Article Text

Abstract
Objectives To compare the 1-year, 2-year and 5-year incidences of acute coronary syndrome (ACS) in patients with rheumatoid arthritis (RA) starting any of the biologic disease-modifying antirheumatic drugs (bDMARDs) currently available in clinical practice and to anchor these results with a general population comparator.
Methods Observational cohort study, with patients from Denmark, Finland, Norway and Sweden starting a bDMARD during 2008–2017. Time to first ACS was identified through register linkages. We calculated the 1-year, 2-year and 5-year incidence rates (IR) (on drug and ever since treatment start) and used Cox regression (HRs) to compare ACS incidences across treatments taking ACS risk factors into account. Analyses were further performed separately in subgroups defined by age, number of previous bDMARDs and history of cardiovascular disease. We also compared ACS incidences to an individually matched general population cohort.
Results 24 083 patients (75% women, mean age 56 years) contributing 40 850 treatment courses were included. During the maximum (5 years) follow-up (141 257 person-years (pyrs)), 780 ACS events occurred (crude IR 5.5 per 1000 pyrs). Overall, the incidence of ACS in RA was 80% higher than that in the general population. For all bDMARDs and follow-up definitions, HRs were close to 1 (etanercept as reference) with the exception of the 5-year risk window, where signals for abatacept, infliximab and rituximab were noted.
Conclusion The rate of ACS among patients with RA initiating bDMARDs remains elevated compared with the general population. As used in routine care, the short-term, intermediate-term and longer-term risks of ACS vary little across individual bDMARDs.
- rheumatoid arthritis
- tumor necrosis factor inhibitors
- cardiovascular diseases
- biological therapy
Data availability statement
Data are available upon reasonable request addressed to JA, johan.askling@ki.se.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Patients with rheumatoid arthritis (RA) are at increased risk of acute coronary syndrome (ACS) and other cardiovascular diseases, but how different biologic/targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) compare to each other with regard to these risks remains unclear, and most studies have compared risks with one b/tsDMARD to another rather than all available b/tsDMARDs to each other.
What does this study add?
In this Nordic collaborative study, we demonstrate that patients with RA initiating b/tsDMARDs in routine care are at an 80% more elevated risk of ACS than the general population, but as used in routine care, the short-term, intermediate-term and longer-term risks of ACS vary little across individual bDMARDs.
How might this impact on clinical practice or future developments?
As used in routine clinical practice, the short-term, intermediate-term and longer-term incidences of ACS vary little across individual bDMARDs.
Introduction
Patients with rheumatoid arthritis (RA) are at increased risk of cardiovascular (CV) diseases (CVDs), presumably due to a higher prevalence of traditional CV risk factors, effects of the inflammatory disease and, potentially also, direct or indirect effects of its treatment.1–9 Efficacious treatment of RA inflammation should reduce CV disease burden in RA,10–13 but while the absolute risks of CV events in the general population and in cohorts of patients with RA have declined substantially during the past decades, studies from recent years suggest that a gap in CV risk remains between these two populations.5 14–18
Antirheumatic therapies (here: biologic (b)/targeted synthetic (ts) disease-modifying antirheumatic drugs (DMARDs)) potentially play a role for (closing of) the gap.6 Besides suppressing RA-related inflammation, different b/tsDMARDs (as well as conventional synthetic DMARDs, oral corticosteroids or non-steroidal anti-inflammatory drugs (NSAIDs)) have by themselves been linked to detrimental as well as beneficial effects on CV disease risks.10 12 13 19–22 For instance, tumour necrosis factors inhibitors (TNFis) may aggravate heart failure, tocilizumab and rituximab may alter lipid levels and Janus kinase inhibitors may also induce lipid alterations.10 23–25 In the relative absence of head-to-head CV prevention trials of all DMARDs against each other in RA, observational studies have assessed various aspects of CV risks related to biologic DMARDs (bDMARDs), with somewhat varying results.10 11 However, most of the studies on this topic have compared one drug or one class of drugs (eg, TNFi to csDMARDs) to another, rather than comparing all individual drugs,6 20 26 while from a clinical decision-making point of view, results on individual drugs could also be of interest. Further, long-term studies on CV risks with b/tsDMARDs are sparse.12 13
For these reasons, we aimed to study the short-term (1 year), intermediate-term (2 years) and longer-term (5 years) incidences of acute coronary syndrome (ACS) in patients initiating b/tsDMARDs, taking relevant other factors into account. We further compared the ACS incidences in this RA population to the general population.
Subjects and methods
Design and setting
We performed an observational cohort study using prospectively collected individual-level data from the clinical rheumatology registers in Denmark (DANBIO), Finland (ROB-FIN), Norway (NOR-DMARD) and Sweden (SRQ-ARTIS).27–31 In each country, linkages of the clinical data to other national registers were performed in order to identify data on past and incident ACS events, covariates (see definitions below), emigration and vital status throughout the study period from 1 January 2008 (1 January 2009 for Norway) to 31 December 2017.30
Study population and exposure
We defined ten drug-specific treatment cohorts as all initiators of: adalimumab, certolizumab pegol, etanercept, golimumab, infliximab, abatacept, rituximab, tocilizumab, baricitinib and tofacitinib (the low number of patients and the short follow-up precluded meaningful analyses of the latter two drugs). One patient could contribute to several treatment cohorts (eg, a patient starting etanercept, later switching to tocilizumab, contributed to both cohorts). For all treatments, the number of previous b/tsDMARDs the patient had been exposed to was retrieved. Patients were included irrespective of history of ischaemic heart disease, including ACS.
Outcome
In each cohort, ACS during follow-up was defined as the first registered event of hospitalisation due to either unstable angina (International Classification of Diseases 10th Revision (ICD-10) I20.0) or acute myocardial infarction (MI) (transmural MI ICD-10 I21.0, I21.1, I21.2, I21.3; subendocardial MI ICD-10 I21.4; unspecific MI I21.9), as identified via linkage to the national patient registers.30 In Sweden, the definition also included deaths stating ICD-10 I21 or I20.0 as main cause.
Covariates
Using the registers’ linkage,30 we identified baseline (ie, at treatment start) covariates for each treatment cohort: demographics (eg, sex), clinical (eg, C reactive protein (CRP)), comedication (eg, methotrexate), comorbidities (eg, history of a thromboembolic event) and related medications (eg, use of anticoagulants) and other information (eg, number of previous hospitalisations), see online supplemental table 1.
Supplemental material
Follow-up and risk windows
For each treatment cohort, follow-up began at the start of the b/tsDMARD in question. Any treatment interruption (of the same drug) shorter than 3 months was disregarded. Since patients are recorded as being on a specific treatment rather than with, for example, their dates of dispensation, the treatment interruptions’ rule did not affect the handling of rituximab data. We made no distinction between originator products and their biosimilars.
We applied five different definitions of the follow-up. First, (1) we used an ‘on-drug’ approach with follow-up stop being defined as the first of: first registered ACS, emigration, death, 90 days after any discontinuation of the treatment under study, 2 years after treatment start and end of the study period and (2) same as (1) but 5 years (instead of 2 years) after treatment start. Then, an ‘ever since treatment start’ approach was used in which any drug discontinuation disregarded was also used with a maximum of (3) 1-year, (4) 2-year and (5) 5-year follow-up (online supplemental figure 1). The ‘on-drug’ approach is conceptually similar to an ‘as-treated’ approach used in randomised controlled trials (RCT), while the ‘ever since treatment start’ is similar to an intention-to-treat approach.32 This latter approach could result in one event being attributed to more than one medication.
General population comparator
We identified general population cohorts (available in Denmark and Sweden only) and (through the same type of register linkages) ACS events within these cohorts. We selected each RA patient’s first b/tsDMARD-treatment record to define a cohort of unique RA patients. The general population comparator cohort was individually matched (1:10 in Denmark and 1:5 in Sweden) to these, on sex, age and area of residence. As for the patients with RA, general population controls were included irrespective of history of ischaemic heart disease, including ACS.
Statistical analyses
Online supplemental table 2 contains an overview of the analyses performed according to pooling of data across countries and follow-up definitions. We assessed descriptive statistics at baseline for each treatment cohort and in each country, in each country (pooling treatments) or for each treatment (pooling countries). Because of the low number of patients and follow-up, the baricitinib and tofacitinib cohorts were only included in this descriptive part. For the bDMARD cohorts, we computed the number of ACS events, follow-up-times at risk and crude incidence rates (IRs) of ACS in each treatment cohort, for the five follow-up definitions and per country and treatment. We compared the association between individual bDMARDs and incident ACS using Cox regression, with etanercept as reference, time since treatment start as time scale and a robust sandwich estimator to account for the correlated data structure. Further, as statistical heterogeneity among countries for each treatment was low (I2 statistic<25%), analyses were performed on pooled data and stratified by country (ie, stratified Cox). We used four successively adjusted analyses models: model 1 provided crude HRs (ie, the relative rates as observed in the clinic); model 2 adjusted for age, sex and calendar period of bDMARD start (2008–2013 vs 2014–2017); model 3 additionally included the number of previous b/tsDMARDs, history of ACS, RA seropositivity and CRP level and model 4 additionally adjusted for smoking, number of hospitalisations, accumulated dose of prednisolone, concomitant use of methotrexate, history of hypertensive or cardiac disease (other than ACS), thromboembolic or cerebrovascular events, presence of diabetes, presence of at least one among the five following diseases/comorbidities: kidney disease, affective disorder, chronic obstructive pulmonary disease (COPD), hospitalised infection and cancer and prescription of at least one of the five following drugs: anticoagulants, aspirin, ACE, beta-calcium and lipid-lowering drug. Norwegian data were missing information on several of these variables and were not included in model 4. Variables included for adjustment were measured at baseline and predetermined. Smoking and RA seropositivity included a ‘missing’ category. CRP was categorised in quartiles and a ‘missing’ category was added to these. Otherwise, no imputation was performed for other variables. In all tabulations, cells with less than five ACS events are displayed as ‘N/A’ and no HRs were assessed. Data analyses were performed in SAS, V.9.4.
Separate analyses in subgroups of patients
We performed the same Cox analyses separately by age (18–64 vs 65 years or older), number of previous b/tsDMARDs (none, one, two or more) and presence (yes vs no) of history of any CVD. For this latter analysis, a more extensive definition was applied to rule out previous CV risk and included history of hypertensive or cardiac disease (ACS and other), thromboembolic or cerebral event or prescription of anticoagulants, aspirin, ACE, beta-calcium or lipid-lowering drug. Additionally, the 5-year ‘on-drug’ analyses by treatment cohort were performed restricted to patients starting their first ever bDMARD.
Comparison with the general population
In the Cox analyses, the general population individuals and their index RA patients were followed up from treatment start of the index RA patient (irrespective of which b/tsDMARD was started) and onwards using an ever since treatment start approach with no imposed limit (other than the study period) in the follow-up duration. The Cox regression was run separately for the two countries with attained age as time scale, stratified on the matching variables and adjusted for history of previous ACS. In addition, the same analysis was performed for each bDMARD treatment cohort separately.
Patients’ involvement
This study was performed within the context of a Nordic rheumatology registers collaboration, which employed a patient representatives panel.
Results
Baseline characteristics
Overall, 24 083 patients were included (75% women, mean age 56 years) initiating 40 850 treatment courses. Of these, etanercept was the most common (10 866, 27% of all treatments courses), followed by adalimumab (14%), infliximab (13%), rituximab (12%), tocilizumab (10%), certolizumab pegol (9%), abatacept (9%), golimumab (6%) and baricitinib and tofacitinib (<1%). Overall, 47% of all treatment episodes were from Sweden (19 090 treatment episodes), 34% from Denmark and Finland and Norway contributed 14% and 6%, respectively. Overall, 60% of the treatment starts represented a first ever b/tsDMARD start and 20% a second.
Descriptive statistics for individual b/tsDMARD treatments (all countries pooled) are displayed in table 1. Patients starting rituximab tended to be older (median 62 years) than patients receiving other b/tsDMARDs (median ranging from 55 to 59 years). Compared with patients starting a TNFi, patients starting a non-TNFi bDMARD generally presented somewhat higher values for clinical variables (CRP, erythrocyte sedimentation rate, patient’s global health assessment, pain, health assessment questionnaire and disease activity score with CRP (DAS28CRP)), had been exposed to more previous b/tsDMARDs and more often had comorbidities (COPD, diabetes, history of CV event, history of kidney disease and history of infection). Overall, 30% of the patients on rituximab had a history of hypertensive or cardiac disease, while this proportion was less than 20% for patients on TNFi and between 20% and 25% for the other non-TNFi bDMARDs and tsDMARDs. Patients starting a tsDMARD or non-TNFi bDMARD had a larger accumulated dose of prednisolone than patients starting a TNFi. Intercountry differences were small, overall and by treatment (online supplemental tables 3 and 4).
Baseline characteristics for each treatment cohort (all countries pooled together)
Occurrence of ACS
During the maximum follow-up (5 years, ever since treatment start) amounting to 141 257 person-years (pyrs), we observed a total of 780 incident ACS events, corresponding to a crude IR of 5.5 per 1000 pyrs. The 5-year ‘on-drug’ crude IR was similar. The corresponding numbers for the shortest follow-up definition (1 year, ever since treatment start) were 215 incident ACS during 38 102 pyrs and a crude IR of 5.6 per 1000 pyrs (table 2). For almost all follow-up definitions, rituximab was associated with the highest crude ACS incidences, table 2 and online supplemental table 5.
Number of events per person-years (pyrs), crude incidence rates (IRs) (95% CIs) per 1000 pyrs in each treatment cohort, for 1-year, 2-year and 5-year follow-up lengths, ‘on-drug’ and ‘ever since treatment start’ follow-up definitions
Comparison of risks (HR) in individual bDMARDs
Online supplemental table 6 displays crude and successively adjusted HRs, by treatment and by follow-up definition. Across all comparisons (ie, all follow-up definitions), there was a consistent pattern of statistically significantly elevated HRs for abatacept and rituximab in crude models (HRs ranging from 1.6 to 2.3) the magnitude of which decreased and lost its statistical significance with successive adjustments, so that in the fully adjusted model, HRs for abatacept and rituximab ranged between 1.1 and 1.3. The HRs for infliximab increased slightly with increasing length of follow-up, reaching 1.49 (1.08–2.05) for the 5-year follow-up ‘on drug’. For the other bDMARDs, HRs were close to 1 (online supplemental table 6 and figure 1).
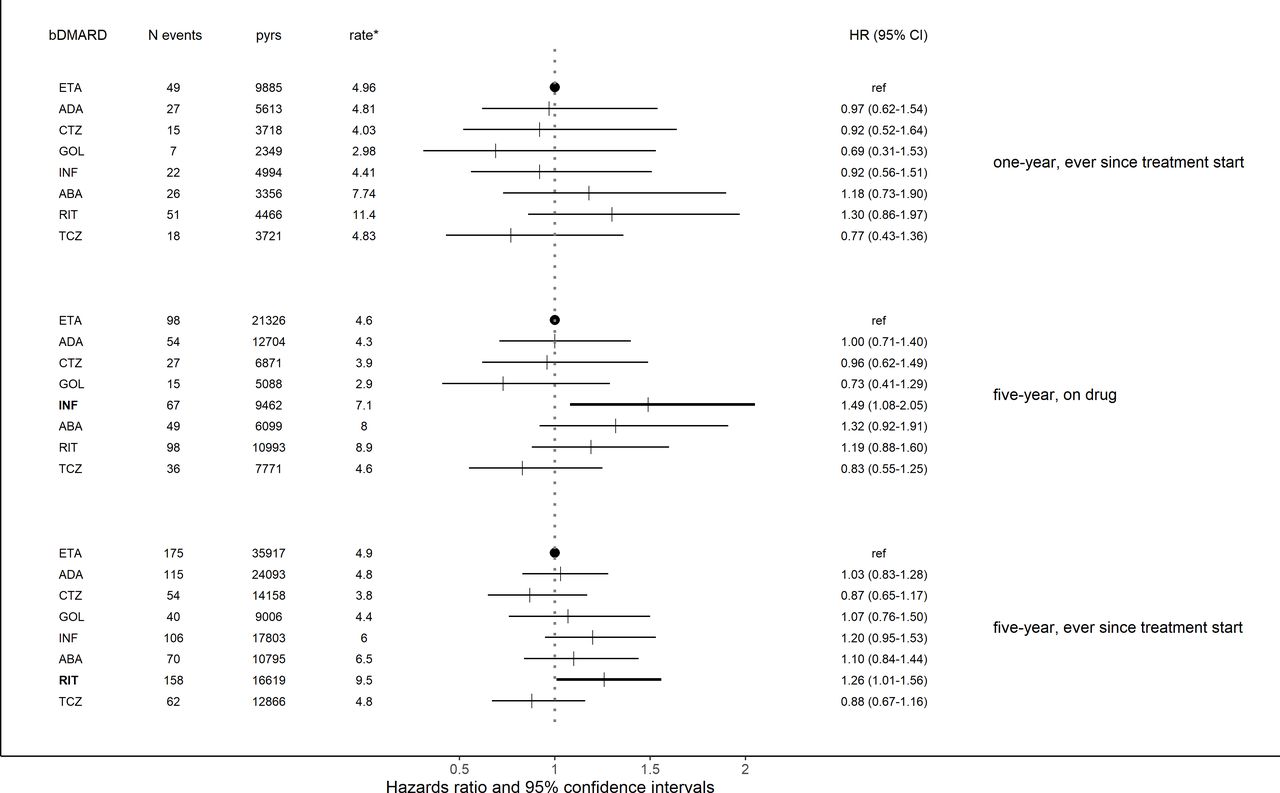
Number of events, person-years (pyrs), crude incidence rates per 1000 pyrs for each bDMARD treatment cohort, HRs obtained from Cox analyses (95% CIs), using etanercept as reference, for the shortest (, ever since treatment start, 1-year) and the longest (ever since treatment start, 5 years) risk windows. *Rate: rate per 1000 pyrs. ABA, abatacept; ADA, adalimumab; bDMARD, biologic disease-modifying antirheumatic drug; CTZ, certolizumab pegol; ETA, etanercept; GOL, golimumab; INF, infliximab; RIT, rituximab; TCZ, tocilizumab.
Separate analyses in subgroups of patients defined by the number of previous b/tsDMARds showed that, among patients starting their first or second bDMARD, none of the drugs were more (nor less) associated with ACS, with the exception of abatacept (‘on-drug’ analysis only) (online supplemental table 7, upper panel and figure 2). By contrast, among patients starting their third or more bDMARD and followed up for 5 years, all HRs were higher with the HRs for abatacept, infliximab and rituximab borderline or statistically significantly increased (figure 2). The analyses performed by age group (18–64 and 65+ years) provided results similar to the main analysis (online supplemental table 7, median panel and figure 2). Excluding all patients with a history of any CVD resulted in a pattern of HRs largely similar to those of the main analysis (online supplemental table 7, lower panel and figure 2). Finally, in patients with a history of any CVD, all HRs were close to one with the exception of infliximab for which the HR was 1.49 (1.02–2.18) for the 5-year follow-up, ‘on-drug’ approach (online supplemental table 7, lower panel and figure 2).

{kind=link}
{kind=link}
HRs obtained from Cox analyses (95% CIs), comparing the rates for each bDMARD to that for etanercept, for a 5-year follow-up length, and fully adjusted model (model 4). Analyses were performed separately on subgroups defined by (A) number of previous b/tsDMARDs (no vs one vs two or more), ‘on-drug’ and ‘ever since treatment start’ approaches, (B) age (18–64 vs 65+ years), ‘on drug’ and (C) history of cardiovascular disease (CVD) (without vs with), ‘on drug’.ABA, abatacept; ADA, adalimumab; b/tsDMARDs, biologic/targeted synthetic disease-modifying antirheumatic drugs; CTZ, certolizumab pegol; ETA, etanercept; GOL, golimumab; INF, infliximab; RIT, rituximab; TCZ, tocilizumab.
Comparison with the general population
Pyrs, mean follow-up times and crude incidences of ACS for the general population comparator cohorts were 304 612 pyrs, 4.8 years and 2.4/1000 pyrs for Denmark and 239 873 pyrs, 4.5 years and 3.6/1000 pyrs for Sweden, which, compared with the RA populations (37 175 pyrs, 5.1 years and 4.5/1000 pyrs in Denmark and 51 193 pyrs, 4.4 years and 6.6/1000 pyrs in Sweden) resulted in HRs (95% CI) of 1.8 (1.5–2.1) for Denmark and 1.8 (1.6–2.0) for Sweden, taking the matching factors (age, sex and calendar time) and history of ACS into account. Treatment-specific analyses showed that every bDMARDs were associated with a higher IR of ACS compared with the general population (online supplemental table 8). The HR (95% CI) for etanercept was around 1.5 in both countries.
Discussion
In this study of almost 41 000 treatment episodes of bDMARDs and covering population-based data from four Nordic countries, we observed that the IR of ACS in patients with RA initiating treatment with a bDMARD was around 80% higher than in the general population. Comparing the bDMARDs to each other, we noted little differences in ACS rates in the short and intermediate terms. In the longer term, initiation of abatacept, infliximab and rituximab was associated with a moderately increased rate of ACS, a finding which remained when patients with previous CVD were excluded, but was largely confined to patients starting their third or later b/tsDMARD.
Numerous studies have addressed aspects of CVD in patients with RA in relation to treatment, many of them reporting on beneficial effects of DMARDs (including methotrexate, TNFis and other bDMARDs) on CV risk factors such as glucose, cholesterol or lipid metabolism, blood pressure, endothelial function and arterial stiffness.12 13 21 22 33–36 Most studies focusing on the association between treatment and CV risk have compared groups of drugs rather than individual ones, at least with regard to TNFis. Compared with non-bDMARDs, TNFis have a positive effect on the risk of CV events,10 11 20 37–39 in particular among responders;39–41 tocilizumab has been reported to exert marginally superior effects on CV outcomes compared with TNFis,10 12 13 but results are conflicting.25 42–44 No detrimental effect on CV outcomes of abatacept or rituximab have been reported.12 13 42 One study reported greater benefit for TNFi non-responders who, as next bDMARD, received tocilizumab or abatacept instead of rituximab.45
The observed increased risk for abatacept, infliximab and rituximab in our study might be explained by residual confounding or confounding by indication. Patients on abatacept and rituximab had more comorbidities and longer disease duration with potentially longer exposure to inflammation, which is associated with CV risk.46 As expected, adjusting for relevant factors generally led to a considerable attenuation of the strength of the association, but we cannot formally disentangle whether our results indicate an interaction (ie, that the ‘true’ risk of certain bDMARDs varies across subsets of patients with RA as defined by their treatment history) or reflect residual channelling bias. The potential protective effect of tocilizumab against ACS, as reported in Atzeni et al,13 was not clearly supported by our results and remains to be clarified. Lastly, compared with the study by Xie et al,42 which also compared individual bDMARDs (although with some differences in the source populations), the HRs in our study were generally closer to 1 and with narrower 95% CI.
Our study has limitations. Although we had access to ample data on comorbid conditions, demographics and clinical characteristics, we lacked information on socioeconomic data such as education level, sick leave and disability pension. We did not have information on concomitant NSAIDs or Cyclooxygenase-2 (COX-2) inhibitors. We also had too little data to allow any meaningful comparison of ACS risk in patients treated with tsDMARDs, for which the CV safety profile is currently questioned.7 13 24 25 47 The comparison of patients with RA with the general population included patients with RA starting a b/tsDMARD treatment, hence representing the subset of the entire pool of RA ill enough to need a b/tsDMARD yet fit enough to be presumed to tolerate such treatment. The ACS definition also varied somewhat between countries which could impact the IRs but not the HRs as Cox analyses were stratified on the country variable. We also used ACS, which is a clinically well-defined entity, as outcome instead of the more heterogeneous composite 'major cardiovascular event' (MACE), in order to further reduce the potential for country-specific variations in the outcome construct, but limited the comparability of our results to, for example, trials using MACE as its single CV outcome.
Our study has several strengths, including its setting (the built-in possibility to compare and pool across five large RA source populations), its large number of subjects and events and the possibility to compare risks across different strata of patients and follow-up times. The use of register linkages and previously developed algorithms to define ACS and other variables ensured an independent (from exposure) assessment of ACS events, low risk of misclassification of exposure, outcomes and covariates and allowed adjustments for many potential confounders. Data on general population comparator subjects enabled contextualising of our findings. We employed multiple definitions of risk windows to enable assessment of both short-term, intermediate-term and longer-term risks. Finally, with the exception of tsDMARDs, our study allowed evaluation of risks by all clinically available bDMARD options rather than by one (drug or class) versus one other, the former being a reasonable point of departure from a clinical decision-making point of view.
To conclude, as used in routine care, the risks of ACS in patients with RA starting a bDMARD vary little across individual drugs for short and intermediate terms. This most likely also applies to the longer term despite signals of higher ACS incidence that are most probably linked to the treatment context including patient-related factors rather than to the drug per se. Thus, our results suggest that in RA treated with bDMARDs, the bDMARD used does not seem to matter for the risk of ACS.
Data availability statement
Data are available upon reasonable request addressed to JA, johan.askling@ki.se.
Ethics statements
Patient consent for publication
Ethics approval
Denmark: ethical approval not required for registry studies (komitelovens §14, stk. 2, www.nvk.dk), Capital region data-protection office RH-2015–209 and Isuite 04145; Finland: ethical approval—FI: 73/13/03/00/2014; Norwegian: Regional Committees for Medical and Health Research Ethics South East (Ref. 2019/329/REK sør-øst) and Sweden: the Swedish Ethical Review Authority, 2015/1844-31/2.
Acknowledgments
The authors would like to thank Frank Mehnert, Nina Trocovic and Jonas Söderling who assembled the data, respectively, for Denmark, Finland, Norway and Sweden and patients and clinical departments contributing to DANBIO, ROB-FIN, NOR-DMARD and SRQ-ARTIS.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Lay summary
Disclaimer : This is a summary of a scientific article written by a medical professional (“the Original Article”). The Summary is written to assist non medically trained readers to understand general points of the Original Article. It is supplied “as is” without any warranty. You should note that the Original Article (and Summary) may not be fully relevant nor accurate as medical science is constantly changing and errors can occur. It is therefore very important that readers not rely on the content in the Summary and consult their medical professionals for all aspects of their health care and only rely on the Summary if directed to do so by their medical professional. Please view our full Website Terms and Conditions.
Copyright © 2022 BMJ Publishing Group Ltd & European League Against Rheumatism. Medical professionals may print copies for their and their patients and students non commercial use. Other individuals may print a single copy for their personal, non commercial use. For other uses please contact our Rights and Licensing Team.
Footnotes
Handling editor Josef S Smolen
Presented at The study was presented as an oral presentation at the European Alliance of Associations for Rheumatology (EULAR) annual conference in June 2021 (OP0114).
Contributors Substantial contribution to conception and design, reading and approval of the final version and revising the draft critically:BD, LL, SAP, BG, MLH, KLG, RP, HR, CT, BG, BM and JA . Analysis: BD. Interpretation of data: BD, LL, SAP, BG, MLH, KLG, HR, CT, BG, BM and JA. Drafting the article: BD, JA, LL, SAP and BG. Guarantor: JA.
Funding This work was supported by NordForsk and the Foundation for Research in Rheumatology (Foreum), Vinnova. The research infrastructure was supported by funds from the Swedish Research Council, the Swedish Heart Lung Foundation, the Swedish Cancer Society and Region Stockholm–Karolinska Institutet (ALF).
Competing interests LL: chairs the steering committee of the Swedish Rheumatology Quality Register, SRQ. Karolinska University Hospital and its principal investigator SRQ has had agreements for register data analyses with AbbVie, Amgen, BMS, Eli Lilly, Galapagos, Janssen, Novartis, Pfizer, Sanofi, Sobi and UCB. BG: research grants: Pfizer, BMS, Sandoz and AbbVie. MLH: grants: AbbVie, Biogen, BMS, Celltrion, Eli Lilly Denmark A/S, Janssen Biologics B.V, Lundbeckfonden, MSD, Pfizer, Roche, Samsung Bioepis and Sandoz; chairs the steering committee of the Danish Rheumatology Quality Registry (DANBIO), which receives public funding from the hospital owners and funding from pharmaceutical companies, and cochairs Eurospa, which generates real-world evidence of treatment of psoriatic arthritis and axial spondyloarthritis based on secondary data and is partly funded by Novartis. KLG: grants: BMS. RP: lecturer: Actelion, Boehringer Ingelheim, Pfizer, Sanofi and Janssen; grants: Mylen and data safety monitoring: Boehringer Ingelheim, Lilly, Janssen and AbbVie. HR: Congress fees and speaker fees from AbbVie and consulting fees: Celgene and Pfizer. CT: speaker fees: AbbVie, Bristol-Myers Squibb, Nordic Drugs, Pfizer and Roche. BG: consultant and lecturer fees: Novartis. BM: research grant (paid to employer) and consultancy fees: Novartis. JA: grants: AbbVie, Astra-Zeneca, BMS, Eli Lilly, Galapagos, MSD, Pfizer, Roche, Samsung Bioepis, Sanofi and UCB. AbbVie, Astra-Zeneca, BMS, Eli Lilly, MSD, Pfizer, Roche, Samsung Bioepis, Sanofi, and UCB have entered into agreements with Karolinska Institutet with JA as principal investigator, mainly in the context of safety monitoring of biologics via the ARTIS national safety monitoring system.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.