Article Text

Abstract
Objectives To evaluate the distinct impact of disease modifying antirheumatic drugs (DMARD) combination and monotherapy in immune response to an inactivated SARS-CoV-2 vaccine in patients with rheumatoid arthritis (RA).
Methods This phase 4 prospective study analysed seroconversion (SC) of anti-SARS-CoV-2 immunoglobulin G (IgG) and neutralising antibodies (NAb) induced by the inactivated vaccine (CoronaVac) in patients with RA in comparison to controls (CG). Disease activity and treatment were also assessed. Only participants with baseline negative IgG/NAb were included.
Results Patients with RA (N=260) and CG (N=104) had comparable median ages (59 years (50–65 years) vs 58 years (49.8–64 years), p=0.483). Patients with RA had moderate but lower SC (61.8% vs 94.2%, p<0.001) and NAb positivity (45% vs 78.6%, p<0.001) in comparison to CG after full vaccination. Baseline disease activity did not influence immunogenicity (p>0.05). After multivariate analyses, factors independently related to reduced SC were: older age (OR=0.79 (0.70–0.89) for each 5-year interval, p<0.001), methotrexate (OR=0.54 (0.29–0.98), p=0.044), abatacept (OR=0.37 (0.19–0.73), p=0.004) and number of DMARD (OR=0.55 (0.33–0.90), p=0.018). Regarding NAb, age (OR=0.87 (0.78–0.96) for each 5-year interval, p=0.007) and prednisone >7.5 mg/day (OR=0.38 (0.19–0.74), p=0.004) were negatively related to the presence of NAb. Further comparison of SC/NAb positivity among RA treatment subgroups and CG revealed that methotrexate/tofacitinib/abatacept/tocilizumab use, in monotherapy or in combination, resulted in lower responses (p<0.05), while tumour necrosis factor inhibitor and other conventional synthetic DMARD interfered solely when combined with other therapies.
Conclusions Patients with RA under DMARD have a moderate immunogenicity to CoronaVac. We identified that nearly all DMARD combinations have a deleterious effect in immunogenicity, whereas a more restricted number of drugs (methotrexate/tofacitinib/abatacept/tocilizumab) also hampered this response as monotherapy. These findings reinforce the need of a broader approach, not limited to specific drugs, to improve vaccine response for this population.
Trial registration details NCT04754698.
- Arthritis
- Rheumatoid
- Covid-19
- vaccination
- biological therapy
- therapeutics
Data availability statement
All data relevant to the study are included in the article. Not applicable.
This article is made freely available for personal use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Key messages
What is already known about this subject?
There is increasing evidence of the effect of rituximab, methotrexate, abatacept and corticosteroids on COVID-19 vaccine immunogenicity in overall autoimmune rheumatic diseases cohorts.
What does this study add?
This is the first study to focus, exclusively in rheumatoid arthritis population, the impact of the different therapies and its combinations on the immunogenicity induced by the inactivated Sinovac-CoronaVac vaccine.
We provided novel evidence of an overall reduced anti-SARS-CoV2 S1/S2 immunoglobulin G and neutralising antibodies responses for nearly all drugs used in different combinations and, for methotrexate, tofacitinib, abatacept and tocilizumab also in monotherapy.
A cut-off point of 7.5 mg/day of prednisone was identified as deleterious for immunogenicity.
The humoral response was not influenced by disease activity status at the time of vaccination.
How might this impact on clinical practice or future developments?
Our findings show an overall deleterious effect of nearly all DMARD, either in monotherapy or in combination, reinforcing the need of a broader strategy, not limited to individual drugs, to improve vaccine response for this population which might include drug temporary discontinuation or booster doses.
Introduction
The COVID-19 has proven to be a major threat to individuals worldwide.1 Patients with rheumatoid arthritis (RA), one of the most common autoimmune rheumatic diseases (ARD),2 are at a high risk of severe COVID-19 outcomes,3–5 especially those with active disease, under immunosuppressive therapies, or with comorbidities.5 6 In this context, mass vaccination is the main measure to control the pandemic.
The Sinovac-CoronaVac inactivated vaccine7 8 has been one of the most widely used in the world, with an efficacy of 83.5% in reducing infections, according to the phase 3 trial.9 Its effectiveness was demonstrated in Chile (10.2 million people studied), with a reduction of 87.5% in hospitalisation, 90.3% in intensive care unit admission and 86.3% for death.10 Recently, an appropriate, but reduced, immune response with Sinovac-CoronaVac vaccine was described in a large population of overall patients with ARD.11 Similarly, previous reports assessed safety and immunogenicity of other anti-SARS-CoV-2 vaccines, such as messenger RNA (mRNA) and viral vector vaccines, and demonstrated safety and lower, but adequate, immunogenicity, also in overall ARD populations.12–22 Regardless of vaccine type, glucocorticoids,11 14 21 22 rituximab,11 13–16 20 21 methotrexate (MTX),11 14 17 18 22 mycophenolate mofetil11 13–15 21 and abatacept11 14 15 21 have deleterious effects in immunogenicity.
None of these previous reports, however, focused specifically on patients with RA and the several combinations of distinct disease modifying antirheumatic drugs (DMARD) that they use. The only study to focus on such population was underpowered to show differences among treatments.23 The small sample size of some drugs subgroups in monotherapy or combination in these studies and the scarce data on conventional synthetic DMARD (csDMARD) other than MTX precluded a definitive conclusion regarding the effect of these drugs on COVID-19 vaccine immunogenicity in the RA population.11–23 The cut-off dose in which prednisone hampers vaccine-induced antibody response in patients with RA also needs to be established.
Therefore, the aim of the present study was to assess the impact of distinct DMARD, used in combination or in monotherapy, in the immunogenicity to Sinovac-CoronaVac vaccine in patients with RA, compared with age-balanced and sex-balanced controls. We also evaluated the safety and the influence of disease activity on immune response.
Methods
Study design and participants
This was a subanalysis of a prospective, single centre, controlled phase 4 study (CoronavRheum, clinicaltrials.gov) that evaluated the immunogenicity/safety of Sinovac-CoronaVac vaccine in patients with ARD,11 regularly followed at the Outpatient Clinics of Rheumatology Division (Hospital das Clinicas HCFMUSP, Faculdade de Medicina, Universidade de Sao Paulo, Brazil). For the original study,11 adult (age: ≥18 years old) patients with ARD were invited to participate after their electronic chart review of the last 3 months (recruitment up to 3 weeks before enrolment). Subsequently, a control group (CG) was invited, including subjects without ARD among the maintenance/administrative hospital workers and relatives, with comparable sex and age to the overall ARD sample. For the current analysis, all patients with RA,24 were included and, subsequently, a CG was randomly selected using an Excel programme (5 patients with RA to 2 controls), with comparable sex frequencies and ages (≤5-year difference).
Exclusion criteria were acute febrile illness/symptoms of COVID-19 at vaccination, history of anaphylaxis to vaccine components, demyelinating disease, decompensated heart failure (class III/IV), blood transfusion ≤6 months, inactivated virus vaccine ≤14 days, live virus vaccine ≤4 weeks, denial to participate, hospitalisation, previous vaccination with SARS-CoV-2 vaccine, rituximab therapy ≤12 months and prevaccination positive COVID-19 serology (anti-S1/S2 immunoglobulin G (IgG) and/or neutralising antibody (NAb)).
Patients and the public were not involved in the design, conduct, reporting or dissemination plans of the present research.
Vaccination protocol
The vaccination protocol included two doses of ready-to-use syringes with Sinovac-CoronaVac vaccine (Sinovac Life Sciences, Beijing, China, batch # 20200412),7 8 containing 3 µg (0.5 mL) of β-propiolactone inactivated SARS-CoV-2 with aluminium hydroxide adjuvant, administered in the deltoid muscle. First dose was on 9–10 February 2021 (D0) and second dose on 9–10 March 2021 (D28), for both patients with RA and CG. Participants with suspicious COVID-19 were instructed to undergo a reverse transcriptase PCR (RT-PCR) test for SARS-CoV-2 in naso/oropharyngeal swabs, available at the hospital. Those with RT-PCR confirmed COVID-19 between doses were excluded from the immunogenicity analyses and received the second dose 4 weeks after the first symptoms.
Immunogenicity outcomes
Blood samples (20 mL) were collected immediately before each vaccine dose and 6 weeks after the last dose (D69) on 19 April 2021. Sera were stored at −70°C. The two co-primary outcomes were IgG seroconversion (SC) to anti-SARS-CoV-2 S1/S2 proteins and the presence of NAb at D69. Secondary outcomes were SC and the presence of NAb at D28, geometric mean titres (GMT) of anti-S1/S2 IgG and their factor increase in GMT (FI-GMT), and neutralising activity of NAb, also at D28 and D69.
IgG antibodies against the SARS-CoV-2 S1/S2 proteins were checked by a chemiluminescent immunoassay (Indirect ELISA, LIAISON, DiaSorin, Italy). SC was defined as positive serology (≥15.0 UA/mL).25 26 GMT (95% CIs) were calculated, attributing the value of 1.9 UA/mL to undetectable levels (<3.8 UA/mL). FI-GMT is the ratio of the GMT after vaccination to the GMT before vaccination.
Circulating NAb were detected by the SARS-CoV-2 sVNT Kit (GenScript, Piscataway, New Jersey, USA). Positivity was defined as ≥30% inhibition of the linkage between the receptor-binding domain of the viral spike glycoprotein with the ACE2 cell surface receptor.27 Medians (IQR) of the percentage of neutralising activity were only calculated for positive samples.
Vaccine adverse events
After each vaccine dose, participants (RA and CG) received a standardised diary to record prospectively local and systemic manifestations (online supplemental figure 1). These diaries were checked at the next evaluation. Additionally, participants were instructed to inform any moderate/severe adverse events (AE) after each vaccine dose (by telephone, smartphone instant messaging or email). AE severity was classified according to WHO definition (WHO 2021),.28
Supplemental material
Medication and disease activity
Data regarding demography, disease characteristics/activity, medications and comorbidities of patients with RA were assessed by electronic chart review. Patients were not instructed to hold medications before or after vaccination, since ACR guidelines first version was uploaded on 8 February 2021, 1 day before the first vaccine dose (D0), with no time to submit changes in vaccination protocol to the ethics committee.29 Patients were asked about their subjective perception of disease activity worsening after each vaccine dose.
Statistical analysis
The sample size calculation was based on the 24% reduction of SC after vaccination with the 2009 non-adjuvanted influenza A/H1N1 vaccine in patients with RA.30 Expecting SC rates of 53% in patients and 77% in CG, with a 5% α error and 80% power (5:2 ratio), the minimum sample would be 110 patients with RA and 44 healthy subjects.
Categorical variables were presented as number (percentage) and compared using χ2 or Fisher’s exact tests, as appropriated. Continuous general data were presented as medians (IQRs) and compared using Mann-Whitney U test (two groups) or Kruskal-Wallis one-way analysis of variance on ranks (more than two groups). Only for patients with RA, multivariate logistic regression analyses were performed with SC or the presence of NAb at D69 as dependent variables, and variables with p<0.2 in each univariate analysis as independent variables. Subgroup analyses, including only patients with no DMARD or in DMARD monotherapy, were also performed with the same parameters. Comparisons of IgG titres were assessed as Napierian logarithm (ln) transformed data, using generalised estimating equations (GEE) with normal marginal distribution and gamma distribution, respectively, and identity binding function, assuming first-order autoregressive correlation matrix between moments, followed by Bonferroni’s multiple comparisons to identify differences between groups (overall patients with RA and CG) and time points (D0, D28 and D69). Statistical significance was defined as p<0.05. All statistical analyses were performed using SPSS, V.20.0 (IBM-SPSS for Windows V.20.0).
Results
A total of 424 patients with RA and 542 controls were invited. After exclusion criteria, 279 seronegative patients with RA and 301 controls composed the final samples (figure 1). They were age balanced and sex balanced in a 5:2 ratio, and, finally, 260 patients with RA and 104 controls comprised the final comparison groups (figure 1, table 1). Most participants (n=339, 93.1%) were vaccinated on 9–10 February 2021, without differences between groups (91.5% vs 97.1%, p=0.07). Participants who could not attend on such days had up to 15 days for enrolment and vaccination.

Modified CONSORT flow diagram. CONSORT, Consolidated Standards of Reporting Trials; IgG, immunoglobulin G; RT-PCR, reverse transcriptase PCR.
Baseline characteristics of patients with RA and CG, all with negative anti-S1/S2 IgG serology and NAb at baseline
Immunogenicity outcomes in patients with RA compared with CG
From the matched sample, 9 (3.5%) patients with RA and 1 (1%) control (p=0.293) were additionally excluded due to RT-PCR-confirmed COVID-19 during follow-up. Compared with controls, patients with RA had lower frequencies of SC and the presence of NAb, and lower GMT and neutralising activity at D69 (table 2, figure 2).
Data regarding anti-S1/S2 IgG (SC rates, anti-SARS-CoV-2 S1/S2 IgG titres and FI in titres, and frequency of NAb) and median percentage of neutralising activity in patients with RA and CG after the first (D28) and second (D69) doses of CoronaVac vaccine

Box plots of ln-transformed IgG titres over time in patients with RA (n=251) and controls (CG, n=103). Data were analysed in ln-transformed data using GEE with normal marginal distribution and gamma distribution, respectively, and identity binding function assuming first-order autoregressive correlation matrix between moments (D0, D28 and D69) in the comparison of the 2 groups (RA vs CG), followed by Bonferroni’s multiple comparisons. Tests were two-sided. RA and CG were comparable only at D0 (P > 0.999). The mean behaviour of the ln-transformed IgG titres was different in RA and CG groups at D28 (*p<0.001) and D69 (*p<0.001). Mean titres increased at each time point for RA and CG (†p<0.001). Dotted line denotes the cut-off level for positivity (ln 15 AU/mL=2.71 by indirect ELISA, LIAISON SARS-CoV-2 S1/S2 IgG). CG, control group; GEE, generalised estimating equations; IgG, immunoglobulin G; ln, logarithm; RA, rheumatoid arthritis
Assessment of factors associated with immunogenicity in patients with RA
Among the original 279 patients with RA, we analysed 266 (4 patients did not collect the last sample and 9 had COVID-19 during follow-up). Univariate and multivariate analyses pointed the following factors as negatively associated to SC: older age, number of DMARD, MTX and abatacept. Sulfasalazine was positively associated with SC only in univariate analyses (table 3). Regarding NAb, age and prednisone dose ≥7.5 mg/day were negatively related to the presence of NAb in univariate and multivariate analyses (table 3).
Unadjusted and adjusted logistic regression models examining the factors associated with positive anti-S1/S2 IgG antibodies and NAb after two doses of CoronaVac (at D69) in 266 patients with RA
Assessment of factors associated with immunogenicity in patients with RA without combination therapy
A subgroup analysis, including only patients with no DMARD or in DMARD monotherapy, was performed and pointed older age and abatacept use as negatively associated to SC (table 4), while prednisone use in a dose ≥7.5 mg/day was related to the absence of NAb (table 4).
Unadjusted and adjusted logistic regression models examining the factors associated with positive anti-S1/S2 IgG antibodies and NAb after 2 doses of CoronaVac (at D69) in 71 patients with RA under any DMARD monotherapy (n=64) or without DMARD (n=7)
Direct comparisons of patients under distinct DMARD combinations with the original CG
Direct assessments of subgroups of patients under distinct treatments with the original CG were performed at D69 (online supplemental tables 1 and 2; figures 3 and 4). For each subgroup assessed, age and sex distribution persisted comparable to CG (p>0.05), except for those under ‘other csDMARD’ (sulfasalazine) in monotherapy (online supplemental table 1). Disease activity was similar among major groups (p>0.05) (online supplemental table 3). Lower SC and the presence of NAb rates were observed among patients under MTX, abatacept and tocilizumab, both in monotherapy and in combination with other drugs. Patients under non-MTX-csDMARD and tumour necrosis factor inhibitor (TNFi) had decreased rates only in combination with other therapies. Tofacitinib use, alone or in combination, impacted on NAb presence (online supplemental table 1; figure 3). Most patients with RA under any DMARD (alone or in combination) had lower GMT than CG (figure 4; online supplemental table 4).
Supplemental material
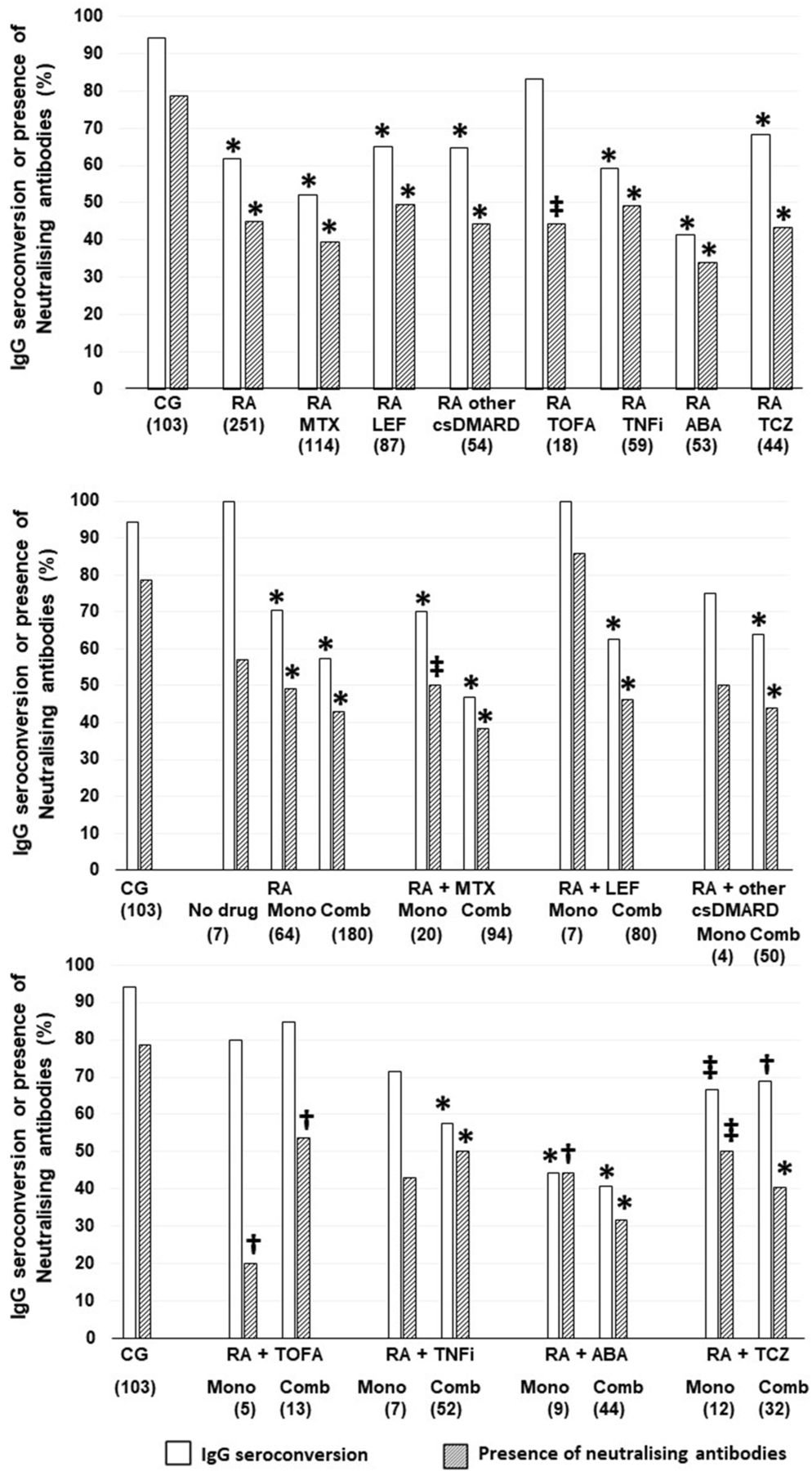
Anti-SARS-CoV-2 S1/S2 IgG SC and the presence of NAb at D69, according to RA treatments in comparison to CG, using a two-sided χ2 or Fisher’s exact tests, as appropriate. All the analyses are two-sided. Data are shown as percentages. The number of patients in groups is depicted under their designations. ABA, abatacept; CG, control group; Comb, combination therapy; csDMARD, conventional synthetic disease modifying antirheumatic drugs; DMARD, disease modifying antirheumatic drugs; IgG, immunoglobulin G; LEF, leflunomide; Mono, monotherapy; MTX, methotrexate; NAb, neutralising antibodies; RA, rheumatoid arthritis; TCZ, tocilizumab; TNFi, tumour necrosis factor inhibitor; TOFA, tofacitinib. Other csDMARD: sulfasalazine (n=29) or hydroxychloroquine (n=25). *p<0.001 vs CG; †p<0.05 vs CG; ‡p<0.01 vs CG.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Box plots show Napierian ln-transformed anti-SARS-CoV-2 S1/S2 IgG titres at D69, according to RA treatments in comparison to CG, using the Mann-Whitney U test. Analyses were two-sided. Dotted line denotes the cut-off level for positivity (ln 15 AU/mL=2.71 by Indirect ELISA, LIAISON SARS-CoV-2 S1/S2 IgG). The number of patients in groups is depicted under their designations. ABA, abatacept; CG, control group; Comb, combination therapy; csDMARD, conventional synthetic disease modifying antirheumatic drugs; DMARD, disease modifying antirheumatic drugs; LEF, leflunomide; ln, logarithm; Mono, monotherapy; MTX, methotrexate; RA, rheumatoid arthritis; TCZ, tocilizumab; TNFi, tumour necrosis factor inhibitor; TOFA, tofacitinib. Other csDMARD: sulfasalazine (n=29) or hydroxicloroquine (n=25). *p<0.001 vs CG; †p<0.05 vs CG; ‡p<0.01 vs CG.
Vaccine tolerance and safety
No moderate or severe AE was reported. After the first dose, patients had more overall and systemic reactions, headache and arthralgia, than CG (online supplemental table 4). After the second dose, no difference was observed. After first vaccine dose, 11 patients (4.2%) reported worsening of disease activity perception, while 14 (5.6%) reported after the second shot.
Discussion
To the best of our knowledge, this is the first study to focus on the impact of the different therapies and its combinations, exclusively in patients with RA, on the immunogenicity induced by inactivated Sinovac-CoronaVac vaccine. This detailed analysis provided novel evidence of an overall reduced immune response in many different combinations, and, in monotherapy, for abatacept, MTX, tocilizumab and tofacitinib.
The main strength of this study is the inclusion of a robust RA population under representative distribution of different drug categories, allowing a precise analysis of the influence of specific mechanisms on humoral response, even in monotherapy. Inclusion of a paired CG was also essential to avoid the well-known effects of age and sex on vaccine immunogenicity.31 32 Moreover, disease activity was evaluated by validated scores. The isolated analysis of patients with RA prevented interference from drugs not commonly used in RA in the regression models. We also deliberately avoided patients under rituximab because of its well-known influence on humoral immunogenicity and heterogeneous phases of the cycles at the vaccination period.11 13–15 17 20 21 30 Furthermore, immunogenicity was assessed by two validated methods.25–27 In this context, anti-SARS-CoV-2 S1/S2 IgG was used in other large trials of COVID-19 vaccination in patients with ARD.14 22 Although higher titres of NAb were associated to increased COVID-19 protection,33 34 further prospective studies with continuous disease surveillance are necessary to better evaluate possible cut-off levels and persistence of protection.
Among csDMARD, virtually any combination therapy was associated with decreased responses for both IgG and NAb. Although 62.5% of these combinations included MTX, other associated csDMARD also reduced immunogenicity when in combination with biologic DMARD (bDMARD) or other sDMARD. In fact, the number of DMARD was independently related to reduced SC in a similar magnitude to MTX (45% decrease). These novel findings of reduced immunogenicity with non-MTX-csDMARD associations were not appropriately evaluated in other studies due to the small sample size of subgroups of patients using such combinations.12–23
Of note, in monotherapy, MTX was the only csDMARD associated with reduced response both to IgG and NAb in comparison to controls. Although Braun-Moscovici et al 15 suggested that impairment of the humoral response might be attributed to the concomitant treatment, our findings point that this also occurs with MTX monotherapy at a lesser degree. This result reinforces those findings with other COVID-19 vaccines.14 17–19 22 Interestingly, tofacitinib, alone or in combination, had a negative impact mainly on NAb, but also in IgG GMT, which is in line with previous findings about the BNT162b2 mRNA14 and anti-pneumococcal vaccines.35 We reinforce that non-MTX csDMARD in monotherapy (leflunomide and sulfasalazine) had no negative impact on immunogenicity, and this is probably a subgroup of patients who do not need drug discontinuation, as observed in studies with other COVID-1920 22 and influenza30 36 vaccines. However, the small representation in monotherapy of these drugs precludes a definitive conclusion.
Regarding the role of biological therapies, any combination with bDMARD was deleterious. This finding extended previous results on relevance of combination therapy as the main cause of poor vaccine response.14 15 Regarding abatacept, it was the drug with the greatest impact on immunogenicity herein: IgG SC rate and NAb positivity were, respectively, limited to 25% and 20% of patients under abatacept in combination with MTX. This fact is in accordance with previous findings of up to 90% reduction of anti-SARS-CoV-2 IgG response to the BNT162b2 mRNA vaccine, especially in combination with MTX.14 15 22 We extended these observations, demonstrating a harmful effect of abatacept in combination with other csDMARD and in monotherapy. Specifically, the exclusive evaluation of patients without combination therapy highlighted abatacept as related to vaccine non-response, even in monotherapy, in comparison to other DMARD. The impact of abatacept on vaccination confirms previous evidence from influenza A/H1N1,36–38 and pneumococcal conjugate vaccines,39 probably due to the attenuation of co-stimulating signal of naïve T cells, inhibition of T cell proliferation, and inadequate stimulation of B cells.40 41
Other bDMARD, TNFi and tocilizumab, also decreased SC, GMT and NAb responses, in combination not only with MTX but also with other csDMARD, adding information to previous data with other COVID-19 vaccines, solely for combination with MTX.14 17 However, in monotherapy, TNFi did not have deleterious effects on vaccination response, in accordance with previous findings.13 15 17 21 22 In contrast, the negative impact of tocilizumab, both in combination and in monotherapy, was not previously reported. This finding may be related to the weaker immunogenicity of the inactivated vaccine in comparison with mRNA or virus vector vaccines.33 Alternatively, patients evaluated herein were all seronegative at baseline, while other studies did not exclude pre-exposed patients,14–16 who are known to have a greater immune response magnitude.17 42
Of note, more than half of our RA population was using prednisone. In this regard, some trials11 14 21 22 evidenced a negative effect of steroids on immunogenicity of different SARS-CoV-2 vaccines but without a clear minimum daily dose threshold. Recently, doses greater than 10 mg/day were pointed as a possible cut-off in patients with lupus.43 Herein, we found that lower doses of 7.5 mg/day of prednisone are a major factor associated with impairment of NAb response.
Safety was demonstrated, with only mild AE reported. However, higher frequencies of AE occurred in patients with RA, as previously described for other COVID-19,44 influenza30 45–47 and yellow fever48 vaccines. This is possibly due to a greater awareness of symptoms among patients, and probably not related to recall or reporting bias, since diaries were given after each vaccine dose and collected in the next visit, and not at the end of the study.
Disease activity status did not interfere with the immune response as observed by different composite activity indexes, in accordance with previous findings on influenza A/H1N1 vaccine.30 However, data were obtained from up to 3 months before vaccination, precluding a definitive conclusion. Of note, most patients were on low activity status at the first vaccine dose. Therefore, the results may not be generalised for those with high disease activity.
The present study has some limitations. Disease Activity Scores with 28 joints (DAS28) were not systematically assessed after immunisation, although less than 6% of patients reported the perception of disease worsening. Similarly, no flare-up assessed by DAS28 was observed in two prior cohorts of patients with ARD who received mRNA vaccines.12 15 In contrast, Furer et al demonstrated worsening in Simplified Disease Activity Index score in 20% of patients with RA after complete vaccination with the BNT162b2 mRNA in a short period of follow-up,14 while 20% got better and 60% remained unchanged. It is not clear if the effect was due to vaccination itself, and further studies are necessary to clarify this point. Another limitation was the absence of T cell response evaluation. In addition, the comparison of small sample size subgroups with controls may be underpowered to draw definite conclusions.
In summary, we provided novel evidence that the RA moderate response to Sinovac-CoronaVac vaccine is associated with a distinct impact of drugs, with nearly all DMARD combinations presenting a deleterious effect in immunogenicity. A more restricted number of drugs (abatacept, MTX, tocilizumab and tofacitinib) also hampered this response even as monotherapy, while TNFi and non-MTX csDMARD did not. In addition, we identified that prednisone at a dosage of ≥7.5 mg/day decreased NAb response to vaccine. Altogether, these findings reinforce the need of a broader approach, not limited to a specific drug temporary suspension, to improve vaccine response for this population.
Data availability statement
All data relevant to the study are included in the article. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The protocol was approved by the National (Comissão Nacional de Ética em Pesquisa) and Institutional Ethical Committee (Comissão de Ética para Análise de Projetos de Pesquisa) of Hospital das Clinicas HCFMUSP, Faculdade de Medicina, Universidade de Sao Paulo, Brazil (ID CAAE: 42566621.0.0000.0068). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank the contribution of the Central Laboratory Division, Registry Division, Security Division, IT Division, Superintendence, Pharmacy Division and Vaccination Centre for their technical support. We also thank the volunteers for participating in the three in-person visits of the protocol and for handling the biological material, and those responsible for the follow-up of all participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Contributors ACM-R, CGSS, EFNY, SGP, EGK, NEA and EB conceived and designed the study. EB is responsible for the overall content as the guarantor. ACM-R, CGSS, EFNY, SGP, CAS, TP, LdVKK, NEA and EB participated in data collection and analysis and supervised clinical data management, writing of the manuscript and revision of the manuscript. LdVKK, TP and EB organised and supervised blood collection and vaccination protocol. Pasoto supervised serum processing, SARS-CoV-2-specific antibody ELISA/neutralisation assays and SARS-CoV-2 RT-PCR. ACM-R, KRB, DSD, AYS, HCdS, CGSS, EFNY, SGP, CAS, TP, LdVKK, CSRA, MSRS, TLN, GGMB, EGK, NEA and EB collected epidemiological and clinical data and assisted with the identification of SARS-CoV-2 infection and follow-up of patients. All authors helped to edit the manuscript.
Funding This study was sponsored by grants from Fundação de Amparo à Pesquisa do Estado de São Paulo (number: 2015/03756–4 to NEA, SGP, CAS and EB; number: 2017/14352–7 to TP; number: 2019/17272–0 to LdVKK; and number: 2021/06613–0 to TLN); Conselho Nacional de Desenvolvimento Científico e Tecnológico (number: 305242/2019–9 to EB and number: 304984/2020–5 to CAS) and B3, Bolsa de Valores do Brasil. Instituto Butantan supplied the study product and had no other role in the trial.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.