Article Text

Abstract
Objective: To investigate the influence of age on the effectiveness and tolerance of antitumour necrosis factor alpha (TNFα) therapy in rheumatoid arthritis (RA).
Methods: 730 patients of the Dutch Rheumatoid Arthritis Monitoring (DREAM) register were categorised into three groups according to their age at initiation of anti-TNFα therapy (<45, 45–65 and >65 years). Effectiveness of anti-TNFα therapy was primarily assessed by longitudinal analysis of the DAS28 during the first 12 months of treatment.
Results: Improvement in disease activity and physical functioning was significantly less in elderly patients, correcting for relevant confounders. Elderly patients reached the EULAR categories of good responders and remission less often than younger patients. Drug survival, co-medication use and tolerance were comparable between the three age groups.
Conclusion: Anti-TNFα therapy significantly reduced disease activity in all age groups of patients; however, it appeared less effective in elderly compared with younger RA patients.
Statistics from Altmetric.com
Life expectancy is increasing in the western world and the elderly represent an increasing proportion of the rheumatoid arthritis (RA) patient population.1,2,3 Parallel with these demographical changes, the introduction of tumour necrosis factor alpha (TNFα) blocking agents increased treatment goals with aiming for remission.4 This goal might not be easily achieved in the elderly RA population. The physiological and immunological processes of ageing can result in varying clinical responses to therapy and an increased incidence of adverse events.5 The increased production of pro-inflammatory cytokines found in the elderly might lead to a higher incidence of auto-immune diseases, possibly with a more severe phenotype.6,7
Data on the outcome of anti-TNFα therapy in the elderly are limited and mainly originate from post-hoc analysis of randomised clinical trials (RCT) investigating the efficacy of etanercept.8,9,10,11 It is suggested that effects demonstrated in RCT are higher than in clinical practice due to the strict selection of patients.12,13 Therefore, large observational studies with better reflection of the daily clinical practice are needed to investigate effectiveness. Moreover, the proportion of elderly patients in RCT is small in comparison to clinical practice.
The present study investigated the effectiveness and tolerance of anti-TNFα therapy in elderly and younger RA patients during the first year of anti-TNFα treatment, using a large prospective cohort of Dutch RA patients. Treatment decisions following anti-TNFα treatment failure were compared between age groups.
Patients and methods
Study population
The Dutch Rheumatoid Arthritis Monitoring (DREAM) register was used for analysis, which is a multicentre cohort of RA patients starting first-time anti-TNFα treatment. The objective of the register is to monitor the safety, long-term effectiveness and pharmacotherapy in daily clinical practice. Since February 2003, data were prospectively obtained from consecutive patients in 11 hospitals in the Netherlands. Seven of the hospitals included 96–100%, two hospitals included 62–64% and two hospitals included only approximately 45% of their consecutive patients who were eligible for anti-TNF therapy. However, the patients not included in the register did not differ from the patients that were included, with respect to the disease activity score in 28 joints (DAS28), age and gender. The study protocol was approved by the local Ethics Committee.
Evaluation of effectiveness
The primary outcome measure of effectiveness was the course of the DAS28 over 12 months. Secondary outcome measures included the DAS28 at 12 months, the change in DAS28 from baseline to 12 months, the percentages of patients reaching the EULAR criteria for clinical response and remission after 12 months, the longitudinal assessment of functional capacity (health assessment questionnaire; HAQ) and the changes in health-related quality of life assessed by the Short-Form 36 (SF-36) health survey.
Drug survival, tolerance and safety
Survival analysis of the first anti-TNFα agent was performed. Tolerance was assessed by drug discontinuation rates and by examining the incidence of major adverse events and the reasons for discontinuation.
Co-medication use and treatment decisions
The use of methotrexate, oral and intramuscular prednisone was investigated at baseline and during follow-up. Treatment decisions following the discontinuation of anti-TNFα treatment were analysed.
Statistical analysis
Patients were divided into three groups based on their age at the start of anti-TNFα treatment: less than 45 years, 45–65 years and over 45 years. Variables were compared between the groups by one-way analysis of variance, the Kruskal–Wallis test or the χ2 test when appropriate. The course of the DAS28, the HAQ and the SF-36 subscales were analysed by linear mixed models for longitudinal data, corrected for relevant confounders. Age was included as a continuous variable first and then divided into age groups. Variables expected to be important predictors of outcome, including disease duration, rheumatoid factor and baseline DAS28, were included in all models. Methotrexate and oral prednisone use were dichotomised to indicate current use at the time of disease activity evaluation and were handled as time-varying confounders. Interactions were tested between age, gender and disease duration. Multiple logistic regression analysis with calculation of odds ratios (OR) was used to test the influence of age on being a responder, a good responder or achieving clinical remission after 12 months of therapy. Drug survival was analysed using the Kaplan–Meier method.
Results
Patients
By the end of January 2007, 730 patients were included in the register: 146 aged less than 45 years; 388 aged between 45 and 65 years and 196 patients older than 65 years. Twelve patients were lost to follow-up within one year, before discontinuation of anti-TNFα treatment and 81 were censored on 15 February 2007. Table 1 summarises the baseline characteristics.
Baseline characteristics of the three age groups
Effect of age on DAS28
Linear mixed model analysis showed that age had a significant influence on the course of the DAS28 (p = 0.000), also after correction for baseline DAS28, baseline HAQ, disease duration, rheumatoid factor, gender, and current methotrexate and oral prednisone use (p = 0.000). Using age groups in the same model, the improvement in disease activity was significantly less in elderly patients compared with both the middle-aged group (p = 0.022) and the youngest age group (p = 0.001; fig 1A). None of the interactions were significant when included in the model.

Course of (A) the disease activity in 28 joints (DAS28) and (B) the health assessment questionnaire (HAQ) from baseline to 12 months in the three age groups.
Higher baseline DAS28 in the elderly did not fully explain the differences in effectiveness. Figure 1A shows that the DAS28 improved equally in the three groups during the first 3 months of treatment and that the differences emerged mainly after 6 months with more improvement of DAS28 in the youngest age group. At baseline, elderly patients started with a higher DAS28, had less improvement in DAS28 (1.9, 1.7 and 1.5 in young, middle-aged and elderly groups, respectively, p = 0.026), resulting in a significantly higher DAS28 at 12 months (3.03, 3.60 and 4.00, respectively, p = 0.000). Individual parts of the DAS28 at baseline, at 12 months and the change from baseline to 12 months are shown in supplementary table 2 (available online only).
Effect of age on response and remission
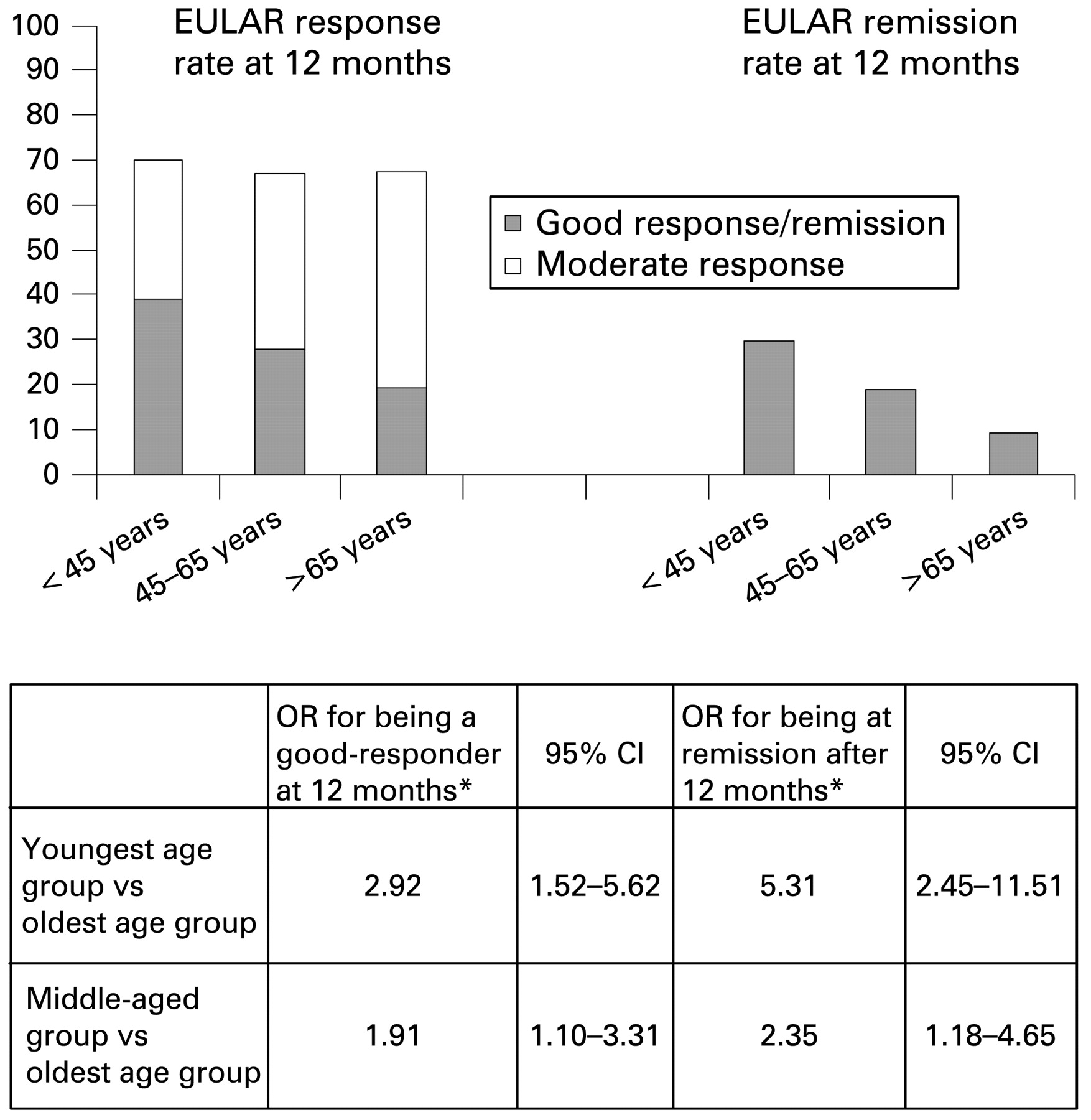
The same proportion of patients in the three age groups had a response—moderate or good—according to the EULAR criteria (SD 65%; fig 2). However, the percentage of elderly patients reaching “good response” or “clinical remission” was significantly lower compared with the younger age groups, which was confirmed by multiple logistic regression. The OR for the different groups are shown in fig 2.
{kind=link}
{kind=link}
EULAR response and remission rates in three age groups. Odds ratios (OR) for the chance of being a good responder or being in clinical remission according to the EULAR criteria. DAS28, disease activity score in 28 joints; HAQ, health assessment questionnaire.
Effect of age on HAQ and SF-36
Improvement in physical functioning (HAQ) was significantly less in elderly patients (p<0.005), controlling for the same confounders as for the DAS28 (fig 1B). Similarly, from the SF-36 subscales, physical-functioning and role-physical showed less improvement in elderly patients (not shown, p<0.05).
Drug survival, tolerance and co-medication use
Drug survival rates were not different between the age groups (p = 0.567); 210 patients (28.7%) stopped using anti-TNFα within the observation time. Dose changes in the three anti-TNF agents, reasons for discontinuation and the incidence of severe adverse events were comparable between the age groups.
Methotrexate was used in comparable frequency and dosage in all age groups. Oral prednisone was used more often by elderly patients (26.7%, n = 39 young; 31.2%, n = 121 middle-aged vs 43.9%, n = 86 elderly; p = 0.001); however, time-averaged doses were comparable. No significant differences were found in dose increase or decrease of oral prednisone.
Treatment decisions following cessation of the first anti-TNFα treatment
Significantly fewer elderly patients switched to a second anti-TNFα agent (15.8%, n = 31 elderly vs 27.9%, n = 108 middle-aged and 31.5%, n = 46 young patients). Also, a higher percentage of elderly patients continued on their previously prescribed disease-modifying antirheumatic drug therapy, without any new medication added to their treatment regime (12.8%, n = 25 elderly; 6%, n = 23 middle-aged and 5.5%, n = 8 young, p<0.005).
Discussion
This study addressed the influence of age on the effectiveness and safety of a first anti-TNFα treatment in RA in daily clinical practice, using a large prospective RA cohort of consecutive starters of anti-TNFα. In this cohort, elderly patients starting anti-TNFα therapy had more severe disease at baseline and showed less improvement in disease activity compared with younger patients, which resulted in approximately 1 point difference in DAS28 at 12 months between the eldest and the youngest groups. Consequently, 20% fewer elderly patients reached the EULAR categories of good responder and DAS28-defined remission than in the youngest group. The 12-month drug survival rates did not differ between the age groups, which might be explained by the equal percentages of non-responders. Less improvement in physical functioning in elderly patients was reflected in both the HAQ and the SF-36. Disease duration, assessed as confounder as well as effect modifier, did not influence the results.
The efficacy of etanercept treatment in the elderly RA population was previously demonstrated in post-hoc analysis of RCT.8,9,10,11 However, the results obtained from RCT cannot be applied directly to all patients encountered in clinical practice, as RCT generally have a highly selected trial population with a very low percentage of elderly included.12 Our study used a representative clinical care population with a high percentage of elderly patients treated with one of the three anti-TNFα agents.
One observational study from Switzerland found similar results to ours regarding EULAR response and improvement in functional capacity.14 However, DAS28 changes were similar in the age groups, leading to the conclusion that age did not influence effectiveness.
During the past decade, RA treatment has become more ambitious by aiming for remission.15,16 Therefore, our finding of a lower remission rate in the elderly is relevant.
Patients with greater disease activity at baseline might have more difficulty reaching the threshold of DAS28-based remission. However, when correcting for a high baseline DAS28, the chance of reaching remission was still significantly lower in the elderly group.
Our results suggest that treatment goals are not as easily achievable in elderly as in younger RA patients. Physiological and immunological changes of senescence and decreased compliance in patients with multi-medication might play a role in this. Nevertheless, the large effect also in elderly patients and the comparable incidence of adverse events in the three age groups leads to the conclusion that anti-TNF treatment remains justified in elderly RA patients.
Acknowledgments
The authors are indebted to all research nurses and rheumatologists of the 11 departments of rheumatology for their participation and contribution in the data collection: J Alberts, P Barrera Rico, M Creemers, J Deenen, A van Ede, T van Gaalen, E de Groot, H van Heereveld, F van den Hoogen, L Schalkwijk, C Versteegden, C Vogel, M Vonk (Radboud University Nijmegen Medical Centre, Nijmegen); H Cats, A Eijsbouts, M Franssen, I Geerdink, S Hol, F van den Hoogen, M Jeurissen, P Koopmans, P van ’t Pad Bosch, D de Rooij, A Stenger, H van Wijk (Sint Maartens Kliniek, Nijmegen); T Berends, C Bijkerk, C De Gendt, J Harbers, M Janssen, A de Jong, H Knaapen, H Visser (Rijnstate Hospital, Arnhem); A ter Avest, K Drossaers, M Hoekstra, M Kruijssen, I Kuper, A Mooij, H Vonkeman (Medisch Spectrum Twente, Enschede); H Bernelot Moens, E Bos, K Drossaert, C Haagsma, K van de Hoeven, J Oostveen (Twenteborg Ziekenhuis, Almelo); M Kleine Schaar (Streekziekenhuis Midden Twente, Hengelo); J de Boer, H van de Brink, S Erasmus, J Moolenburgh, W Swen (Medical Centre Alkmaar, Alkmaar); I Henkes, H Hulsman, K Ronday (Leyenburg Hospital, Den Haag); M Geurts, J Haverman, P van Oijen, N Wouters (Jeroen Bosch Hospital, Den Bosch); GAW Bruyn, EN Griep, PM Houtman, A Spoorenberg, A Krol, J Woudwijk (Medical Centre Leeuwarden, Leeuwarden); R van Berkel, H Brus, W Hissink Muller, A van Roy, M. Wijnands (Twee Steden Hospital, Tilburg).
REFERENCES
Supplementary materials
Web only appendix 68;9:1470
Footnotes
▸ Additional supplemental table 2 is published online only athttp://ard.bmj.com/content/vol68/issue9
Funding Funding from the Dutch National Health Insurance Board and the Dutch affiliations of Wyeth Pharmaceuticals, Abbott Pharmaceuticals and Roche Pharmaceuticals enabled the data collection for the DREAM study.
Competing interests None.
Ethics approval The study protocol was approved by the local Ethics Committee.