Article Text

Abstract
Objective To compare the clinical outcomes at 1 year after the treatment with either abatacept or tocilizumab in patients with rheumatoid arthritis in routine clinical practice.
Methods To overcome potential bias in allocation to treatment with abatacept or tocilizumab, a propensity score based on multiple baseline characteristics variables was calculated and 102 of 194 patients treated with abatacept and 102 of 273 patients treated with tocilizumab were statistically extracted. Clinical outcomes were assessed.
Results The baseline characteristics were statistically comparable. At week 52, 72%/69% of patients (abatacept/tocilizumab) were still receiving treatment. The Simplified Disease Activity Index (SDAI) decreased from 28.7/27.7 at baseline to 14.0/12.5 at week 52 with abatacept/tocilizumab, respectively. At week 52, the remission rates for abatacept/tocilizumab were 18%/20%, respectively. No statistical difference in clinical efficacy between abatacept and tocilizumab was seen. Moreover, a subanalysis showed that abatacept and tocilizumab had similar effectiveness with or without methotrexate. However, prognostic factors at baseline contributing to the Clinical Disease Activity Index at week 52 were different between the two groups by multiple regression analysis. A higher rheumatoid factor (RF) titre and lower SDAI at baseline were associated with lower SDAI at week 52 in patients treated with abatacept, whereas patients receiving tocilizumab with a lower Health Assessment Questionnaire Disability Index and who were biologics-naïve at baseline had a lower SDAI at week 52.
Conclusions We compared patients treated with abatacept or tocilizumab after statistical adjustment by propensity score matching. Clinical efficacies, including SDAI, were comparable in both treatment groups. However, the predictive factors were different: abatacept appears to benefit patients with higher RF titres, and early induction of tocilizumab is an important factor for good clinical efficacy.
- Rheumatoid Arthritis
- DMARDs (biologic)
- Outcomes research
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA) is an autoimmune disease characterised by synovitis. With the development of tumour necrosis factor (TNF) inhibitors, clinical remission has become a primary goal in the treatment of the disease.1 In addition to TNF inhibitors, tocilizumab, which targets interleukin (IL)-6, and abatacept, which targets T cells, have recently been introduced. Based on the results of clinical trials, abatacept and tocilizumab are regarded as standard treatments together with TNF inhibitors in patients with RA whose disease is refractory to methotrexate (MTX).2–9 Current research focuses on how to use these biological products.10 To date, no randomised controlled trials (RCTs) comparing the efficacies of abatacept and tocilizumab have been conducted.
RCTs are regarded as a reliable means of obtaining evidence on the efficacy and safety of drugs. However, there are limitations to RCTs.11 The most important limitation is that the study subjects are selected using inclusion and exclusion criteria. In most cases, older and young individuals and those with liver and/or renal disease are excluded. This limits the applicability to clinical practice of the results on the efficacy and safety of drugs. On the other hand, observational studies typically involve patients who are commonly encountered in daily clinical practice; however, study participants are subject to selection bias due to the uncontrolled differences between the treatment and control groups. Therefore, a precise comparison of drugs is difficult in observational studies.
In recent years, propensity score matching has become a popular method of reducing the limitations of observational studies, such as selection bias, by adjusting for potential confounding factors. Studies using propensity scores have been considered as reliable and able to produce evidence comparable to RCTs by reducing selection bias. Propensity score matching does, however, require a certain number of subjects because matched patients have to be extracted from a primary study population.12–14
The subjects of our study comprised 194 patients treated with abatacept and 273 with tocilizumab. Of these patients, 102 from each group were matched based on the estimated propensity scores. The objective of this study was to determine the predictive factors of the efficacy of abatacept and tocilizumab and to provide evidence to guide drug selection by comparing the clinical efficacy of the two drugs.
Patients and methods
Patients
All patients who started treatment with abatacept or tocilizumab between May 2008 and December 2013 at our hospital were registered in the study. All patients had a diagnosis of RA defined using the American Rheumatism Association 1987 revised criteria or the 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) classification criteria.15–17 The study was approved by the ethics review board of the University of Occupational and Environmental Health, Japan and was conducted as a retrospective observation study.
Abatacept and tocilizumab treatment
Abatacept and tocilizumab were prescribed to patients with RA uncontrolled by normal doses of existing disease-modifying antirheumatic drugs. Abatacept was given as an intravenous infusion (500 mg for patients of <60 kg, 750 mg for 60–100 kg and 1000 mg for >100 kg) at weeks 0, 2 and 4, and then every 4 weeks thereafter. Tocilizumab was administered intravenously (8 mg/kg) every 4 weeks.
Clinical efficacy
Disease activity was assessed using the 28-joint count disease activity score-erythrocyte sedimentation rate (DAS28-ESR)18 and the Simplified Disease Activity Index (SDAI).19 ,20 Functional impairment was assessed using Health Assessment Questionnaire Disability Index (HAQ-DI).21
Propensity score matching
In contrast to RCTs, it is difficult to compare the efficacy in an observational study because of the treatment-selection bias. To overcome this problem, we used propensity score matching.22 The propensity score matching method was proposed to evaluate statistically causal effects free from confounding effects, by mathematically refashioning an observational study into a randomised study. In this study, the propensity score was estimated using a multivariable logistic regression model predicting the use of abatacept using the following key variables: age, sex, disease duration, prior treatment with biological agents, MTX use, oral steroid use, SDAI, tender joint count (TJC), swollen joint count (SJC), patient’s global assessment (PGA), physician’s (evaluator) global assessment (EGA), DAS28-ESR, rheumatoid factor (RF), matrix metalloproteinase 3 (MMP-3), ESR, C-reactive protein (CRP) and HAQ-DI. After confirming that the accuracy of this model was good (the area under the receiver operating characteristic curve was 0.81; online supplementary figure S1), we then matched 102 patients in each group based on the propensity score.
Statistical analysis
A paired t test was used to detect statistically significant differences between baseline and week 52 in each group. Comparisons of the matched cohorts were performed using McNemar's test. The Kaplan–Meier method was used to assess the retention rates and the differences were analysed by the log-rank test. To identify prognostic factors, a full model with age, sex, disease duration, prior use of biological agents, MTX use, CRP, RF, MMP-3, SDAI and HAQ-DI was fitted. All reported p values were two-sided and were not adjusted for multiple testing.23 ,24 The level of significance was taken as p<0.05. The last observation carried forward method was used for patients who discontinued treatment before week 52 to include all patients in analysis. All analyses were conducted using JMP V.11.0 (SAS Institute Inc, Cary, North Carolina, USA).
Results
Patients disposition and baseline characteristics
All patients who started treatment with abatacept (n=194) or tocilizumab (n=273) between 2008 and 2013 were enrolled. To avoid treatment-selection bias, propensity score matching was performed (see online supplementary figure S2), resulting in 102 matched pairs of patients who treated with abatacept or tocilizumab (see online supplementary table S1).
The patients’ characteristics are shown in table 1. Mean age was 60.7 years for abatacept and 59.2 years for tocilizumab, and most patients were woman (85.3% for abatacept and 83.3% for tocilizumab). Mean duration of illness was 8.7 years for abatacept and 9.5 years for tocilizumab.
Baseline characteristics of patients
Mean disease activity at baseline was 28.7 and 5.7 for SDAI and DAS28-ESR in the abatacept group and 27.7 and 5.6 for SDAI and DAS28-ESR in tocilizumab group, respectively. Mean HAQ-DI scores were 1.5 in both groups. Around half the patients had been treated with at least one biological agent (54.9%/59.8%).
Concomitant MTX at baseline was given to 66.7% in the abatacept group and 64.7% in the tocilizumab group at mean doses of 11.2 mg/week and 11.9 mg/week, while 34.3% and 37.3% were treated with concomitant oral steroids at mean doses of 4.9 mg/day and 4.9 mg/day (prednisolone equivalent), respectively.
Other laboratory findings included mean RF, MMP-3, ESR and CRP levels of 166.3/176.6 U/mL, 236.0/205.6 ng/mL, 53.3/51.3 mm/h and 2.1/2.0 mg/dL, respectively.
These baseline characteristics of the two groups were statistically comparable (table 1).
Drug survival and adverse events
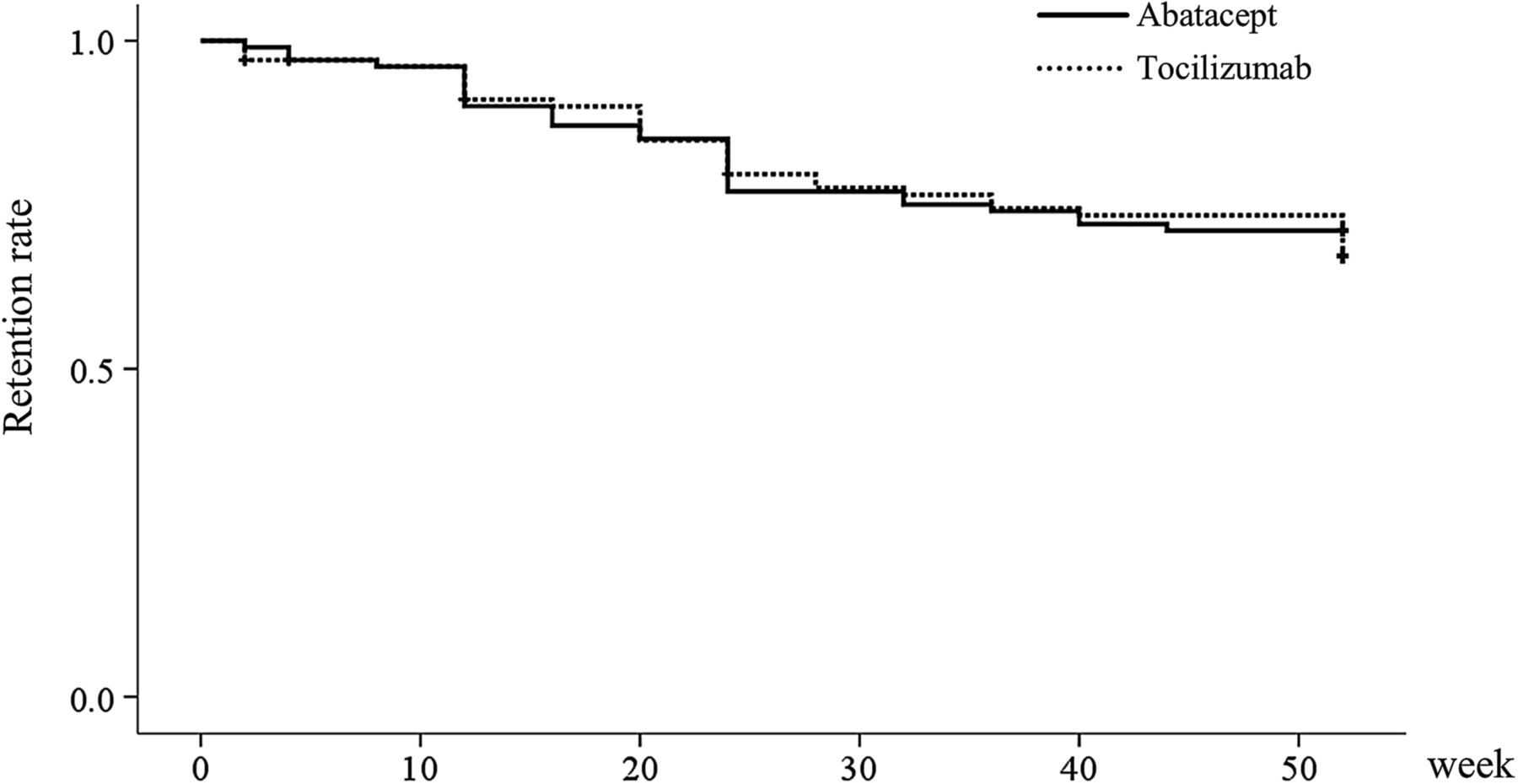
The retention rates are shown in figure 1. At week 52, 71.6% of patients were still receiving abatacept and 68.6% of patients were still receiving tocilizumab. The retention rates were not significantly different (p=0.64). In addition, the prevalence of comorbidities, which may affect the retention rate, such as diabetes and the presence of coexisting pulmonary disease, were also not different.

Retention rate of abatacept and tocilizumab treatment over 52 weeks (Kaplan–Meier plots).
The most common reason for discontinuation of abatacept was inadequate effect (22.5%); four patients (3.9%) discontinued treatment because of an adverse event (see online supplementary table S2). On the other hand, among those who discontinued tocilizumab, inadequate effect was reported by 17 patients (16.7%) and an adverse event was reported by six patients (5.9%). Notably, no patients in the abatacept group withdrew because of infection, whereas three patients (2.9%) withdrew because of infection in the tocilizumab group. Other adverse events that led to discontinuation were stomatitis in the abatacept group and liver dysfunction in the tocilizumab group (see online supplementary table S2).
Clinical efficacy
The changes of SDAI recorded over 52 weeks are in shown in figure 2A. The SDAI for patients receiving abatacept significantly improved from 28.7 at baseline to 14.0 at week 52. Changes in disease activity in patients stratified by SDAI (remission, SDAI <3.3; low, SDAI >3.3 to <11.0; moderate, SDAI >11.0 to <26.0; high, SDAI >26.0) are shown in figure 2A. SDAI remission rate was 18% at week 52 of patients who treated with abatacept. Overall, 47% of patients achieved either remission or a low disease activity at the end of the study.
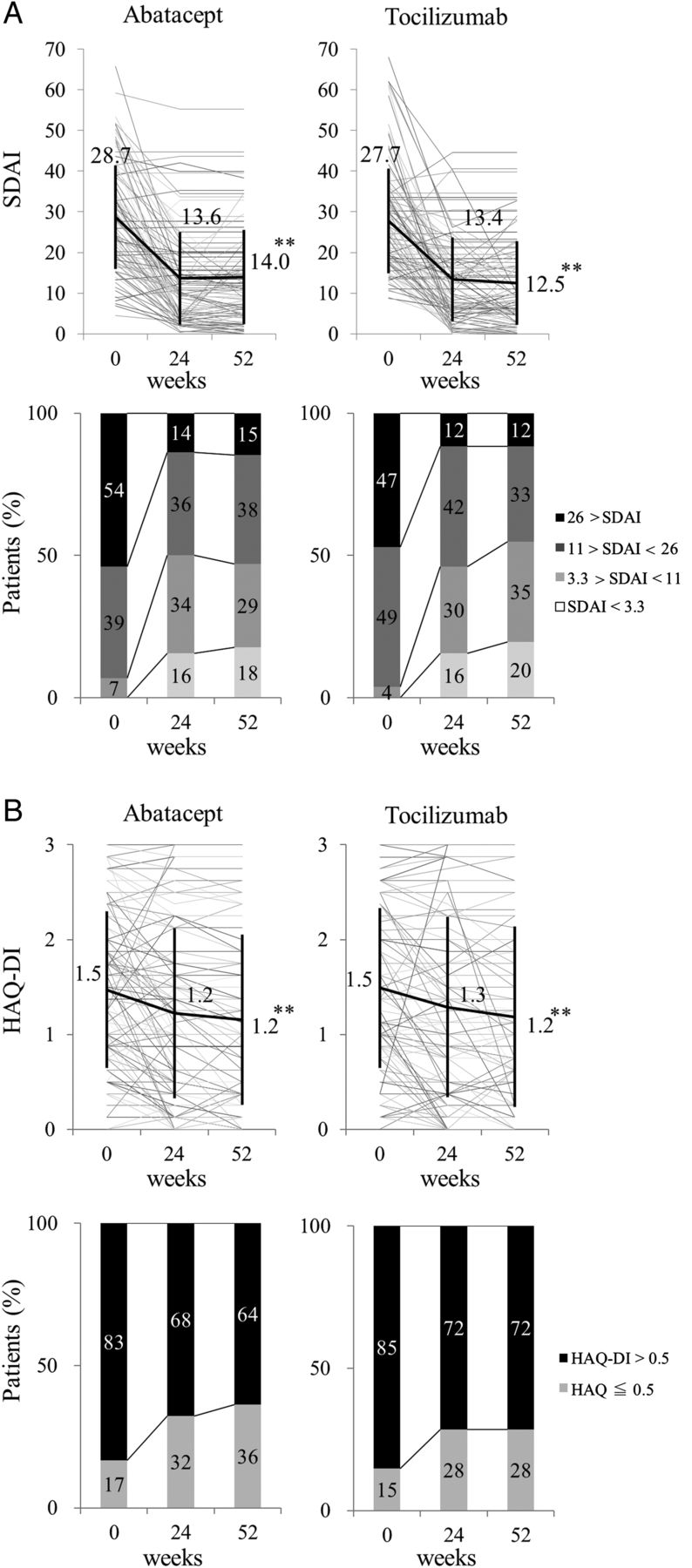
Effects of treatment with abatacept and tocilizumab for 52 weeks on clinical outcomes. (A) Time course of the Simplified Disease Activity Index (SDAI) and disease activity stratified according to SDAI; (B) time course of the Health Assessment Questionnaire Disability Index (HAQ-DI) and proportion of patients with HAQ-DI ≤0.5. **p<0.001.
Patients receiving tocilizumab also showed a significantly improved SDAI from 27.7 at baseline to 12.5 at week 52 (figure 2A). Changes in disease activity in patients stratified by SDAI are shown in figure 2A. SDAI remission rate was 20% at week 52 of patients who treated with tocilizumab. Overall, 55% of patients achieved either remission or a low disease activity at the end of the study.
The proportions of patients achieving remission or a low disease activity stratified by SDAI were also similar (p=0.72, 0.27, respectively) at week 52. These results suggest that abatacept and tocilizumab had similar clinical efficacy in routine care.
Health Assessment Questionnaire Disability Index
The mean HAQ-DI improve significantly from 1.5 to 1.2 at week 52 and from 1.5 to 1.2 at week 52 in the abatacept and tocilizumab groups, respectively (figure 2B). Overall, 36% of patients at week 52 achieved functional remission, defined as HAQ-DI≤0.5 in the abatacept group (figure 2B). Similarly, 28% of patients achieved functional remission in the tocilizumab group (figure 2B). The rate of functional remission reached a plateau at 24 weeks in the tocilizumab group, while it increased continuously for 52 weeks in the abatacept group (figure 2B).
Improvements in the HAQ-DI score were comparable between the two treatment group and there were no statistical differences (p=0.26).
CDAI variables and laboratory findings
In the next part of the study, the Clinical Disease Activity Index (CDAI) and the individual CDAI component (TJC, SJC, EGA and PGA) changes were analysed. Mean TJC improved significantly in the abatacept group (from 9.1 to 4.2) and in the tocilizumab group (from 8.7 to 3.6) between baseline and week 52 (figure 3A). Similar improvements were seen in mean SJC (6.7 to 2.1 in the abatacept group and 6.6 to 1.6 in the tocilizumab group). Mean EGA decreased significantly from baseline to week 52 in the abatacept group (from 50.1 to 23.5) and in the tocilizumab group (from 48.3 to 26.3). Similar improvements were also seen in the mean PGA (57.7 to 43.5 in the abatacept group and 56.9 to 41.1 in the tocilizumab group). Overall, mean CDAI decreased significantly in the abatacept group (26.6 to 12.9) and in the tocilizumab group (25.8 to 12.2) from baseline to week 52. Therefore, the magnitude of CDAI and CDAI component improvements was similar.

{kind=link}
{kind=link}
{kind=link}
Effects of treatment with abatacept and tocilizumab for 52 weeks on (A) the Clinical Disease Activity Index (CDAI) and CDAI component (mean tender joint count, swollen joint count, evaluator global assessment and patient global assessment), (B) laboratory findings (mean C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), matrix metalloproteinase 3 (MMP-3) and rheumatoid factor (RF)). DAS28, 28-joint count disease activity score.
However, when we evaluated DAS28-ESR in the two groups, we found that it decreased significantly from baseline to week 52 in the abatacept group (from 5.7 to 4.2) and in the tocilizumab group (from 5.6 to 3.1); the magnitude of improvement was greater in the tocilizumab group (figure 3A). The result may be because tocilizumab is an IL-6 antagonist, and IL-6 plays an important role in enhancing the inflammatory markers such as CRP and ESR that influence the value of DAS28 directly.
CRP levels in the abatacept group and tocilizumab groups were 2.1 mg/dL and 2.0 mg/dL, respectively, at baseline and decreased to 1.2 mg/dL and 0.3 mg/dL, respectively, at week 2, and 1.0 mg/dL and 0.3 mg/dL, respectively, at week 52 (figure 3B). Similar tendencies were also seen in ESR changes (figure 3B).
The MMP-3 levels in the abatacept and tocilizumab groups were 236.0 ng/mL and 205.6 ng/mL, respectively, at baseline and decreased to 153.2 ng/mL and 106.0 ng/mL, respectively, at week 52 (figure 3B). The RF titres in the abatacept and tocilizumab groups decreased from 166.3 and 176.6 U/mL, respectively, at baseline, to 147.0 and 161.6 U/mL, respectively, at week 52. The reductions in RF titres were not statistically significant either group (figure 3B).
Prediction for CDAI and HAQ-DI
We next performed subanalyses to identify factors associated with disease progression. In the abatacept group, examination of prognostic factors at baseline contributing to CDAI at week 52 showed that SDAI and RF titre were independent prognostic factors (table 2). The standardised partial regression coefficient of SDAI was 0.54 (p<0.001), and that of RF titre was −0.21 (p=0.02). On the other hand, RF titre and SDAI at baseline were not prognostic factors in tocilizumab group.
Independent predictors for CDAI at week 52 in multivariable analysis
Multiple regression analysis showed that previous use of a biological agent and baseline HAQ-DI score were significantly associated with CDAI after 52 weeks of tocilizumab treatment (table 2). The standardised partial regression coefficient of previous use of a biologic agent was 0.24 (p=0.01), and that of HAQ-DI score was 0.39 (p<0.001). However, these factors were not prognostic factors in the abatacept group.
Altogether, higher titres of RF and lower SDAI were associated with lower SDAI at week 52 in patients treated with abatacept, whereas lower HAQ-DI and no previous use of a biologic agent were associated in those receiving tocilizumab. Similar outcomes were obtained in the prognostic factors contributing to SDAI (see online supplementary table S3).
We next determined the prognostic factors contributing to HAQ-DI at week 52. In this analysis, baseline HAQ-DI and disease duration were identified as independent prognostic factors in both the abatacept and tocilizumab groups (table 3). The standardised partial regression coefficients of HAQ-DI were 0.70/0.64 (abatacept: p<0.001/tocilizumab: <0.001), and those of disease duration were 0.20/0.25 (p<0.001/<0.001). In other words, the factors associated with HAQ-DI at week 52 were shorter disease duration and lower HAQ at baseline in both groups.
Independent predictors for HAQ at week 52 in multivariable analysis
Discussion
To our knowledge, this is the first study comparing the efficacies of abatacept and tocilizumab and reporting the predictive factors of the response to treatment using propensity score matching.
A previous study examining the effects of abatacept and tocilizumab in clinical practice reported that the two drugs were effective in improving the SDAI and HAQ-DI.23 However, that study was not a RCT; thus, it is not clear if the two treatments were truly comparable. Our study employed propensity score matching and showed that abatacept and tocilizumab had comparable continuing efficacies, and that treatment with the drugs resulted in comparable clinical and functional remission rates.
In this study, clinical remission was assessed using the SDAI at week 52. Our results showed that the clinical remission rates of abatacept and tocilizumab were 18% and 20%, respectively, indicating that the two drugs had comparable efficacies. In addition to the last observation carried forward methods,25 the clinical remission rates were comparable by the non-responder imputation method and the analysis of as-observed data26 (see online supplementary table S4). However, a different result was obtained for the inflammatory reaction. Whereas only gradual improvements in CRP and ESR values were seen in the abatacept group, significant and rapid improvements were seen in the tocilizumab group 2 weeks after the start of treatment. This tendency was considered attributable to the inhibition of IL-6, which directly mediates inflammatory reactions.
Furthermore, no significant differences in the functional remission rates were observed between the two groups. Therefore, we considered that abatacept and tocilizumab had comparable efficacies for the treatment of RA, although tocilizumab was associated with greater improvement in the inflammatory reaction.
Predictors of the response to treatment exhibited a major difference between the two treatment groups. Patients with a lower SDAI and higher RF titre at baseline responded well to abatacept. Previous studies also reported a difference in the predictors of the response to treatment; patients who were positive for the anti-cyclic citrullinated peptide antibody were shown to respond well to abatacept,27 and patients with higher RF titres were shown to respond well to rituximab.28 ,29 In contrast, TNF inhibitors were more effective in patients with lower or negative RF titres.30 ,31 Thus, it is possible that T cell-targeting agents and B cell-targeting agents are more effective than TNF and IL-6 inhibitors in patients with seropositive RA.
The HAQ-DI at baseline was found to be a significant predictor of the response to tocilizumab treatment. This might be a characteristic of the drug, as another study has reported that patients with a lower HAQ-DI tended to respond well to tocilizumab.9 Moreover, shorter disease duration and a lower HAQ-DI at baseline were predictors of the functional improvement of both abatacept and tocilizumab when patients were evaluated with the HAQ-DI at week 52. These findings suggest that patients with advanced joint destruction are under the influence of damaged-associated HAQ-DI.32
This study used propensity score matching to assess the treatment efficacies of abatacept and tocilizumab. Most previous studies on the treatment of rheumatoid diseases were RCTs and not observational studies. However, the results of RCTs are not always applicable to daily clinical practice since the characteristics of patients entering the trials are largely determined by the inclusion/exclusion criteria.11 On the other hand, observational studies are subject to selection bias and typically result in differences in the background characteristics between the groups. The propensity scores were estimated using multivariate logistic regression analysis to reduce patient selection bias. By using this method, we were able to compare the efficacies of the drugs in two treatment groups with similar clinical backgrounds. Hence, the comparisons conducted in our study are comparable to data derived from RCTs.
Our study has several limitations. First, it was a single-centre study with inherent selection bias. However, we are confident about the results of the present analysis since a meta-epidemiological study showed that there was only a small difference between the results of single-centre and multicentre trials.33 Second, it was not possible to compare the drugs we used and TNF inhibitors since the rates of concomitant MTX treatment were about 65% for both the abatacept and tocilizumab groups, which is lower than the rates of concomitant MTX treatment in patients treated with TNF inhibitors. However, it should be noted that even if we performed a subanalysis by stratifying patients according to concomitant MTX, the clinical efficacy was similar between abatacept and tocilizumab (see online supplementary table S5). Third, our findings would need to be re-examined if a new confounding factor was discovered since the propensity score matching method cannot control for unknown confounding factors. Finally, we did not assess joint destruction by X-ray examination.
This study demonstrated that abatacept and tocilizumab had comparable continuing efficacies, and that treatment with the drugs resulted in comparable clinical and functional remission rates. Moreover, abatacept and tocilizumab showed similar effectiveness with or without MTX. The predictors of the response to treatment were a higher RF titre for abatacept and a lower HAQ-DI for tocilizumab. We believe that innovative statistical methods such as propensity score matching can contribute to the growing body of clinical evidence and might lead to the development of tailor-made medicine using biological products for patients with RA.
Acknowledgments
We thank Dr Wanying Li for improvements of the statistical methods.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online figures
- Data supplement 2 - Online tables
Footnotes
Handling editor Tore K Kvien
Contributors SK contributed to the study design, overall review, writing of the manuscript, and the other authors were involved in the performance of the study and review of the manuscript. YT, SN participated in the study design and coordination. All authors enrolled and managed patients in the clinic. All authors read and approved the final manuscript.
Funding This work was supported, in part, by a grant-in-aid for scientific research from the Ministry of Health, Labor and Welfare of Japan, the Ministry of Education, Culture, Sports, Science and Technology of Japan, and the University of Occupational and Environmental Health, Japan, through UOEH grant for advanced research.
Competing interests YT, has received consulting fees, speaking fees and/or honoraria from Abbvie, Daiichi-Sankyo, Chugai, Takeda, Mitsubishi-Tanabe, Bristol-Myers, Astellas, Eisai, Janssen, Pfizer, Asahi-kasei, Eli Lilly, GlaxoSmithKline, UCB, Teijin, MSD, Santen, and has received research grants from Mitsubishi-Tanabe, Takeda, Chugai, Astellas, Eisai, Taisho-Toyama, Kyowa-Kirin, Abbvie, Bristol-Myers. SH has received speaking fees, and/or honoraria from Abbvie.
Patient consent Obtained.
Ethics approval The ethics review board of the University of Occupational and Environmental Health, Japan.
Provenance and peer review Not commissioned; externally peer reviewed.