Article Text

Abstract
Objective: To estimate the annual incidence of inflammatory joint diseases in a population based prospective referral study in an adult population in Kronoberg County in southern Sweden.
Methods: The patients were referred from primary healthcare centres to the rheumatology department in Växjö Central Hospital or to the one private rheumatologist in Växjö participating in the study. Additionally, the hospital records for patients with joint aspirates during the inclusion period were checked. The patients were registered as incident cases if the onset of the joint inflammation was between 1 May 1999 and 1 May 2000. A systematic follow up of incoming referrals was conducted up to 31 January 2001. Children under the age of 16 and patients with septic arthritis, crystal arthropathies, and osteoarthritis were excluded from the study.
Results: A total of 151 new cases with inflammatory joint diseases were identified during one year, corresponding to a total annual incidence of 115/100 000. Of these, 31 patients (21%) had rheumatoid arthritis, the annual incidence being 24/100 000 (for women 29/100 000, and for men 18/100 000). Reactive arthritis was diagnosed in 37 patients (24%, annual incidence 28/100 000) and 54 patients had undifferentiated arthritis (36%, annual incidence 41/100 000). Eleven patients presented with psoriatic arthritis (7%, annual incidence 8/100 000). The incidence of Lyme arthritis was small in this non-endemic area, and the incidence of sarcoid arthritis corresponded to that in earlier studies.
Conclusion: This is the first prospective population based annual incidence study of early arthritis in Sweden. In this population, 36% of the incident cases had undifferentiated arthritis, whereas rheumatoid arthritis and reactive arthritis accounted for 45% of the cases. The incidence figures compare well with figures reported from other countries.
- incidence
- epidemiology
- rheumatoid arthritis
- spondyloarthropathy
- ACR, American College of Rheumatology AS
- ankylosing spondylitis
- MCTD, mixed connective tissue disease
- PsA, psoriatic arthritis
- RA, rheumatoid arthritis
- ReA, reactive arthritis
- SLE, systemic lupus erythematosus
Statistics from Altmetric.com
- ACR, American College of Rheumatology AS
- ankylosing spondylitis
- MCTD, mixed connective tissue disease
- PsA, psoriatic arthritis
- RA, rheumatoid arthritis
- ReA, reactive arthritis
- SLE, systemic lupus erythematosus
The annual number of new cases of inflammatory joint disease in a defined population has major implications for the planning of rheumatology health care. Different methods for estimating the incidence of inflammatory joint diseases have been applied in rheumatological epidemiology.
Two earlier population based studies of inflammatory joint diseases from Finland gave a total rate of inflammatory joint disease of 65–218/100 000. The studies were based on drug reimbursement for chronic joint inflammation and two patient series combined.1,2 The second study also included gout and osteoarthritis.
A prospective notification of referrals of new patients with rheumatoid arthritis (RA),3 prospective and retrospective estimates of RA incidence with the help of RA registers,4,5 retrospective studies of hospital records,6–9 and studies of patients with drug reimbursement10 are examples of earlier incidence studies on RA, giving an incidence of 13–66/100 000 for women and 5–28/100 000 for men. A high incidence of RA of 42 cases/10 000 person-years has been reported from a Pima Indian reservation.11 There have also been reports of a declining incidence in RA,3,6,10,12 but this has not been verified in other studies.9,13
The incidence of ankylosing spondylitis (AS) has been reported to be 6.6–10/100 000.14–16 The studies on the incidence of psoriatic arthritis (PsA) are difficult to interpret because of the lack of defined criteria, but incidence rates of 6–7/100 000 have been reported.17,18 The incidence of postenteric reactive arthritis (ReA) in Finland has been estimated as 14/100 000, and postvenereal ReA as 13/100 000, the total incidence being 27/100 000.2
In Sweden, all medical care is subject to governmental control and is available to the entire population. The country is divided into seven regions consisting of neighbouring counties. Each region has a large referral hospital, and each county (in total 21) has a council (“ landsting “) responsible for health care. Health care within the counties is further divided into varying numbers of healthcare districts—which usually have their own primary healthcare centre—and a local district hospital. As a rule, each primary healthcare centre has several general practitioners. Private practitioners are rather uncommon, and those who are established are generally attached to and supported by the county council. Specialist health care is accessible to all and referral is easy.
At the time of the study, the county of Kronoberg in southern Sweden (Småland) (fig 1) had a population of 177 000, and the number of inhabitants over 16 years of age was 140 000. The population count for 2000 was used as the population is stable. This county has two hospitals, the Central Hospital in Växjö, and the local district hospital in Ljungby. The rheumatology department is located in Växjö Central Hospital. At the time of the study there was one privately practising rheumatologist in this county (OB), and he participated in the study. Some rheumatological patients were also treated at Ljungby District Hospital, but there was no specialist in rheumatology in the hospital. Thus, in this county, the care of patients with active rheumatological diseases who need specialist treatment is concentrated either in the rheumatology department in Växjö Central Hospital or with the one private practitioner participating in the study. The county has 25 primary healthcare centres.

Map of Scandinavia showing Kronoberg county.
In Sweden, patients with early inflammatory joint diseases are initially taken care of by general practitioners at the primary healthcare centres. Crystal deposition diseases and osteoarthritis are primarily treated at the primary healthcare centres. However, the policy in Sweden for all cases of early arthritis of unknown cause, as well as all patients with acute or subacute polyarthritis, is that of a rapid referral from the primary healthcare centres to a rheumatologist for confirmation of the diagnosis and consideration of further therapeutic strategies. Quick referral to a rheumatologist has been particularly stressed in cases of suspected RA and is a generally agreed treatment principle in Sweden. In general, patients with ongoing inflammatory joint symptoms are treated at rheumatology departments, and not referred back to the primary healthcare centres.
The aim of this prospective population based incidence study of new referrals was to examine the annual incidence of inflammatory joint diseases in the adult population of 132 000 in the county of Kronoberg in southern Sweden between May 1999 and May 2000.
PATIENTS AND METHODS
The incoming patients were included as incident cases in the study if they had a new joint inflammation with swelling of at least one joint, were over the age of 16, and provided that the onset of the joint inflammation occurred between 1 May 1999 and 1 May 2000. Children aged 16 or under and patients with osteoarthritis, septic arthritis, and crystal deposition diseases were excluded from the study. Patients with a history of joint swelling before May 1999 were excluded. The general practitioners in the participating primary healthcare centres referred the patients either to the outpatient clinic at the rheumatology department in Växjö Central Hospital or to the private rheumatologist in Växjö (OB). Some of the patients included in the study were admitted to the rheumatology department in Växjö Central Hospital from the emergency department of the hospital and from other clinics. Only patients resident in this county were included in the study. It was not possible to identify patients who resided in this county but accessed care in other counties or were referred to centres outside this county.
The patients were followed up according to normal practice at the rheumatological unit's outpatient clinic, at the private practice of the rheumatologist, or, in patients admitted to hospital, in accordance with normal practice in the wards. As some of the patients might present several months after the onset of the joint symptoms, the incoming referrals to the rheumatology unit and the private practitioner were systematically checked until 31 January 2001.
Altogether, 21 primary healthcare centres, one private outpatient rheumatology unit, and all specialised units at Växjö Central Hospital and at Ljungby District Hospital where patients with inflammatory joint diseases might present (for example, departments of internal medicine, orthopaedics, dermatology, and infectious diseases) participated in the study. The coverage area encompassed an adult population (>16 years) of 132 000 people. One of the authors (MS) personally visited the general practitioners in each participating primary healthcare centre and the doctors in the participating clinics in the hospitals to inform them about the study before the start. Rapid referral to a rheumatologist in appropriate cases was particularly stressed. In addition, all participating centres received written information. The department of orthopaedics and the dermatologist in Ljungby District Hospital received only written information. Additionally, other privately practising physicians with specialties other than rheumatology in Växjö were given written information about the study before the start. All participating primary healthcare centres and clinics also received regularly, at three month intervals, a written reminder of the study. This contained the inclusion criteria and a report of the number of included patients and their diagnoses so far.
After inclusion in the study, the diagnosis of the arthritis was conducted as follows. All of the patients defined as having RA fulfilled the 1987 ACR (American College of Rheumatology) criteria.19 Radiographs of the inflamed joints, usually the hands and feet, were taken of all the patients with suspected RA at presentation. Psoriatic arthritis was defined as psoriasis in association with arthritis, with a negative test for rheumatoid factor.20 The criteria for Lyme arthritis was a history of monoarthritis or oligoarthritis with no alternative explanation and with a positive serology for Borrelia burgdorferi as analysed by the enzyme immunoassay at the local microbiology laboratory.21 Reactive arthritis was defined as an inflammatory joint disease either preceded by an infection and verified by cultures or positive serology, or, in the absence of a history of infection, by cultures or serology alone. The patients with joint inflammation not meeting the above criteria were classified as cases of undifferentiated arthritis. As some of the patients were treated in other clinics and not seen by us, systematic screening for infections was difficult. The diagnoses were clinical. All of the patients did not have radiography of their hands and feet, nor was there a systematic analysis for recent infections or rheumatoid factor.
To obtain more reliable incidence data, and to achieve an estimate of the referral bias in the study, the hospital records of the patients who had been subjected to a joint fluid aspiration during the time of the inclusion (1 May 1999 to 1 May 2000) were also checked.
The study was approved by the regional ethics committee at the University of Lund. The registration of the patients for the incidence study was approved by the Växjö Central Hospital's leading committee as a patient data register.
The estimates were calculated with 95% confidence intervals (95% CIs) using a Poisson distribution.
RESULTS
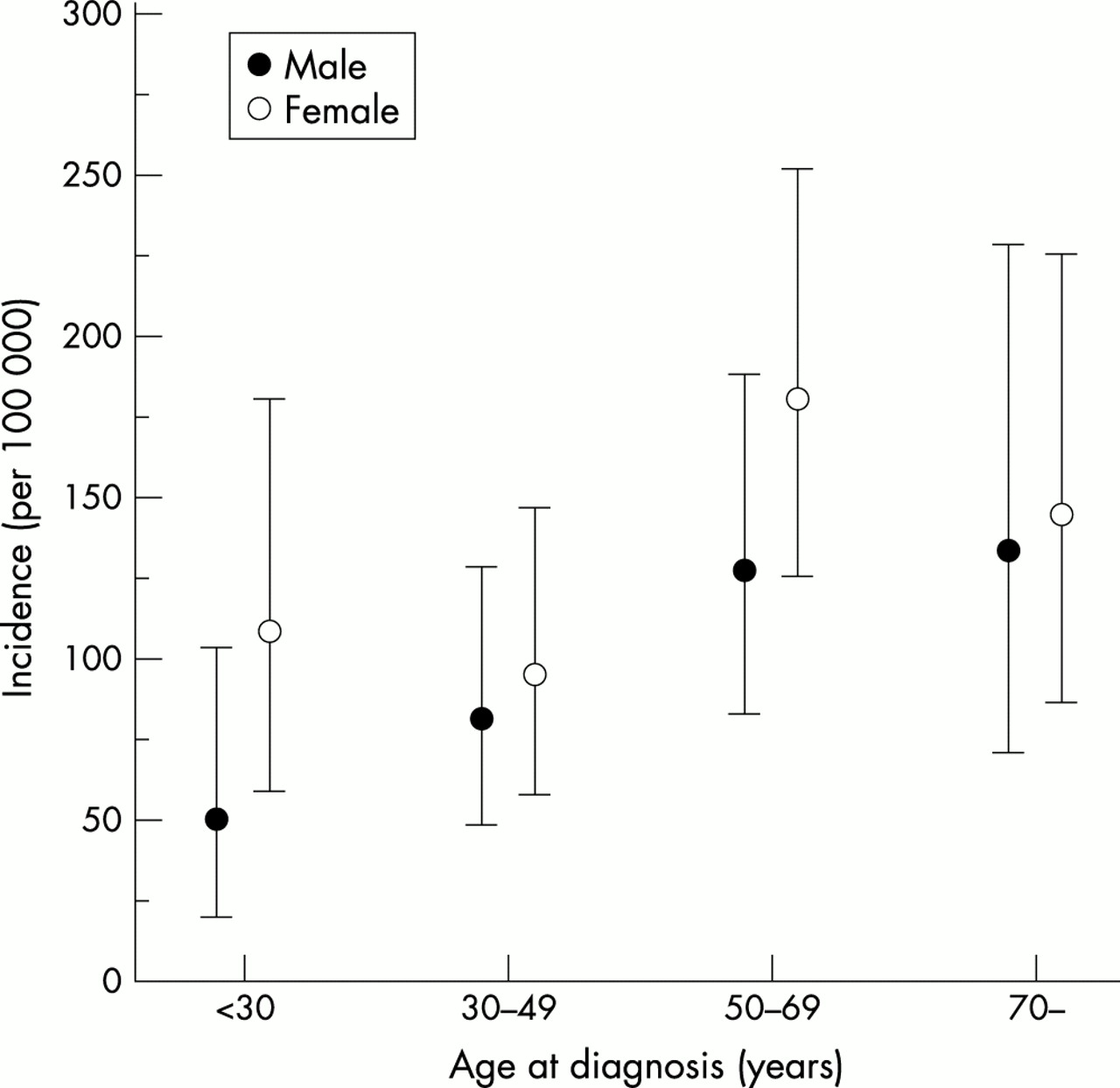
A total of 151 patients were registered as incident cases with a new inflammatory joint disease. This gave a total annual incidence for inflammatory joint diseases of 115/100 000 (95% CI 97 to 134) (table 1). Figure 2 shows the age specific annual incidence for the entire patient population. The median duration of symptoms from onset to inclusion in the study was two months (range 0–17, interquartile range 1,3). Forty eight patients (32%) had a monoarthritis.
Absolute numbers and annual incidences/100000 of inflammatory joint diseases in Kronoberg county in southern Sweden
{kind=link}
{kind=link}
Age specific annual incidence of inflammatory joint diseases in southern Sweden, with 95% confidence intervals.
Thirty one patients (21% (95% CI 14 to 28)) fulfilled the ACR 1987 diagnosis criteria for rheumatoid arthritis. The patients were registered as incident cases of RA when the ACR 1987 criteria were met by 31 January 2001, and the symptoms had started between 1 May 1999 and 1 May 2000. Twenty seven of the patients with RA fulfilled the ACR criteria for RA 12 months from inclusion, and four fulfilled the ACR criteria during the study period. This gave a total annual incidence for RA of 24/100 000 (95% CI 16 to 33). Nineteen patients were women, and 12 patients were men, the incidence being 29/100 000 and 18/100 000, respectively. The mean age of the patients was 60 (SD 15). All patients were white. Of the total patient group, 17 were seropositive and 14 were seronegative. Additionally, nine patients, two men and seven women, were clinically classified as having RA but did not satisfy the ACR criteria during the study period; they were classified as having undifferentiated arthritis. If these patients were included in the calculation of incidence of RA, the total annual incidence was 30/100 000 (95% CI 22–41); for women it was 39/100 000 (95% CI 26–57), and for men 21/100 000 (95% CI 12–36).
Eleven patients (7% (95% CI 4 to 13)) were diagnosed as having psoriatic arthropathy, giving an incidence of 8/100 000 (95% CI 4 to 15). Of these, eight were women and three were men. The mean age at diagnosis was 52 (SD 21). All patients with a diagnosis of psoriatic arthritis tested seronegatively for rheumatoid factor.
Thirty seven (24% (95% CI 20 to 31)) of the patients had reactive arthritis, giving an incidence of 28/100 000 (95% CI 20 to 39). Twenty four patients had postenteric ReA (incidence 18/100 000), one patient had a genitourinary ReA, six had ReA caused by other diseases (staphylococcal soft tissue infection (two), tooth root infection, Escherichia coli septicaemia, urosepsis, mastitis (one each)), and six patients had an acute upper respiratory tract infection as the cause. The total incidence for genitourinary ReA, ReA from other causes, and ReA caused by respiratory tract infection was 10/100 000.
Fifty four (36%(95% CI 29 to 45)) of the patients had undifferentiated arthritis, giving an incidence of 41/100 000 (95% CI 31 to 54). Three patients had the clinical diagnosis of Lyme disease. Three patients had acute sarcoid arthritis, giving an incidence of 2/100 000 (95% CI 0 to 7). All patients with sarcoid arthritis were men, and the diagnoses were clinical. The patients presented with acute arthritis and had enlarged hilar lymph nodes on chest radiography. Biopsies were not performed.
Twelve (8%(95% CI 4 to 13)) of the patients had varying diagnoses, comprising temporal arteritis (one), Henoch-Schönlein's purpura (three), systemic lupus erythematosus (SLE) (two), polymyalgia rheumatica (two), erosive osteoarthritis with synovitis (one), ankylosing spondylitis (two), and mixed connective tissue disease (MCTD) (one).
Several patients had two or more diagnoses. The patient with a new MCTD also had serological signs of Borrelia burgdorferi infection, and she also had an episode of temporal arteritis clinically, whereas her temporal artery biopsy was negative. One patient who registered as having a Campylobacter jejuni ReA also had a history of back pain without previous peripheral synovitis four years previously, and she also had radiological sacroiliitis.
Thirty three patients in the study had a joint aspiration (22%). Seven patients were identified through the hospital records for joint aspirates, giving the referral bias of 5%. These patients had an acute arthritis during the inclusion period but were not referred to a rheumatologist.
DISCUSSION
This prospective population based referral study addresses the annual incidence of inflammatory joint diseases in an adult population of 132 000 in southern Sweden. Overall, the incidence rates in our study compare well with the incidence rates reported in previous studies.
The strength of our study was the very good cooperation between general practitioners and rheumatologists in this area. The primary healthcare centres were continuously informed and updated. Also, the need for a quick referral of patients with inflammatory joint diseases to a rheumatologist has wide acceptance in the Swedish healthcare system. To estimate the referral bias, we also screened the hospital records of patients with joint aspirates during the inclusion phase. To minimise the referral bias, we also registered patients in other than rheumatological centres, where patients with joint symptoms might present—for example, the orthopaedics departments. However, the fact that patients in this incidence study were also seen and treated in other clinics than ours presented a bias in the study, as a systematic screening for infections was difficult, and all of the patients did not have radiography.
One caveat in our study is the inclusion time of one year, which may be too short. Because infections in the normal population may vary seasonally and from year to year, perhaps a longer inclusion period would have levelled out this bias. Additionally, we screened incoming referrals up to the end of January 2001—that is, eight months after stopping the inclusion. This may also be too short a time, as RA often starts insidiously, and patients might present months or even years after the initial symptoms. Concerning referral bias, the cases that were missed in this incidence study were most probably subacute with few symptoms, as acute monoarthritis and polyarthritis, and particularly more chronic joint disease lasting weeks or months, are usually rapidly referred from general practitioners to rheumatologists. Other cases that we missed were most likely spontaneously resolving short lived joint inflammations where the patient did not seek medical help. We probably also missed some cases where patients sought medical attention either at the primary healthcare centre or at another specialist unit, without being referred to a rheumatologist. However, although all of the patients did not have radiography, it is very likely that the referral bias for patients with RA was small, as it is an accepted treatment principle in Sweden to refer patients with this diagnosis to rheumatologists.
Seven patients were identified through the hospital records for joint aspirates, and the referral bias calculated from this is 5%. Two of these patients had an ReA and five had a diagnosis of undifferentiated arthritis. The true number of missed incident cases in this study is very difficult to estimate, and the estimate of 5% referral bias is probably an underestimate.
This is the first annual incidence study of RA in Sweden. Our results are in agreement with incidence rates reported from earlier population based studies from other countries, and identical to the incidence rates found in the TIRA study, another ongoing Swedish early arthritis cohort (unpublished results). In incidence studies of RA, two biases have to be noted: firstly, the bias of late presentation, and secondly, the slow accumulation of the ACR criteria. The first bias has been discussed above. As not all patients with early RA meet the ACR 1987 criteria at presentation, there have been discussions as to whether the incidence date should be the date of the symptom onset, the date when the patient met the ACR criteria, or the date when the patient presented.22 We chose an approach whereby the patient was registered as an incident case when the symptoms started between 1 May 1999 and 1 May 2000, and the ACR criteria were met by 31 January 2001—that is, a cumulative incidence. All patients with RA in this study recalled the month when their symptoms first appeared, and 27 patients fulfilled the ACR RA criteria 12 months from inclusion. This is the third study where the onset of symptoms is registered as the incidence date.6,22
Several patients in this study had clinical RA with a negative infection screen but did not meet all of the ACR 1987 criteria, so these patients were classified as cases of undifferentiated arthritis. A prospective study such as this, with an initial short follow up, underestimates the true incidence of RA, and a cumulative incidence during a longer follow up is required. A follow up study starting in 2001 will answer the question of how many patients with the diagnosis of undifferentiated arthritis in this study will later on develop RA.
The lack of universally accepted diagnostic criteria for psoriatic arthritis hampers epidemiological studies. We used the diagnostic criteria from Moll and Wright.20 There are only a few other studies addressing the incidence of psoriatic arthritis in a population based setting, giving incidence rates of 6 to 7/100 000 inhabitants, close to our result, 8/100 000.2,17,18 Our study also includes mild cases of psoriatic arthritis, as the patients were referred to a specialist early in the disease to establish diagnosis regardless of severity of illness. We hope the follow up study will also address the question of a “cumulative” incidence of psoriatic arthritis, as some of the patients presenting with arthritis develop psoriatic nail and skin changes after the onset of joint symptoms, and are most probably initially classified as having undifferentiated arthritis.
The incidence of Lyme arthritis was low in our study. Småland does not seem to be an endemic area for Lyme disease compared with, for example, the coastal area of Blekinge about 100 km south of Småland. However, 14% of healthy blood donors in Kronoberg were seropositive for Borrelia burgdorferi in 1996 (unpublished information, Department of Microbiology, Växjö Central Hospital). The seropositivity for Borrelia burgdorferi in the normal population of Aspö island in Blekinge archipelago has been reported to be 19%, and the prevalence of Lyme arthritis there 2.3%.23
Only three patients, all men, had the diagnosis of acute sarcoid arthritis in our study, giving an incidence of 2/100 000, which corresponds to the figures published earlier from Oslo in Norway, 2.9/100 000.24 All diagnoses were clinical. Two of our patients presented during the winter and one in spring. The absolute numbers in our study are obviously small and no conclusions can be drawn as to, for example, seasonal variation of sarcoid arthritis.
There are only a few studies addressing the incidence of ReA in a population based setting, giving incidence rates of 4.6–13/100 000 for postvenereal ReA and an incidence of 5–14/100 000 for postenteric ReA.2,25 Our study included the whole range of ReA with both mild and severe cases, some of which developed into chronic cases, and the total annual incidence was 28/100 000. We expected to see ReA in this proportion, as the duration of the symptoms to the inclusion was relatively short, and almost a third of the patients had monoarthritis. In a Finnish study, the incidence of chronic ReA necessitating reimbursed medication was 2.2/100 000, probably, as the author comments, representing a minimum figure.1 The incidence of postenteric ReA was 18/100 000, with Campylobacter jejuni being the predominant causal agent. Very surprisingly, the incidence of postvenereal ReA in this study was extremely low (one case). One patient had urine positive for Chlamydia trachomatis by polymerase chain reaction three months after inclusion, but a negative test at the inclusion, and was classified as having undifferentiated arthritis. The difference in incidence rates compared with other studies may be due to a true difference in incidence—for example, because of different frequencies of HLA-B27 in the populations—or the use of different laboratory methods, referral bias, incomplete screening, or patient selection. There were no epidemics in Sweden during the time of inclusion in this study. We classified the patients with negative cultures and serology as having undifferentiated arthritis, using quite strict criteria. According to other study designs, some of our patients with negative cultures and negative serologies would have been classified as having “reactive arthritis of unknown origin” or “possible ReA”.1
The incidence of undifferentiated arthritis was 41/100 000 in our study. A population based study on chronic undifferentiated arthritis found an incidence of 13/100 000.1 There seems to be a consensus in the literature that this is a poorly defined disease entity, probably including cases in their early stages of development to, for example, RA, abortive or self limiting disease, overlap diseases, and ReA after either unknown or viral agents, and probably some of these cases are also misclassified as seronegative RA.25,26 In the published studies of cohorts of early arthritis, undifferentiated arthritis forms 20–60% of cases, and seems to have a positive prognosis, as over 50% go to partial or total remission.2,26–31 Hopefully, our follow up study will also elucidate the question of prognosis of patients with undifferentiated arthritis, especially development into RA and remission.
The incidence of ankylosing spondylitis in our study was, as expected, low, and not representative of the true incidence of the disease. We found only two female patients with clinically distinct ankylosing spondylitis. A third female patient had a clear new sacroiliitis, presenting with a spondylarthropathy-like disease caused by a Campylobacter jejuni infection. She was classified as having ReA. One patient, as mentioned above, had a distinct radiological sacroiliitis not diagnosed previously, and she was also classified as a patient with ReA. The diagnosis of sacroiliitis of recent onset is difficult, and we presume that many of these patients are initially referred from the primary healthcare centres to orthopaedic surgeons. Furthermore, it usually takes years before the typical radiological changes develop, and the mean time from the onset of the symptoms to diagnosis has been reported to vary from 3.7 to 10 years.14,15 The incidence of SLE in this study is, likewise, not representative of the true incidence, as only patients with arthritis were registered as incident cases.
In summary, we present the first annual incidence rates of rheumatoid arthritis, psoriatic arthritis, reactive arthritis, and undifferentiated arthritis in Sweden in a population based setting. Thirty six per cent of the patients had undifferentiated arthritis, and 21% and 24% had rheumatoid arthritis and reactive arthritis, respectively. A policy of quick referral of the patients with new joint inflammation to a rheumatologist can be accomplished by good cooperation with general practitioners and specialists, and the referral bias seemed to be small. This benefit the patients as early diagnosis and the early initiation of treatment are vital.
Acknowledgments
The study was supported by research grants from the Swedish Rheumatology Association, the Research Council of Kronoberg (FoU-Center), and Region Skåne. We thank Inger Westholm and Monika Lönnqvist for invaluable help.