-19-AOF. A comparison of their baseline features as well as detailed data of their follow-up is available in online supplemental figures S3–S4. The Kaplan-Meier curve of their D30–D90 survival is displayed in figure 3. During this period, we observed 19 deaths in the SLE group (25.3%) and 46 (15.4%) in the matched control group. The HR for death occurring from day 30 to day 90 after COVID-19-AOF among patients with SLE was 1.83 (1.05–3.20). A sensitivity analysis using a rematch procedure for patients still alive at D30 is presented in online supplemental figure S7–S8.
All HRs calculated for the crude and the matched analyses are summarised in table 3.
Summary of the main results of the study
Healthcare use after COVID-19-AOF
Analysis of healthcare use post COVID-19-AOF for the matched population still alive at D30 is presented in online supplemental figure S5. We observed that patients with SLE had more reports of coinfection diagnoses than the matched control patients (mean (±SD): 9.09 (±8.5) in the SLE group vs 7.6 (±6.1) in the control group). Otherwise, we found no difference in the number of SLE-related outcomes such as renal biopsy or dialysis for AKI. Similarly, we found no difference in unspecific outcomes such as number of hospital stays, diagnosis of pulmonary embolism or coronary angiography for myocardial infarction.
Discussion
Our analysis of the French national medical and administrative database showed that SLE is associated with a worsened prognosis during COVID-19-AOF requiring hospitalisation. Importantly, we observed an increased late-onset mortality, between D30 and D90, for hospitalised patients with SLE still alive 30 days after the first day of admission, independently of age, gender and various comorbidities such as chronic kidney disease.
Conversely, in our selected unmatched population, the crude analysis of the COVID-19-AOF outcome showed that hospitalised patients with SLE have an unchanged prognosis as compared with the general population. Such observation may be biased because patients with SLE are younger and more frequently female. On the other hand, patients with SLE have more comorbidities.16 Using a matching strategy that was devised to limit such biases, a specific delayed risk was unravelled in hospitalised SLE patients with COVID-19-AOF. Such increased risk might be related to the high coinfection rate during or after COVID-19 in these patients. Patients with SLE could be more susceptible to coinfection due to their treatment. They may also be at risk of COVID-19-induced immune paralysis. Of note, SLE flares or cardiovascular events rates did not seem to be increased after COVID-19-AOF. Since we did not have access to patients’ detailed files and treatments, we were not able to confirm that SLE disease went uneventful.
Several studies have assessed the specific prognosis of patients with SLE during COVID-19 and displayed heterogenous results.8 9 17–20 Most studies analysed a mixed subset with various rheumatic diseases and included a very limited number of patients with SLE. Moreover, no matching strategy was used to limit the bias related to age, sex and comorbidities among the SLE population.
We found a relatively low number of patients with SLE among the French population with COVID-19-AOF (196 of 113 371, 0.2%) between March and November 2020, whereas Cordtz et al 21 recently reported an increased risk of hospitalisation for SLE patients with COVID-19 in Denmark compared with the general population. It might be due to a lack of precision in coding SLE procedures; however, our results fit well with the prevalence of SLE in France, estimated at 5 for 10 000.22 Moreover, the characteristics of our patients with SLE are consistent with previously published large epidemiological studies on patients with SLE conducted in France.22
Because it is a hospital database, we only had access to in-hospital mortality. Since patients with SLE are more likely to be admitted to hospital, the proportion of in-hospital mortality for patients with SLE is expected to be higher than for the general population. However, we found that most of the patients discharged before D90 went home; therefore, we can assume that a very limited number of them died after discharge. Follow-up was limited to 90 days after COVID-19, with data gathered before November 2020; thus, the investigated population encountered almost exclusively the original ‘Wuhan’ SARS-CoV-2 strain.
Our work has several strengths. First, in accordance with the French Health Insurance System, PMSI gather exhaustive data of all French hospitals, meaning that our data included every patient with at least one diagnosis of SLE reported from 2011 to 2020. Thanks to linking between the successive hospitalisation episodes, we were able to examine all hospital records of each individual patient and to assess 30-day and 90-day outcomes. Our matched study allowed us to take into account several confounding factors that usually blur the comparison between patients with SLE and the general population. Although the severity of COVID-19-AOF was not included in the matching procedure, we observed a very similar rate of ICU admission, Simplified Acute Physiology Score II and healthcare use between patients with SLE and the matched control population, confirming the validity of the matching process.
COVID-19-AOF has a late-onset poor prognosis in patients with SLE. Further studies are warranted to delineate the clinical course of patients with SLE who survived severe COVID-19.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
In accordance with the French regulatory system regarding personal and medical data and after agreement of the institutional review board (IRB), our institution was allowed to access the PMSI database. We only had access to patients diagnosed with infection-associated organ failure and/or SLE according to our definition. All data were anonymised. This study does not involve human participants.
Acknowledgments
The authors thank Celine Feger, MD (EMIBiotech) for her editorial support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Contributors AM designed and conducted the analysis and wrote the manuscript. TP, SR, DvG, AS and KS were involved in the project development and edited the manuscript. J-FT directed the project and wrote the manuscript. AM is the guarantor of this study.
Funding PhD fellowship support for AM was provided by Agence Nationale pour la recherche (n°ANR-19-CE17-0029).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.