Article Text

Abstract
Objectives To investigate the extent and performance of MRI lesions in the sacroiliac joint (MRI-SI) and spine (MRI-spine) in patients with suspected axial spondyloarthritis (axSpA).
Methods MRI-SI/spine of patients with chronic back pain (onset <45 years) in the SPondyloArthritis Caught Early (SPACE) cohort were scored by two well-trained readers for inflammation, fatty lesions, erosions, sclerosis/ankylosis and syndesmophytes. MRI performances were tested against the Assessment of Spondyloarthritis international Society (ASAS) axSpA criteria (positive: imaging-arm+ or clinical-arm+; negative: possible axSpA (few spondyloarthritis (SpA) features present) or no SpA). Arbitrary cut-off levels for MRI lesions were set to assure at least 95% specificity (tested in the no SpA group).
Results In total 126 patients were ASAS criteria positive (73 imaging-arm+ (22 by modified New York criteria (mNY)+; 51 by MRI+mNY−); 53 clinical-arm+) and 161 were ASAS criteria negative (89 possible axSpA and 72 no SpA). On MRI-SI (n=287), at least three fatty lesions (or at least three erosions) were seen in 45.5 (63.6)% of mNY+ patients, 15.7 (47.1)% of MRI+mNY− patients and 15.1 (13.2)% of clinical-arm+ patients versus 3.4 (6.7)% of possible axSpA patients and 2.8 (4.2)% of no SpA patients. A combined rule (at least five fatty lesions and/or erosions) performed equally well. Sclerosis and ankylosis were too rare to analyse. On MRI-spine (n=284), at least five inflammatory lesions (or at least five fatty lesions) were seen in 27.3 (18.2)% of mNY+ patients, 13.7 (21.6)% of MRI+mNY− patients and 3.8 (1.9)% of clinical-arm+ patients versus 4.5 (6.7)% of possible SpA patients and 2.9 (4.3)% of no SpA patients.
Conclusions The presence of (1) at least five fatty lesions and/or erosions on MRI-SI, (2) at least five inflammatory lesions or (3) at least five fatty lesions on MRI-spine allows an acceptable discrimination of axSpA and no SpA, while assuring >95% specificity.
Statistics from Altmetric.com
Introduction
Conventional radiographs of sacroiliac joints (SIJ) are frequently used for detecting sacroiliitis and diagnosing axial spondyloarthritis (axSpA). Limitations to this method are the major inter-reader variability and, as it takes time to develop structural damage visible on radiographs, the delay in diagnosis of several years.1–5 A good addition to using radiographs is MRI, since MRI can visualise both inflammatory lesions and structural damage while radiographs only depict structural damage.4 Hence the increasing interest in MRI in the field of axSpA. MRI has a major role as entry criteria imbedded in the imaging arm of the Assessment of Spondyloarthritis international Society (ASAS) classification criteria for axSpA.6 Patients fulfilling the imaging arm have sacroiliitis on conventional radiographs and/or MRI plus ≥1 additional spondyloarthritis (SpA) feature.6 Radiographic sacroiliitis is defined as described in the modified New York (mNY) criteria.7 Sacroiliitis on MRI is defined according to the ASAS definition of a positive MRI of the SIJ (MRI-SI).8 Experts in the field created this definition in 2009, which is based on inflammatory lesions only. The question if structural lesions should be added to this definition is still outstanding. Trying to address this question, a study found that erosions are relatively specific for SpA and may increase the utility of MRI. They proposed an adjusted version of the ASAS definition of a positive MRI-SI adding the presence of erosions.9 Another question that emerged was whether the inclusion of spinal lesions could contribute to detecting axSpA. In 2012, the same group of experts that created the definition of a positive MRI-SI, proposed a definition for a positive MRI of the spine (MRI-spine).10 The realisation of this definition was based on a systematic literature review; however, before its existence the Canada–Denmark MRI working group also described spinal lesions typical for SpA. Comparing these studies demonstrates the similarity of descriptions used by both working groups.10–12
There were two objectives in this study. First, to investigate the quantity of structural MRI-SI lesions and inflammatory and structural MRI-spine lesions in patients with axSpA and patients with relatively short duration chronic back pain (CBP) due to other causes. Elaborating on this, the second objective was to investigate which lesions, and to what extent, assure sufficient specificity for axSpA.
Methods
Patients of ≥16 years with CBP (≥3 months, ≤2 years, onset <45 years, cause unknown) were included in the SPondyloArthritis Caught Early (SPACE) cohort from five participating centres in the Netherlands (Leiden, Amsterdam and Gouda), Norway (Oslo) and Italy (Padova). To classify patients according to the ASAS criteria, presence of SpA features was examined according to a fixed protocol including physical examination, laboratory tests, plain radiographs and MRI-SI/spine. The SpA features are radiographic sacroiliitis (mNY criteria: bilateral grade ≥2 or unilateral grade ≥3),7 sacroiliitis on MRI (presence of ≥2 inflammatory lesions highly suggestive of axSpA on a single slice or one lesion on ≥2 consecutive slices),8 HLA-B27 positivity, positive family history for SpA, inflammatory back pain (IBP), psoriasis, peripheral arthritis, dactylitis, heel enthesitis, uveitis, inflammatory bowel disease (IBD), good response to non-steroidal anti-inflammatory drugs (NSAIDs) and elevated C-reactive protein (CRP) or erythrocyte sedimentation rate (ESR).6
Baseline data were used in the analyses. A detailed description of the recruitment and clinical assessment of the SPACE cohort has been published before.13
MRI assessment
Patients underwent an MRI-SI and MRI-spine performed on a 1.5T scanner. The acquired sequences for both modalities were Short Tau Inversion Recovery (TR2500/TE600) and T1-weighted Turbo Spin-Echo (TR550/TE10), with a slice thickness of 4 mm. The MRI-SI images were performed in coronal oblique plane and MRI-spine in sagittal plane.14 Two well-trained readers (RvdB and MdH) independently scored all MRIs with both sequences viewed simultaneously, while blinded for all clinical data. MRI-SI was scored separately from MRI-spine. In some cases adjudication scores were obtained (see below).
MRI-SI lesions
Weber et al adapted the Spondyloarthritis Research Consortium of Canada (SPARCC) scoring system for inflammation in the SIJ to quantify fatty lesions, erosions, sclerosis and ankylosis in the SIJ.9 In the current study this adapted SPARCC scoring system was used and structural lesions on ≥2 consecutive slices were scored, resulting in a maximum score of 40 per lesion (5 lesions per quadrant over all slices×4 quadrants×2 SIJ). Note that ankylosis always involves two quadrants (either upper iliac and upper sacral or lower iliac and lower sacral quadrants). In addition, readers gave a general dichotomous verdict (yes/no) on a ‘positive MRI-SI’ (ASAS definition).8
An adjudicator (VNC) was introduced when readers disagreed on a ‘positive MRI-SI’ or the presence/absence of erosions according to a specific definition (≥2 erosions on the same slice or one erosion seen on ≥2 consecutive slices).9 We offered images that needed adjudication and images on which initial readers agreed to keep the adjudicator blinded. In the analyses, mean scores of the two readers agreeing on a ‘positive MRI-SI’ were used for quantifying MRI-SI lesions.
MRI-spine lesions
Spinal MRI lesions were scored according to the Canada–Denmark score in which every vertebral unit (VU) is divided into quadrants. Per quadrant dichotomous scores (presence/absence) on corner inflammatory and structural lesions (fatty lesions, erosions, syndesmophytes) are given.11 ,12 Inflammatory and fatty lesions were scored when present on ≥2 consecutive slices. Erosions and syndesmophytes were scored when visible on ≥1 slice. Spinal lesions were only scored when considered typical for axSpA and not due to other causes like degenerative changes. Both readers also gave a general dichotomous verdict (yes/no) on a ‘positive MRI-spine’ (ASAS definition: ≥3 corner inflammatory lesions).10 An adjudicator (VNC) was introduced when inter-reader disagreement on a ‘positive MRI-spine’ (ASAS definition) or presence/absence of ≥3 fatty lesions was found.
The lesions of all quadrants throughout the 23 VUs were added up and the mean scores of the two readers agreeing on ‘positive MRI-spine’ were used to quantify spinal lesions for analyses.
Classification
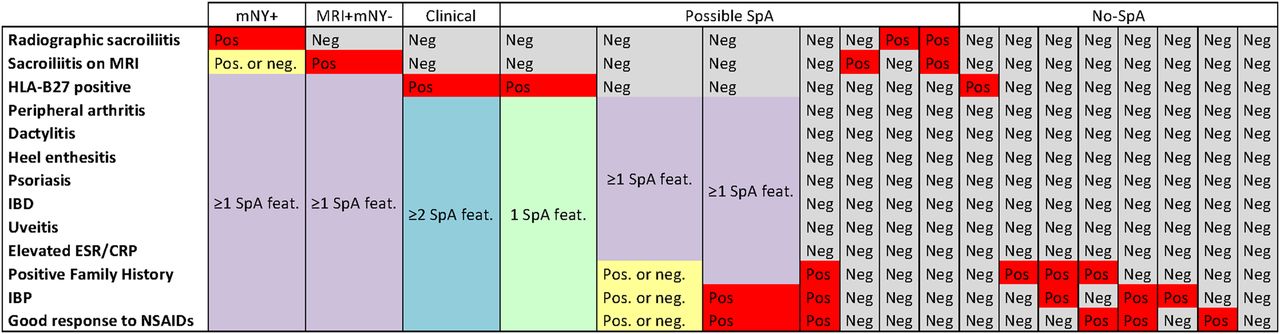
All patients were classified according to the ASAS criteria for axSpA.6 Patients with axSpA were divided into subgroups; the imaging arm contained patients fulfilling the mNY criteria (mNY+) and patients not fulfilling the mNY criteria but with a ‘positive MRI-SI’ (MRI+mNY−) and ≥1 SpA feature. HLA-B27-positive patients with ≥2 additional SpA features and mNY− and MRI-SI− were grouped (clinical arm). There were also patients not fulfilling the ASAS criteria but with a suspicion of axSpA because of the presence of SpA features with a high likelihood (eg, dactylitis) or three less specific (IBP, positive family history for SpA and good response to NSAIDs) SpA features (possible axSpA).15 The final group consists of patients in whom the possibility of having SpA at baseline was very low since patients did not have sacroiliitis on imaging, were HLA-B27 negative or had ≤2 SpA features with a low likelihood for SpA (no SpA). For a complete and detailed description on how patients were classified see figure 1.

{kind=link}
Grouping of the patients. The first row depicts the different groups and the first column depicts all SpA features (starting with the major elements of the ASAS criteria (imaging and HLA-B27)). The other columns represent the various classification groups. Each patient can belong only to one of these subgroups. Per column, all conditions mentioned in the cells must be met. Some individual SpA features are mandatory: the red cells indicate all individual features that must be present and the grey cells indicate all individual features that must be absent. In addition, in some subgroups there are individual SpA features that have no impact on the classification (indicated as yellow). Finally, there are groups of SpA features for which exactly one SpA feature needs to be positive (green), ≥1 SpA feature needs to be positive (purple) or ≥2 SpA features need to be positive (blue). ASAS, Assessment of Spondyloarthritis international Society; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; feat., feature; HLA, human leucocyte antigen; IBD, inflammatory bowel disease; mNY, modified New York criteria; Neg, negative; NSAIDs, non-steroidal anti-inflammatory drugs; Pos, positive; SpA, spondyloarthritis.
To detect the influence of age we compared the extent of MRI lesions in patients with an age at onset of CBP <35 years and between 35 and 45 years.
Data analysis
The proportion of patients with lesions was presented using several cut-offs. Lesions in the no SpA group were considered ‘false positive’. Arbitrarily, we defined the lowest cut-offs with ≤5% false positives, reported in bold and italic, as the optimal cut-off to ensure high specificity. In addition, the lowest cut-offs with ≤10% false positives were reported in italic. Besides single MRI lesions, also combinations of lesions were tested in order to find the number and type of lesions most specific for axSpA. All analyses were performed in SPSS V.22.0.
Results
Baseline MRI-SI and clinical data were available in 287 patients, of which 103 (35.9%) are men. There were 126 patients (43.9%) fulfilling the ASAS criteria, 89 possible axSpA patients (31.0%) and 72 no SpA patients (25.1%). Of the no SpA patients, 21 had IBP only, 12 had both IBP and a good response to NSAIDs, 7 had a good response to NSAIDs, 5 had a positive family history and 2 patients were HLA-B27 positive, all in the absence of other SpA features. There were 18 patients without SpA features. Five possible axSpA patients had sacroiliitis on X-ray (n=1) or MRI (n=4) in the absence of other SpA features and therefore did not fulfil the ASAS criteria (table 1).
Characteristics of patients with axSpA and chronic back pain due to unknown causes
MRI-SI lesions
In 72 cases adjudication was needed due to disagreement on a positive MRI-SI (kappa primary readers=0.75) or the presence of erosions (kappa primary readers=0.57).
Table 2 shows the proportion of patients with single MRI-SI lesions. Fatty lesions and erosions were seen in all subgroups of patients, but more frequently in patients fulfilling the imaging arm (mNY+ and MRI+mNY−), and only somewhat more frequent in patients in the clinical arm compared with the possible axSpA and no SpA groups. Cut-off ‘≥3 fatty lesions’ and cut-off ‘≥3 erosions’ corresponded to ≤5% false positives. Applying these cut-offs differentiated well between patients fulfilling the imaging arm, especially mNY+ patients, and no SpA patients. The proportion of patients with ‘≥3 fatty lesions’ and ‘≥3 erosions’ in the clinical arm and possible axSpA group is relatively low, ranging from 3.4% to 15.1%. Sclerosis and ankylosis were rarely seen (table 2).
Proportions of patients with single or combined lesions seen on MRI of the SIJ
Several combinations between structural lesions were investigated to see if this would increase specificity. Since sclerosis and ankylosis as single lesions occurred rarely, and were not specific, combinations containing these lesions were not shown, as these did not change the results. When looking at ‘fatty lesions and/or erosions’ cut-off ≥5 yielded ≤5% false positives, while the proportion of patients in the MRI+mNY− (37.3%) and mNY+ (63.6%) groups remain reasonably high (see table 2).
MRI-spine lesions
In 284 of 287 patients MRI-spine was available. Disagreement between readers resulted in adjudication in 43 patients. The reliability for the primary readers was good to moderate (kappa 0.73 for inflammatory lesions and 0.60 for fatty lesions).
More than half of the patients in the imaging arm had spinal inflammatory lesions (cut-off ≥1), but this was also the case in 36.3% of the no SpA patients. With ≥5 inflammatory lesions the proportion of false positives decreased ≤5% with still a relatively high proportion of patients with inflammatory lesions in MRI+mNY− (13.7%) and especially in the mNY+ group (27.3%) (table 3). Fatty lesions (cut-off ≥1) were the most often seen spinal structural lesions (range 24.5%–50.0%). Cut-off ≥5 corresponds to ≤5% false positives, while the proportion of patients in the mNY+ and MRI+mNY− groups were 18.2% and 21.6%, respectively.
Proportions of patients with lesions seen on MRI of the spine
Between 22.7% and 33.3% of patients across all groups had ≥1 erosion. Increasing the cut-off decreased the proportion of false positives from 14.5% (cut-off ≥2) to 7.2% (cut-off ≥3) to 2.9% (cut-off ≥4). However, the proportion of patients in the imaging arm was nearly as low, decreasing from 18.2% to 13.6% to 4.5% (mNY+) and 15.7% to 7.8% to 3.9% (MRI+mNY−) with cut-off ≥2, ≥3 and ≥4, respectively, showing that spinal erosions are not suitable to discriminate between subgroups. This applies also to syndesmophytes, as similar proportions of patients with syndesmophytes were shown in all subgroups irrespective of the cut-off (table 3).
Specificity did not increase when combining inflammatory and structural lesions. Even when combining the two most specific spinal lesions (‘inflammatory and/or fatty lesions’), specificity did not increase and the proportion of false positives only drop below ≤5% with cut-off ≥8 (data not shown).
Effect of age
In order to further investigate the specificity of lesions we stratified patients by age at onset of CBP: onset of CBP <35 years (younger age group) or onset of CPB between 35 and 45 years (older age group). On MRI-SI there was no effect of age for any single lesion, nor for any combinations (data not shown). However, on MRI-spine, the number of inflammatory lesions corresponding to ≤5% false positives was far lower in the younger (≥3) compared with the older (≥6) age group (table 4). Furthermore, with this lower cut-off in the younger age group the proportion of patients in the imaging subgroups was still high, while with the higher cut-off in the older age group the proportion of patients was comparable throughout all subgroups. Similarly, fatty lesions (cut-off ≥3) were only specific for axSpA in the younger age group. For erosions and syndesmophytes the specificity was poor in both age groups (table 4).
Proportions of patients with lesions seen on MRI of the spine, stratified by age
Discussion
In patients with CBP included in the SPACE cohort we investigated the extent of structural lesions on MRI-SI, as well as inflammatory and structural lesions on MRI-spine. We found the rules ‘≥5 fatty lesions and/or erosions’ on MRI-SI, as well as ‘≥5 spinal inflammatory lesions’ and ‘≥5 spinal fatty lesions’ to be highly specific for axSpA, while still assuring an acceptable and useful level of discrimination between axSpA patients and no SpA patients. Similar results were found for single MRI-SI lesions: optimal cut-offs were ‘≥3 fatty lesions’ and ‘≥3 erosions’.
Erosions on MRI-SI are considered specific for axSpA. Studies have shown that erosions, either in the presence or in the absence of inflammation, are seen in both patients with early axSpA and ankylosing spondylitis (AS). These studies have purported that structural lesions, especially erosions, greatly contribute to the diagnostic value of MRI-SI.16 ,17 But there are limited data about the extent of MRI-SI lesions. Althoff et al and Krohn et al reported 2.4–7.6 fatty lesions and 3.8–8.2 erosions in patients with axSpA (nr-axSpA and AS).18 ,19 The extent of these lesions seem to correspond to the cut-offs we find to be specific for axSpA in our study. Unfortunately, due to the absence of a control group in these studies it is impossible to confirm the specificity using our cut-offs in their studies. But Weber et al included patients with axSpA as well as patients with non-specific back pain and healthy controls when defining optimal cut-offs for MRI-SI. They reported data from two cohorts and found that ≥1 erosion (both cohorts) and ‘≥12/≥9 fatty lesions’ (cohort A/B) yielded a specificity of ≥90.0%. When looking at lesion combinations they found ‘≥12/≥11 fatty lesions and/or erosions’ (cohort A/B) to be most specific for axSpA.20 There is a difference in study design compared with our study. Weber et al classified patients based on the clinical opinion of a rheumatologist with access to the patient's clinical data and pelvic radiographs. We have classified patients according to the ASAS criteria. By doing so, we deliberately not interpreted the MRI features under study. Previously, we have shown that there is high agreement between the rheumatologist's diagnosis and fulfilment of the ASAS criteria in the SPACE cohort.13 It might be a reasonable approach to consider fatty lesions in conjunction with erosions rather than each separately: one study has shown that fatty lesions alone only contribute marginally to recognising patients with axSpA, while the majority of the patients with axSpA have fatty lesions alongside inflammation or erosions.21 Summarising the literature, evidence is found that erosions have more diagnostic value than fatty lesions (alone). In keeping with our findings, a useful next step in determining the diagnostic utility of MRI-SI could be to test if adding ‘≥3 fatty lesions’ as a criterion to the ASAS definition of a positive MRI-SI would increase the diagnostic performance. Similar analyses could be conducted with criteria such as ‘≥3 erosions’ and the combination of ‘≥5 fatty lesions and/or erosions’.
The validation of our findings in independent cohorts could provide insight into the dilemma if and which structural lesions should be added to the ASAS definition of a positive MRI. Another relevant question is if MRI somehow could replace the role of plain pelvic X-rays in the determination of a positive imaging result.
In our study we have shown that reasonable and applicable cut-offs can be defined for inflammatory and fatty lesions on MRI-spine when specificity (>95%) for axSpA is the main aim. However, there are some conflicting data in the literature. A recent study states that adding spinal inflammatory and fatty lesions, in the classification of patients with axSpA, does not help since a better classification of patients with nr-axSpA is offset by increased misclassification of controls.22 However, with a suitable cut-off value the number of false positives could be reduced. In our analyses, only ‘≥5 inflammatory lesions’ and ‘≥5 fatty lesions’ are having >95% specificity. This cut-off of ‘≥5 inflammatory lesions’ is higher than the proposed ASAS definition of a positive MRI-spine (≥3), but Weber et al report an even higher cut-off (≥6 inflammatory lesions) corresponding to moderate to substantial diagnostic utility in patients with axSpA, while their cut-off of ≥6 fatty lesions only resulted in moderate specificity (82%/81% for two cohorts). In addition, like us, they found that combining spinal inflammatory and fatty lesions does not increase specificity.23 Also, Bennett et al found that >5 fatty lesions had diagnostic utility for axSpA.24 Comparing our data with the literature, even with different readers, different cohorts and different choices of external standard, we have arrived at approximately similar cut-offs for inflammatory and fatty spinal lesions (≥5 for both) with proven preservation of high specificity.
When the ASAS criteria were developed, MRI-spine was not included because the specificity of spinal lesions was argued.6 The aforementioned study by Weber et al22 reported that combining MRI-spine and MRI-SI added little diagnostic value compared with MRI-SI alone. Testing our proposed cut-offs in independent cohorts could provide further insight in this matter.
The major limitation in studies testing the diagnostic value of imaging in axSpA is the lack of a ‘gold standard’. In this study, patients were classified according to the ASAS criteria. Since we have investigated lesions not (yet) included in the ASAS criteria, circular reasoning is likely irrelevant here. An alternative external standard could be the diagnosis by the rheumatologist. However, physicians use similar clinical data to base their opinion on and may have had access to imaging data that could influence their opinion about the presence/absence of axSpA. A definite strength of this study is the availability of a no SpA control group that allows the determination of true specificity. Having multiple readers involved in the image scoring and this being a multicentre cohort study markedly added to the credibility of the final judgement about the presence or absence of structural lesions and the generalisability to other independent cohorts.
In conclusion, the presence of (1) at least five fatty lesions and/or erosions on MRI-SI, (2) at least five inflammatory lesions or (3) at least five fatty lesions on MRI-spine, allows an acceptable discrimination of axSpA and no SpA, while assuring >95% specificity.
References
Footnotes
Handling editor Hans WJ Bijlsma
Contributors MdH performed the statistical analyses and writing of the manuscript. DvdH gave methodological advice and supervised all procedures. All authors contributed to the acquisition and interpretation of data, read, revised and approved the final manuscript.
Funding The study has been funded by the Dutch Rheumatism Association (Reumafonds).
Competing interests None declared.
Ethics approval Local Medical Ethical Committee of the centres involved.
Provenance and peer review Not commissioned; externally peer reviewed.