Article Text

Abstract
Background The phase of arthralgia is the earliest moment to clinically recognize patients who may develop Rheumatoid Arthritis (RA). Previous imaging studies in the arthralgia phase have shown that inflammation precedes RA development. It is unknown which symptoms/characteristics relate to subclinical joint inflammation as measured by MRI. Among all patients with arthralgia, those with clinically suspect arthralgia (CSA) are suspected to progress to arthritis according to the clinical judgement of their rheumatologists. We determined the symptoms/characteristics of patients with CSA who had inflammation on MRI.
Methods 102 patients with CSA and without clinical arthritis were included. They completed questionnaires, underwent joint counts and unilateral 1.5 T MRI of MCP joints 2–4, wrist and MTP joints 1–5. Synovitis, bone marrow oedema (BME) and tenosynovitis were scored according to the OMERACT rheumatoid arthritis MRI scoring system. Symptoms and signs were related to MRI inflammation (based on MRI scores in symptom-free controls; a sum of synovitis, BME and tenosynovitis scores ≥3 was considered positive). Whether certain clinical characteristics frequently occurred together with MRI inflammation was studied by partial least squares analysis.
Results MRI was performed in 93 patients with CSA, 44% of whom had subclinical MRI inflammation. Synovitis was the most prevalent inflammatory feature on MRI (20%). Patients with MRI inflammation were older and were more frequently positive for anti-citrullinated peptide antibodies than patients without MRI inflammation (p<0.001 and 0.049). In PLS analysis, including 16 clinical and serological characteristics as independent variables and MRI inflammation as dependent variable, no clear clusters of patients with and without MRI inflammation were identified.
Conclusions Subclinical inflammation as measured by MRI is present in 44% of patients with CSA. A combination of symptoms/characteristics incompletely differentiated patients with and without MRI inflammation.
- Magnetic Resonance Imaging
- Inflammation
- Arthritis
- Rheumatoid Arthritis
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA) has a period of preclinical disease. According to a recent EULAR study group, this period can be split into several phases—namely, genetic and environmental risk factors for RA, systemic autoimmunity associated with RA, symptoms without clinical arthritis and unclassified arthritis.1 Although genetic and serological risk factors for RA have been extensively studied,2 ,3 the phase of symptoms without clinical arthritis is relatively unexplored. The type of arthralgia and concomitant symptoms that are characteristic of a preclinical phase of RA have not yet been studied. Also, regularly used terms such as inflammatory arthralgia are not uniformly defined.
Early treatment of RA and thus early identification of disease is associated with improved disease outcome.4 ,5 Hence, there is a need to characterise the patients with arthralgia who are actually at risk of RA in order to identify them from the many patients presenting with arthralgia to rheumatology outpatient clinics.
Previous studies on the preclinical phase of symptoms without clinical arthritis evaluated patients with any arthralgia who had an increased risk of RA because of the presence of anti-citrullinated peptide antibodies (ACPA) or rheumatoid factor (RF). Of these patients, 18–35% developed arthritis after a median follow-up of around 12 months.6–8 As only 60% of patients with RA are ACPA-positive9 and ACPA are also prevalent in the population who do not progress to RA,10 ,11 we decided to study the preclinical phase with a different approach. We started from a clinical point of view and evaluated patients presenting with recent-onset arthralgia that was, according to the rheumatologist, clinically suspected to progress to RA over time; this was called ‘clinically suspect arthralgia’ (CSA). Whether or not a patient had CSA was decided by the treating rheumatologist at the first visit before any laboratory results were known; having autoantibodies was not a requirement for having CSA.
It is known that systemic markers of inflammation are increased in the preclinical phase of RA.6 ,12–18 Local inflammation in small joints has also been observed using different imaging technologies.19–21 MRI is a sensitive tool and is more sensitive than physical examination to measure local inflammation.22 It detects synovitis, bone marrow oedema (BME), this is also called osteitis and tenosynovitis, and is most suitable for evaluating the earliest inflammatory changes in the small joints of patients considered potentially to be in the preclinical phase of RA.23 ,24
Our ultimate aim is to identify patients with RA at the stage of having symptoms without clinical arthritis. In this study we considered the presence of local subclinical joint inflammation on MRI as a proxy for RA-at-risk. We aim to describe the characteristics of patients with CSA and to investigate in these patients the symptoms, signs and laboratory markers that are related to subclinical local inflammation visualised by MRI.
Methods
Clinically suspect arthralgia (CSA) cohort
The CSA cohort is a population-based inception cohort started in April 2012 at the rheumatology outpatient clinic in Leiden, The Netherlands, with the aim of studying the preclinical phase of RA. The Leiden University Medical Center is the only rheumatology referral centre in a healthcare region of 400 000 inhabitants. The inclusion criterion was the presence of arthralgia of the small joints for <1 year which, because of the character of the symptoms, was considered by the rheumatologist as being suspect to progress to arthritis over time. Thus, inclusion was essentially based on the ‘gut feeling’ of the rheumatologist. As it is not known which symptoms are predictive for arthritis development, no further criteria were included with regard to the type of symptoms. Importantly, when clinical arthritis was present at physical examination or another explanation for the arthralgia was likely such as Heberden's or Bouchard's nodes or tender points, the patients were not included.
The set-up of the rheumatology outpatient clinic of the Leiden University Medical Center is uniquely suited to identify patients in an early disease phase. For several years general practitioners have been encouraged to send any patient with a suspicion of arthritis to our outpatient clinic. The focus on early recognition was enhanced by the institution of an Early Arthritis Recognition Clinic (EARC) in 2010.25 Although the aim of this EARC was to improve early detection of clinically detectable arthritis, it also provided the opportunity to identify patients with clinically suspect arthralgia.
At the first visit to the rheumatology outpatient clinic a senior rheumatologist or rheumatologist in training supervised by a senior rheumatologist decided, based on the findings of anamnesis and physical examination, whether a patient had clinically suspect arthralgia. After informed consent and inclusion, the rheumatologist completed questionnaires regarding the presenting symptoms (onset, character, localisation), current symptoms (inflammatory character, morning stiffness, fatigue) and medical and family histories. Patients filled out questionnaires regarding social status, smoking, alcohol use and work ability, the Health Assessment Questionnaire (HAQ), the Short-Form health survey-36 (SF-36) and the perceived stress scale. A 66-swollen joint count and 68-tender joint count (66-SJC and 68-TJC) were performed by trained research nurses. Blood samples were taken for routine diagnostic laboratory screening (including C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), IgM-RF and ACPA (anti-CCP2, Eurodiagnostica, The Netherlands) and stored to determine other serum markers at a later time. An MRI was performed when no contraindications for MRI were present. Patients were followed longitudinally for the development of arthritis for at least 2 years with scheduled visits at 4, 12 and 24 months. If considered necessary (eg, if patients noticed swollen joints), patients were seen in between the scheduled visits by their rheumatologist. At each follow-up visit, questionnaires were completed, joint counts were performed and blood samples taken. Follow-up ended earlier when arthralgia had progressed to clinical arthritis. This study evaluated baseline data.
MRI scanning and scoring
MRI of the hand (wrist and metacarpophalangeal (MCP) joints) and forefoot (metatarsophalangeal (MTP) joints) was performed within 2 weeks of clinical assessment at the most painful or, in the case of equally severe symptoms on both sides, the dominant side. Patients were asked not to use any non-steroidal anti-inflammatory drugs (NSAIDs) during the 24 h before MRI. The joints were scanned with an MSK-extreme 1.5 T MRI-scanner (GE, Wisconsin, USA). For the MCP joints and wrist the following sequences were acquired: coronal T1-weighted fast spin echo (FSE) and T2-weighted FSE with frequency selective fat saturation (fatsat) and, following intravenous administration of 0.1 mmol/kg gadolinium contrast, coronal and axial T1-weighted FSE fatsat. For the MTP joints, axial T1-weighted FSE and T2-weighted FSE fatsat sequences were obtained. Because of time limitations, post-contrast and coronal sequences were initially not obtained for the MTP joints. After 78 MRIs had been performed, post-contrast and coronal sequences were also performed in the feet (see online supplementary file 2 for a detailed scan protocol).
Synovitis and BME were scored according to the Outcome Measures in Rheumatology Clinical Trials (OMERACT) rheumatoid arthritis MRI scoring system (RAMRIS).23 Although the RAMRIS was not developed to score MTP joints, others have previously adapted the RAMRIS to score MTP joints as well.26 Tenosynovitis in the MCP joints and wrists was assessed as described by Haavardsholm et al.24 Scoring was performed by one trained reader (HWvS) who was blinded to clinical data; the within-reader intraclass correlation coefficient for the total RAMRIS score was 0.94 and for the combined inflammation score was 0.91. The combined inflammation score (sum of the synovitis, BME and tenosynovitis scores) was the main measure of local subclinical MRI inflammation. The cut-off for the presence of MRI inflammation was defined using the MRI scores (scored by HWvS) of 19 symptom-free healthy subjects of comparable age and gender (mean age of controls 46 years, 79% women) who underwent MRI of the MCP, wrist and MTP joints on the dominant side, as described previously.20 A combined inflammation score of ≥2, ≥3 and ≥4 was present in 21%, 10% and 0% of these healthy subjects, respectively. Based on this, a cut-off of ≥3 was primarily used.
Statistical analyses
MRI scores were studied after dichotomisation. Characteristics were compared using χ2 tests, unpaired t tests and Mann–Whitney U tests as appropriate.
To explore whether a combination of certain clinical and serological characteristics frequently occurred together in patients with subclinical MRI inflammation, partial least squares discriminant analysis (PLS-DA) was used. PLS analysis does not test the statistically significance of differences between groups but is a variable reduction technique. It combines variables that frequently occur together in the so-called latent factors and presents for each factor the variance in the outcome that is explained by this factor. Ideally, one finds a few latent factors that explain most of the observed variance. PLS-DA is the variant of PLS with a categorical outcome. Gender, age, presence of family history of RA, symptom characteristics (duration, onset, localisation, morning stiffness), 68-TJC, body mass index (BMI), smoking, ESR, CRP and the presence of IgM-RF and ACPA were included in the PLS as independent variables and the presence of MRI inflammation was included as untransformed dependent variable. Identified latent factors were plotted to explore whether there were distinguishable groups of patients which may represent patients with and without MRI inflammation.
The best cut-off point for clinically relevant MRI inflammation (associated with RA development) is not yet known and will be revealed by longitudinal studies. For this study we have used a cut-off score of ≥3 to dichotomise the group for the presence or absence of MRI-defined inflammation. In subanalyses a cut-off score of ≥4 for MRI inflammation was evaluated.
SPSS V.20.0 was used for analysis; p values<0.05 were considered significant.
Results
Clinical characteristics of patients with CSA
Between April 2012 and August 2013, 1558 patients presented to the rheumatology outpatient clinic of the Leiden University Medical Center with arthralgia. Of these, 102 (6.5%) were considered as being clinically suspect for progression to arthritis and included in the CSA cohort. The main reasons provided by rheumatologists to consider the arthralgia as clinically suspect were: joint pain that was worst in the early morning and improved with movement during the day; the presence of morning stiffness for ≥60 min; and a positive family history for RA. Table 1 presents the baseline characteristics of the included patients and figure 1 shows the location of their tender joints.
Patient and symptom characteristics (n=102)

Localisation of tender joints in the patients with clinically suspect arthralgia without clinical arthritis. DIPs, distal interphalangeal joints, IPs, interphalangeal joints; MCPs, metacarpophalangeal joints; MTPs, metatarsophalangeal joints; PIPs, proximal interphalangeal joints. Data presented are percentages of patients; since a patient can have several tender joints, the total exceeds 100%. The median (IQR) 68-tender joint count was 6 (3–11).
MRI characteristics of patients with CSA
MRI was performed in 93 patients. For the final analysis a combined inflammation score of ≥3 was used, but the components of all the MRI characteristics are shown in table 2 and in online supplementary table 1. Most individual lesions had a RAMRIS score of 1. Particularly for BME, bones with a score of 2 or 3 were rare. When evaluating the total scores for synovitis, BME and tenosynovitis separately, 52.7%, 51.6% and 35.5%, respectively, of the patients had a score of ≥1. Likewise, 20.4%, 9.7% and 10.8% had a score of ≥3 for the respective individual MRI features (table 2). When summing the scores of all three MRI features, 41 patients (44.1%) had a combined inflammation score of ≥3 and were considered as ‘MRI inflammation positive’.
Frequencies of MRI features in patients with clinically suspect arthralgia assessed using the rheumatoid arthritis MRI scoring system (RAMRIS) dichotomised at several cut-off points
Most inflammatory features were observed in the bones and joints of the wrist. Synovitis was most prevalent in the intercarpal, radiocarpal, MTP1 and MCP3 joints. BME occurred mainly in the capitate, lunate and MTP1. Tenosynovitis was most frequent in MCP3 (see online supplementary table 1 for a complete overview).
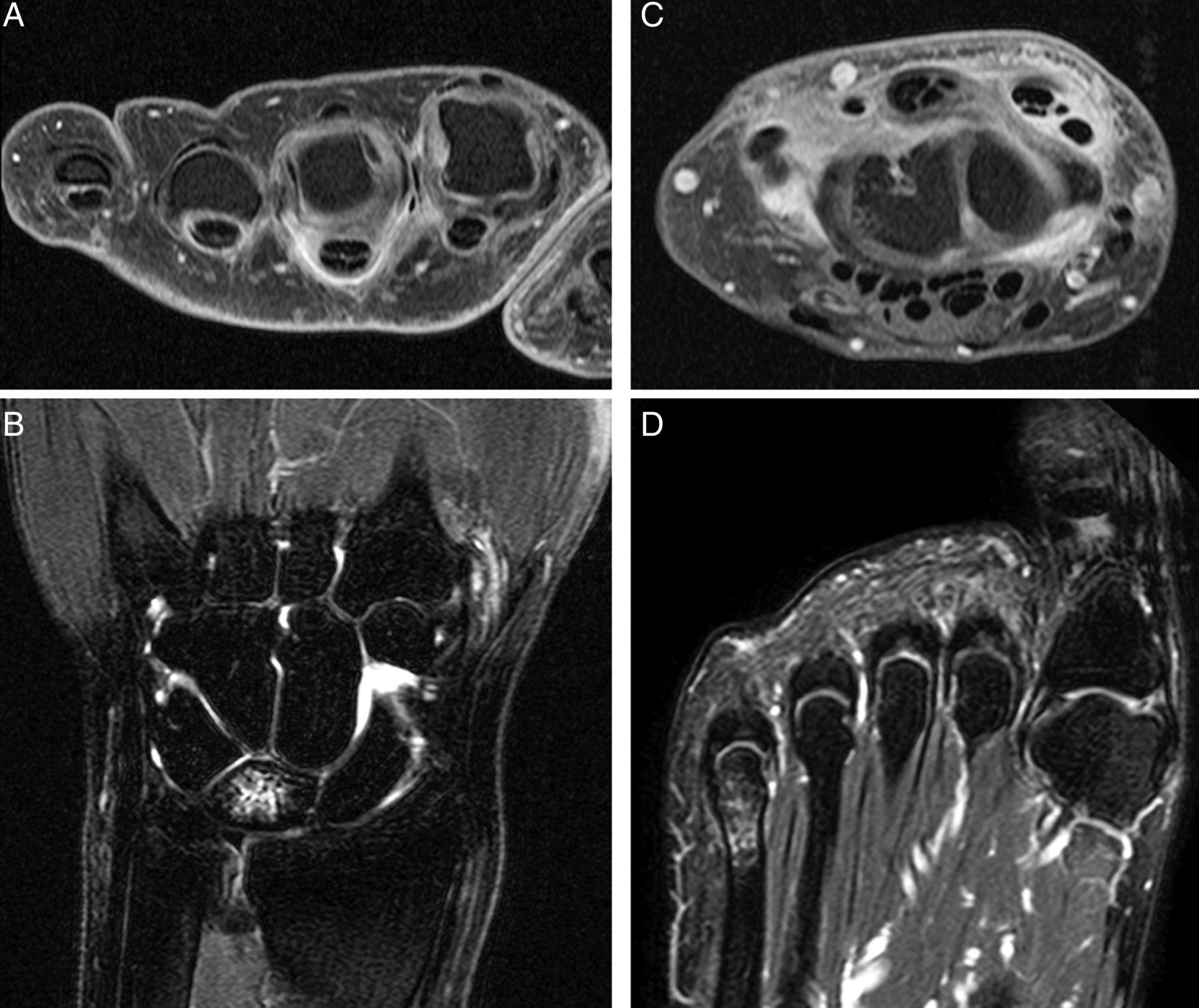
Figure 2 presents examples of patients with subclinical inflammation on MRI.

Subclinical inflammation shown on MRIs of (A) metacarpophalangeal (MCP) joints, (B, C) wrist and (D) metatarsophalangeal (MTP) joints of patients with clinically suspect arthralgia without clinically detectable arthritis. These images belong to four different patients. (A) Post-contrast axial T1-weighted FSE image with fat saturation of the MCP joints showing enhancement of the sheaths of the flexor tendons of MCP3 and MCP4, consistent with tenosynovitis. Synovitis is also present in the MCP2 and MCP3 joints. (B) Coronal T2-weighted FSE image with fat saturation of the wrist showing high signal intensity in the intercarpal joints (with enhancement on the post-contrast sequence, consistent with synovitis) and bone marrow edema (BME) in the lunate. (C) Post-contrast axial T1-weighted FSE image with fat saturation of the wrist showing intercarpal synovitis and tenosynovitis of the extensor compartments 2, 5 and 6. (D) Axial T2-weighted FSE image with fat saturation of the MTP joints with BME in the head of the fifth metatarsal bone. No synovitis is detected. Patient C developed clinically detectable arthritis in this wrist during follow-up.
Comparison of patient characteristics and subclinical MRI inflammation
Characteristics were compared between patients with (n=41) and without subclinical MRI inflammation using the predefined cut-off score of ≥3 (n=52) (table 3). Patients with MRI inflammation were significantly older (mean 50.4 years vs 37.9 years, p<0.001) and more frequently ACPA-positive (22.0% vs 7.7%, p=0.049). Patients with MRI inflammation also had a non-significant tendency to more frequently have a subacute symptom onset, symptom onset in both small and large joints and in the lower extremities, morning stiffness ≥60 min, a higher BMI, a lower 68-TJC and an increased ESR.
Clinical characteristics of patients with clinically suspect arthralgia without and with subclinical inflammation on MRI
Clustering of variables
Subsequently, to identify whether a combination of symptoms, signs and serological markers could distinguish the subsets of patients with and without subclinical MRI inflammation, a PLS analysis was performed with the presence of MRI inflammation as the outcome. Two latent factors were found that together explained 42.0% of the observed variance in MRI inflammation. The major important variables in these latent factors are presented in online supplementary table 2. The individual patients’ scores on these latent factors were plotted to see whether there were distinguishable groups representing patients with and without MRI inflammation. No clear distinguishable patient groups were observed, although a slight tendency to some clustering was noted (figure 3).

{kind=link}
{kind=link}
{kind=link}
Clustering of variables in patients with clinically suspect arthralgia related to inflammation on MRI. In this plot each dot indicates a single person. Latent factor scores indicate how strongly each factor is represented in each patient. A dot indicates how much the variance in an individual patient is being described by latent factor 1 on the x-axis in relation to latent factor 2 on the y-axis. Patients with a combined inflammation score of ≥3 are considered as having subclinical MRI inflammation and are represented by a circle, whereas patients with a combined inflammation score of <3 who are considered as having no MRI inflammation are represented by a triangle. No clearly distinguishable groups were observed, although a tendency to some clustering was observed to discern patients with and without MRI inflammation. Patients with MRI inflammation were older and more frequently had a subacute symptom onset, initial localisation in the large joints, initial localisation in the lower extremities and morning stiffness ≥60 min, a lower 68-tender joint count, a higher body mass index and more often had increased erythrocyte sedimentation rate and positivity for anti-citrullinated peptide antibodies and IgM rheumatoid factor compared with patients without MRI inflammation.
Subanalyses
MRI inflammation was defined as a combined inflammation score of ≥3. Because this cut-off is arbitrary, analyses were repeated with a cut-off score of ≥4. Patients with a combined inflammation score of ≥4 were significantly older (p<0.001), more often had morning stiffness ≥60 min (p=0.030), a lower 68-TJC (p=0.047) and more often had increased CRP (p=0.007) and ESR levels (p=0.003) than patients with a score of <4 (see online supplementary table 3). In PLS analysis, two latent factors were found that together explained 34.5% of the variance when MRI inflammation was defined as a combined inflammation score of ≥4. The patients’ scores of these two factors are shown in online supplementary figure 1. No clear clusters were observed.
Follow-up of MRI-defined inflammation
To date, 29 patients with MRI inflammation have been followed for at least 2 months. Although this follow-up duration is short, 10 of these patients (34.5%) developed arthritis. These patients had a median combined inflammation score of 4 (range 3–20). The patients were diagnosed with RA (n=8), unclassified arthritis (n=1) and psoriatic arthritis (n=1).
Discussion
In the present study we aimed to describe clinical and MRI characteristics of patients with CSA. We observed that subclinical MRI inflammation was present in 44% of all patients and that 35% of these patients with CSA had already progressed to clinical arthritis within at least 4 months of follow-up. The studied symptoms and characteristics could not clearly differentiate between patients with CSA with and without MRI inflammation.
Our approach was to select patients with arthralgia who were, according to the rheumatologist, suspected of progressing to arthritis over time. Since the symptomatic phase without arthritis in the pre-RA phase is not uniformly explicated and it is not known what type of arthralgia is specific for the pre-RA phase, we decided to depend on the ‘gut feeling’ (clinical expertise) of trained rheumatologists to select patients who were suspected as being in a preclinical phase of RA. Whether or not a patient had CSA was determined at the first visit before any blood tests had been performed, and thus did not depend on the knowledge of the autoantibody status of the patient. This concept is different from that used in studies on the preclinical phase that select persons with an increased risk of RA because of the presence of autoantibodies7 or a positive family history.27 The advantage of the current CSA approach is that it is in line with clinical practice where patients present with certain symptoms and the decision to perform additional investigations is based on the clinical presentation. Furthermore, it may allow identification of ACPA-negative RA in the preclinical phase.
The present study is the first large study to use dedicated MRI in patients at risk of RA. Our finding that subclinical inflammation as defined by MRI is present in 44% of patients with CSA is to some extent in line with the results of previous smaller studies. A previous MRI study among 22 patients with ACPA-positive arthralgia showed higher MRI inflammation scores in these patients compared with controls.20 Subclinical inflammation has also been visualised by positron emission tomography and ultrasonography.19 ,21
The joints and bones mostly affected by MRI-defined inflammation in our CSA cohort were locations where MRI inflammation is observed in patients with early arthritis patients (MCP3 joint, capitate and lunate, radiocarpal and intercarpal joints).22 This strengthens the indication that the inflammation observed in the patients with CSA in our study might be a precursor of clinical arthritis. The patients with CSA also frequently had inflammation in the MTP1 joint; this joint showed inflammation most frequently in the symptom-free controls (26%) and presumably inflammation here is not specific for RA.
Since MRI is a sensitive imaging technique, a relevant issue is which scores are normal and which reflect pathology. Several MRI studies on a small number of healthy volunteers showed MRI abnormalities to some extent.20 ,28 ,29 Due to different scoring methods and different readers used, the data are difficult to compare. An advantage of the present study is that it included MRIs of 19 symptom-free controls of comparable age and gender to the patients with CSA. Based on our impression that a score of 1 or 2 is rather minimal and that a score of ≥3 was observed in only 10% of controls, this cut-off was used to define the presence of MRI inflammation. Because we were aware that this cut-off is rather arbitrary and none of the controls had a score of ≥4, sensitivity analyses were done with a score of ≥4 as the definition of MRI inflammation. This showed similar results, although morning stiffness, TJC and the acute phase reactants were then also significantly associated with MRI inflammation. Ultimately, longer follow-up is needed to study the conversion to clinical arthritis. This will also reveal which cut-off of MRI-defined inflammation is associated with progression to clinical arthritis and RA.
This study has limitations. Because of time limitations we initially chose not to perform coronal sequences (perpendicular to the axis of the metatarsals) and post-contrast images of the MTP joints. Synovitis of the MTP joints was therefore initially assessed without contrast enhancement on axial sequences. Although previous studies have reported that eliminating contrast affected the as reliability of synovitis scoring compared with contrast-enhanced MRI, the sensitivity was reported to be high (78–90%) and the specificity moderate (31–79%).30 ,31 After 78 MRIs the scanning protocol was changed and coronal and post-contrast sequences of the foot were included, so synovitis in the MTP joints could be as reliably scored as in the wrist and MCP joints. As a consequence of the moderate specificity of non-contrast sequences, the synovitis scores of the MTP joints of the patients scanned by the first protocol might have been overestimated. On the other hand, due to lack of coronal sequences in the first protocol, the synovitis scores of the MTP joints might have been underestimated. However, synovitis of the MTP joints made a relatively small contribution to the total MRI inflammation score in the present data. A second limitation is the number of patients. Despite the infrastructural investments at our department to identify arthralgia patients early, the large majority of patients with arthralgia who presented at our outpatient clinic did not have CSA. Larger studies are needed to increase our understanding of the processes driving progression of subclinical inflammation in the pre-RA phases.
In the present study subclinical MRI inflammation was considered as proxy for RA-at-risk. Whether all patients with MRI inflammation will eventually develop arthritis is uncertain and unlikely. This will be studied during subsequent follow-up.
In conclusion, the preclinical phase of RA ‘symptoms without clinical arthritis’ was investigated by studying patients with CSA. Subclinical inflammation on MRI was observed in 44% of these patients. A combination of symptoms/characteristics incompletely differentiated patients with and without MRI inflammation. Follow-up will show which characteristics relate to the development of RA.
Acknowledgments
The authors would like to thank B Mertens from the department of Medical Statistics of the Leiden University Medical Center for his help with performing the partial least squares analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
Contributors HWvS, JABvN and AHMvdHvM made a substantial contribution to the acquisition, analysis and interpretation of the data. All authors made a substantial contribution to the conception and design of the work. HWvS and AHMvdHvM drafted the manuscript; JABvN, TWJH, JLB and MR revised the manuscript critically for important intellectual content. All authors approved the final version of the manuscript.
Funding The research leading to these results was funded by a Vidi-grant from the Netherlands Organisation for Scientific Research, the FP7 HEALTH program under the grant agreement FP7-HEALTH-F2-2012-305549, a grant from the Dutch Organisation of Health Research and Development, EuroTEAM, BTCURE and Masterswitch.
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was obtained from the medical ethics committee of the Leiden University Medical Center, Leiden, The Netherlands.
Provenance and peer review Not commissioned; externally peer reviewed.