Article Text

Abstract
Objectives: To study the presence of citrullinated proteins in inflammatory conditions and in clinically non-affected tissues of controls.
Methods: Synovial biopsy specimens from 19 patients with rheumatoid arthritis and 10 healthy controls were investigated by immunohistochemistry. Additionally, muscle tissue from 5 patients with polymyositis and from 7 healthy controls, intestinal tissue from macroscopically affected and non-affected areas from 10 patients with inflammatory bowel disease (IBD) and tonsil tissues from 4 chronically inflamed tonsils were studied.
Results: Citrullinated proteins were present in all synovial biopsy specimens from patients with rheumatoid arthritis, whereas only three of 10 healthy synovial biopsy specimens showed scarce amounts of citrullination. Citrullination was also present in all myositis-affected muscles, whereas it was absent in the muscle tissues of controls. All tonsil biopsy specimens studied were positive for citrulline. Even though more frequently detected in the macroscopically affected colonic areas, no marked difference was observed in the pattern or extent of citrullination between the macroscopically affected and non-affected intestinal IBD tissues.
Conclusion: Citrullination is present in a wide range of inflammatory tissues, suggesting that this process is inflammation dependent rather than disease dependent.
- IBD, inflammatory bowel disease
- PAD, peptidylarginine deiminase
- citrullination
- arthritis
- polymyositis
- inflammatory bowel disease
Statistics from Altmetric.com
Rheumatoid arthritis is an inflammatory disease that is characterised by the presence of antibodies against citrullinated peptides that may have an important role in the pathogenesis of rheumatoid arthritis.1 Citrullination represents the calcium-dependent conversion of peptidylarginine to peptidylcitrulline, which is catalysed by peptidylarginine deiminase (PAD) enzymes. This enzymatic conversion normally occurs in processes such as epidermal differentiation,2 formation of the hair follicle3 and differentiation of the myelin sheath during development of the central nervous system.4 The presence of citrullinated proteins was initially considered specific to the synovium in patients with rheumatoid arthritis.5 However, recent reports showed that citrullinated proteins are also present in non-rheumatoid arthritis inflammatory synovitis,6,7 suggesting that citrullination of specific antigenic targets rather than citrullination as such is a disease-specific process. Moreover, citrullination occurs in autoimmune neurodegenerative diseases such as multiple sclerosis4,8 and Alzheimer’s disease.9 In the light of these observations, we asked whether citrullination occurs in types of inflammation other than arthritis and to what extent citrullination is present in the normal joint. To investigate this, we evaluated the presence of citrullinated proteins in inflamed and non-inflamed tissues.
MATERIALS AND METHODS
Patients
In all, 19 patients meeting the American College of Rheumatology criteria for rheumatoid arthritis and 10 healthy controls without any history of joint complaints were recruited to this study. Synovial biopsy specimens were obtained from different clinically affected joints (10 knee, 4 metatarsophalangeal, 2 elbow, 2 hip and 1 shoulder biopsy specimens) of patients with rheumatoid arthritis, through either arthroscopy (4 biopsy specimens) or open surgery (15 biopsy specimens). Synovial knee biopsy specimens from healthy controls were obtained by arthroscopy.
Muscle biopsy specimens were obtained from five patients with polymyositis and seven healthy controls with normal muscle histopathology (three with chronic myalgia and one with increased creatinine kinase levels, all without any clinical or laboratory signs of any muscle disorders and three healthy controls without muscle complaints).
In all, 10 patients with inflammatory bowel disease (IBD), 3 with ulcerative colitis and 7 with Crohn’s disease, were subjected to colonoscopy. Two biopsy specimens, one from macroscopically affected areas and the other from macroscopically non-affected areas, were obtained for each patient.
We also included in the study tonsil tissues from four patients subjected to tonsillectomy owing to chronic tonsil inflammation.
Normal skin sections from two participants, in whom citrullination was known to be present at the corneum stratum,2 were used as a control staining.
All tissues were snap frozen in dry ice-cooled isopentane; serial cryostat sections (7 μm) were fixed for 20 min with 2% (v/v) formaldehyde and stored at −70°C.
All procedures were approved by the Northern Stockholm Ethical Review Board and informed consent was obtained from all the participants in the study.
Histological analysis and immunohistochemistry
Histological analysis was carried out to characterise the inflammation grade in synovial and colonic biopsy specimens. For synovial biopsy specimens, a four-point scale was used for synovial lining thickness, vascularity and inflammatory cell infiltrate. Colonic biopsy specimens were investigated with regard to cell infiltrate and integrity of the lamina propria and the Lieberkuhn’s crypts.
The presence of citrullinated proteins was detected using a rabbit polyclonal antibody against modified citrulline residues (Anti-Citrulline Modified Detection Kit, Upstate, Lake Placid, New York, USA) at a concentration of 0.2 μg/ml, as previously described.6 The detection system consisted of a biotinylated goat anti-rabbit antibody (Vector Laboratories, Burlingame, California, USA), followed by development with an avidin–biotin-based method (ABC Kit, Vector Laboratories, Burlingame, California, USA). Isotype controls with rabbit immunoglobulins (Dako, Glostrup, Denmark) were also included. The presence of citrullinated proteins was assessed semiquantitatively by two independent observers, who were unaware of the sample’s identity, on a four-point scale as follows: 0, no positive signal; 1, minimal presence; 2, moderate amounts; and 3, high degree of citrullination.
We also investigated the PAD-2 expression in two synovial biopsy specimens from patients with rheumatoid arthritis, three intestinal biopsy specimens and two tonsils by using a rabbit polyclonal antibody (Abcam, Cambridge, Massachussetts, USA).
Statistical analysis
Differences between histological scores were analysed by Mann–Whitney test and differences between proportions by Fisher’s exact test. Value of p<0.05 was considered to be significant.
RESULTS
Table 1 summarises the results of the immunohistochemical analysis.
Immunohistochemical analysis of the study participants
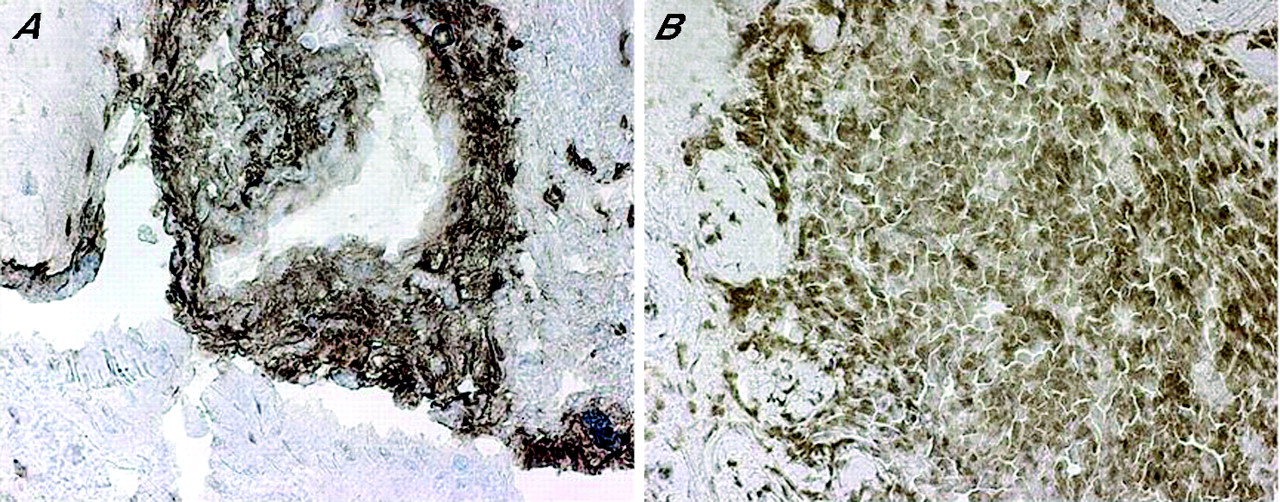
All synovial biopsy specimens from patients with rheumatoid arthritis showed signs of inflammation, with a median histological score of 2 for synovial lining thickness (range 1–4, 4 missing data due to absence of the lining layer in the biopsy specimen), 2 for vascularity (range 1–4) and 2.5 for inflammatory cell infiltrate (range 1–4). Citrullinated proteins were present in all investigated synovial biopsy specimens (100%) from patients with rheumatoid arthritis (fig 1A), with large variations between different patients resulting in a median value of 1 (range 0.5–3). Citrullination was present both in the lining and in the sublining layer, intracellularly as well as extracellularly (fig 2). Endothelial cells, fibroblasts and mononuclear cells were positive for citrullinated proteins, whereas extracellular citrullination was mainly located in the amorphous fibrin areas. 3 of 10 (30%) healthy synovia contained low amounts of citrullinated proteins (fig 1B), resulting in a median value of 0, with a range of 0–1 (p<0.05 compared with specimens from patients with rheumatoid arthritis). Citrullinated proteins were present in isolated mononuclear cells in the lining and sublining, few endothelial cells and sublining fibroblasts.

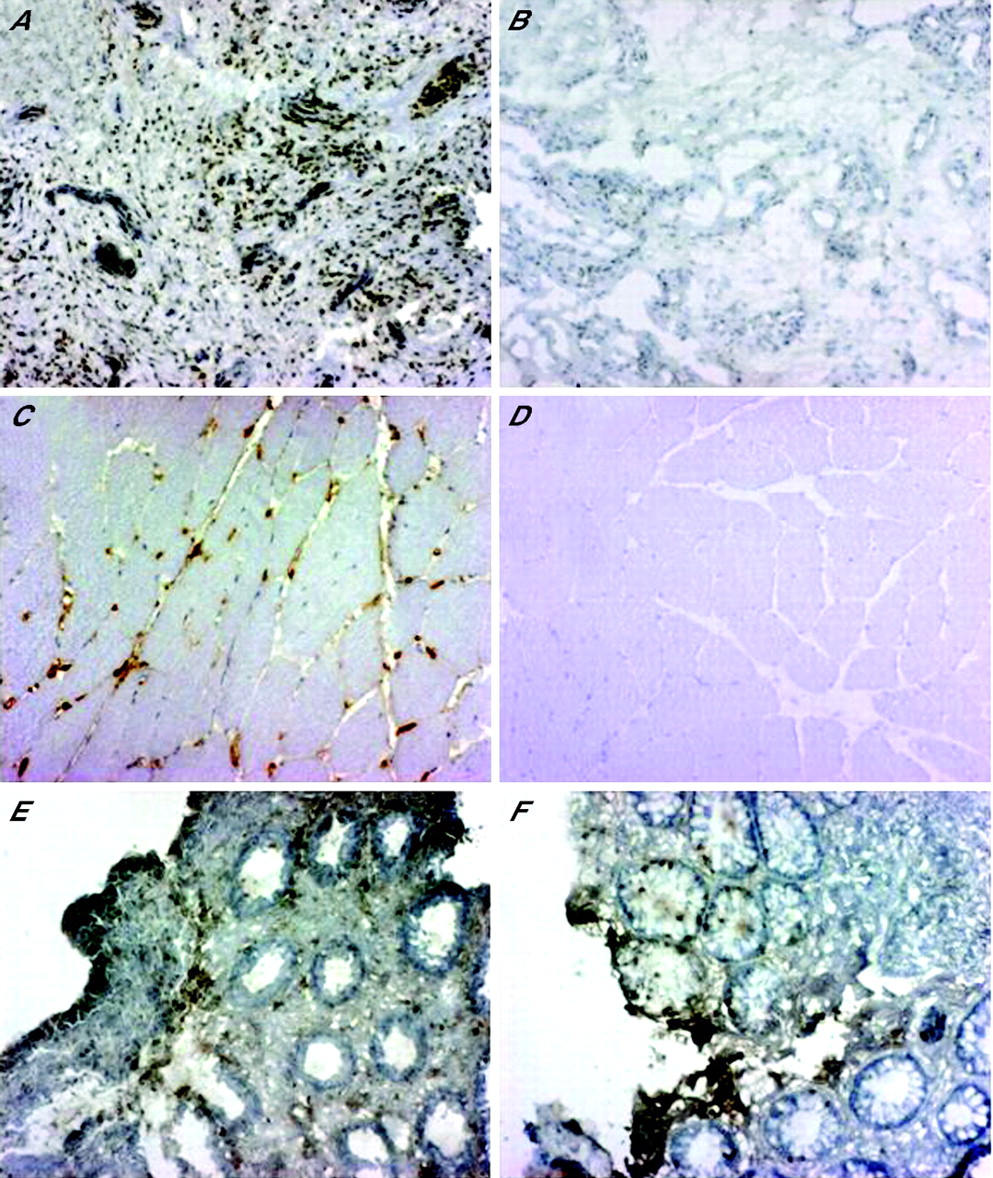
Citrullinated proteins are preferentially expressed in inflammatory tissues. Images represent immunohistochemistry pictures of citrulline proteins in (A) rheumatoid arthritis synovium, (B) healthy synovium, (C) polymyositis, (D) normal muscle, (E) inflammatory bowel disease (IBD) macroscopically affected colon biopsy and (F) IBD macroscopically non-affected colon biopsy.
{kind=link}
{kind=link}
Citrullinated proteins are detected both extracellularly and intracellularly in the lining (A) and in the sublining (B) layers in rheumatoid arthritis synovium.
All samples from patients with polymyositis (100%) were positive (fig 1C), with citrullinated proteins present both in endothelial and inflammatory cells, whereas muscle fibres were negative. By contrast, muscle biopsy specimens from healthy controls (fig 1D) were completely negative (p<0.05 compared with samples from patients with polymyositis).
Colonic biopsy specimens from patients with IBD showed various amounts of citrullinated proteins with no significant differences between macroscopically affected (fig 1E) and non-affected (fig 1F) areas when assessed semiquantitatively. However, in patients with IBD, 70% of the macroscopically affected samples showed the presence of citrullinated proteins compared with only 40% of the macroscopically non-affected samples (p>0.05). Citrullination was present mainly in the lamina propria cells and also in some epithelial cells and infiltrating mononuclear cells of the Lieberkuhn’s crypts, with the same pattern distribution as PAD-2 (data not shown). In agreement with these data, histological examination showed that all macroscopically non-affected biopsy specimens showed minimal to moderate signs of inflammation. Even though less inflammation was seen in the macroscopically non-affected biopsy specimens, no major differences were observed between the two groups.
All four chronically inflamed tonsil samples were positive (data not shown), with citrullinated proteins and PAD-2 expression in macrophage-like cells, both in the T cell and B cell areas.
DISCUSSION
Citrullinated proteins were previously identified in different types of inflammatory arthritis,6,7 suggesting that citrullination is an inflammation-related event. Our study confirms this hypothesis by demonstrating the presence of citrullination in several inflammatory tissues, with little to no expression in control non-inflammatory tissues.
We used a commercially available kit to detect the presence of citrulline-containing proteins independent of neighbouring amino acids to ensure universal detection of citrullinated proteins. In this method, the citrulline side chains are chemically modified, resulting in a bulky complex structure that makes the amino acid sequences flanking the modified citrulline negligible. Moreover, as previously shown by Senshu et al,10 the antibodies have a high sensitivity, reacting only with modified citrulline but not with the unmodified form or free L-citrulline. Other antibodies currently available for immunohistochemical detection of citrulline are dependent on the backbone protein and are therefore less likely to recognise all types of citrullinated proteins.6,11
The specificity of synovial citrullination represents a debated research issue. Previous studies that used a similar detection method identified citrullinated proteins in synovial biopsy specimens of different types of inflammatory arthritis and non-inflammatory joint diseases.6 We further identified scarce amounts of citrullination in synovial biopsy specimens of healthy controls without complaints in the joints. This is not surprising because citrullination seems to be related to the degree of synovial inflammation and because minor injury or physical exercise may initiate a subclinical synovial inflammation in bearing joints even in non-diseased people. However, we observed a considerably higher degree and prevalence of citrullination in the synovia from patients with rheumatoid arthritis compared with the normal controls, suggesting a correlation between inflammation and citrullination. In this study, we dealt with the process of citrullination as such, but further studies to investigate the presence of specific target antigens in different tissues are needed for a better understanding of the relevance of these processes in rheumatoid arthritis.
To confirm this hypothesis, we further investigated other inflammatory conditions: polymyositis, IBD and chronic tonsillitis. All these conditions were associated with various degrees of citrullination, although lower levels and frequency were seen in control tissues. Interestingly, none of the normal muscle biopsy specimens was positive for citrullination. This could be due to the lack of inflammatory cells or to low levels of citrullination that were below detection limits with the method used. Macroscopically unaffected colonic biopsy specimens showed comparable amounts of citrullinated proteins as in macroscopically affected biopsy specimens, although less often (not significant). This finding may be due to the potential disagreement previously shown between macroscopic and histological evaluation in colonic biopsy specimens from patients with IBD.12 This hypothesis is supported by the histological evaluation showing minimal to moderate amounts of inflammation in the macroscopically non-affected colonic biopsy specimens. Moreover, intestinal tissue represents a natural barrier of the human body, and in this context a constant inflammatory process may be present even subclinically.
Our findings show that increased citrullination is not a disease-related event but a more general phenomenon in the context of inflammation, as previously suggested by the model of chronic inflammation in rheumatoid arthritis proposed by Vossenaar et al.13 In view of the recent evidence that antibodies to citrullinated proteins may occur many years before actual onset of clinical symptoms of arthritis and the indications that environmental factors such as smoking may induce both citrullination and anti-citrulline immunity, there is now a need for detailed studies on which molecules are subjected to citrullination in the various inflammatory tissues and for studies on the fine specificity of immune reactions against these citrullinated proteins. Thus, if inflammation in itself is able to induce citrullination, other factors that would contribute to the development of autoimmunity and further inflammation must be present, such as defective B cell tolerance checkpoints,14 genetic background15 or environmental factors.1
Acknowledgments
We thank Marianne Engström for excellent technical assistance. This study was supported by grants from the Swedish Medical Research Council, the Swedish Rheumatism Association, the Insurance Company AFA, the The King Gustav V’s 80 years Foundation, and the Söderberg Foundation.
REFERENCES
Footnotes
-
Published Online First 15 March 2006
-
Competing interests: None declared.