Article Text

Abstract
Objective This observational cohort study investigated the impact of biological (b) disease-modifying antirheumatic drugs (DMARDs) on the outcomes of serious infections (SIs) in patients with rheumatoid arthritis.
Methods We investigated outcomes of SIs observed in 947 patients enrolled in the German biologics register RABBIT(Rheumatoid arthritis: observation of biologic therapy). Outcomes were (1) recovery without complication, (2) sepsis following SI (≤30 days), and (3) death after SI without known sepsis (≤90 days). We applied a multinomial generalised estimating equation model for longitudinal data to evaluate the risks of sepsis and death simultaneously.
Results Sepsis within 30 days after SI was reported in 135 out of 947 patients, 85 of these had a fatal outcome. Fifty-three patients died within 90 days after SI without known sepsis. The adjusted risk of developing sepsis increased with age and was higher in patients with chronic renal disease. Compared with conventional synthetic (cs)DMARDs, the risk was significantly lower when patients were exposed to bDMARDs at the time of SI (OR: 0.56, 95% CI 0.38 to 0.81). Risk factors of fatal SI were higher age, use of glucocorticoids at higher doses and heart failure. Patients treated with bDMARDs and those with better physical function had a significantly lower mortality risk.
Conclusions These results suggest a beneficial effect of bDMARDs on the risk of sepsis after SI and the risk of a fatal outcome. Successful immunosuppression may prevent an unregulated host response to SI, that is, the escalation to sepsis. Further investigation is needed to validate these results.
- Rheumatoid Arthritis
- Infections
- Treatment
- DMARDs (biologic)
- Epidemiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Sepsis is a major concern in patients with serious infections (SIs) because it results in a case fatality rate of 30–50%.1 ,2 Older patients are particularly susceptible to sepsis because of hospitalisation, comorbidity and impaired physical function.3 Growing insights into the biological process of sepsis led to the improved management of this critical condition, but lethality remains high.4 Waage et al5 identified a potential target for the treatment of sepsis almost three decades ago. They found increased levels of tumour necrosis factor-α (TNF) in the serum of patients with sepsis. Tracey et al6 blocked TNF (cachectin) in an experimental study in baboons and demonstrated clinically relevant improvements in survival of sepsis. Beutler et al7 first reported a protective effect of immunisation against cachectin in mice. These promising findings demonstrated that TNF plays a key role in triggering sepsis. They prompted a sequence of randomised controlled trials wherein patients with sepsis were treated with different TNF inhibitors (TNFi).8–11 Similarly, antagonists of the interleukin (IL) 1 receptor were targeted. An overview of trials is given in Remick et al.12 Almost consistently, none of these trials showed a significant improvement in survival of patients treated with TNFi, which led to the conclusion that TNF blockade is not a useful treatment for sepsis. However, in these studies the biological cascade of sepsis had already started in all patients and the treatment may have been administered too late to stop this process.1 ,12 ,13 The importance of the timing of TNF blockade was also shown in an experimental study with baboons.6 Of three groups (no TNFi, TNFi 1 h prior or 2 h prior), only those baboons that were treated 2 h prior to infection survived.6 This result corresponds with Beutler et al7 who found that the timing between immunisation and infection was crucial for survival.
TNFi were established as first biologic disease-modifying antirheumatic drugs (bDMARDs) in the routine care of moderate to severe rheumatoid arthritis (RA) after failure of conventional synthetic (cs)DMARDs. Other bDMARDs have been approved since 2006 that target the CD20 antigen on B lymphocytes (rituximab), suppress T cell activation (abatacept) or inhibit the binding of IL-6 to its receptor (tocilizumab). Due to their immunosuppressive effect, bDMARDs increase the risk of SI in patients with RA who are per se at higher risk of SI due to comorbidities, complications of disease-related joint surgeries and impaired physical function.14–19
Notably, none of the above mentioned studies investigated the outcomes of SI such as (1) recovery from SI, (2) escalation of SI to sepsis or (3) death. The present investigation focuses on patients with RA who acquired SI after enrolment into the German biologics register RABBIT (Rheumatoid arthritis: observation of biologic therapy). We examined the contribution of RA treatment and patient characteristics to the three different outcomes of SI using multinomial regression analysis. We also investigated the overall risk of death within 90 days after the onset of SI.
Statistics and methods
Patients and events of interest
The present study was conducted using data from the German biologics register RABBIT, which is an ongoing observational cohort study. Since May 2001, patients with RA have been eligible for enrolment at the start of treatment with a bDMARD or csDMARD after failure of at least one csDMARD.20 A total of 12 097 patients were enrolled in RABBIT by 30 October 2013. The focus of this paper is the outcome of SIs. Therefore 947 patients who developed one or more infections that were classified as serious according to International Council for Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH) definition21 were included. In the main analysis we excluded 108 SIs in 88 patients with incomplete information on the SI. The main analysis is therefore based on all separable SIs (n=1017) of 859 patients. Patients were considered to be exposed to a particular DMARD when the SI occurred during active treatment with that DMARD, that is, no missed dose before the SI.
Assessments and follow-up
Clinical status was assessed at baseline, months 3 and 6, then every 6 months for 5–10 years.
Rheumatologists reported DMARD exposure (start and stop dates, doses), adverse events, disease activity (including components of the disease activity score based on a 28-joint-count (DAS28)) and comorbidities. Patients reported among other items on physical function using the Hannover Functional Status Questionnaire (FFbH). Its scores can be transformed to the Health Assessment Questionnaire values.22 If serious adverse events were reported the rheumatologist was asked to provide detailed clinical information including hospital discharge letters.
Adherence to scheduled follow-ups was monitored and investigations of dropouts or the reasons for the discontinuation of study participation were performed. This includes inquiries to local administration offices regarding patients’ vital status and cause of death. For further details see.20
Objective
The objective was to examine the impact of patients’ clinical characteristics and RA treatment with TNFi, other bDMARDs, csDMARDs and glucocorticoids on the risk of developing sepsis or a fatal outcome of SI. Three approaches were applied. Approach A (figure 1) investigates the risks of sepsis and death after SI simultaneously and thus includes validated cases of fatal and non-fatal sepsis plus all deaths within 90 days after SI. With this approach we addressed possibly undetected and fatal cases of sepsis after SI. In approach B, the risk of death due to sepsis was investigated. The overall risk of death after SI, with and without sepsis, was addressed in approach C.

Investigation of SI outcomes. Boxes in colour indicate the outcomes of interest and boxes in black indicate the reference population. Approach A examined the risks of sepsis and death after SI simultaneously; this approach accounts for possibly undetected but fatal cases of sepsis (see: objectives & methods). Approach B focuses on the mortality risk of sepsis. Overall mortality after SI was examined in approach C. All sensitivity analyses were applied in the setting of approach A. GEE, generalised estimating equations; SI, serious infection.
Statistical analyses
Model-based analyses
Units of investigation in this analysis were SIs. In approach A two possible outcomes of SI, sepsis (including death from sepsis) and mortality without known sepsis, were investigated simultaneously. These analyses are similar to analyses of competing risks in survival data.23–25 It was crucial to include overall mortality in the analysis in order not to miss undetected cases of sepsis. In approach A (figure 1) we applied a recently introduced generalised estimating equations model for longitudinal and multinomial responses26 to investigate the risks of sepsis and death as outcomes of SI simultaneously. This model class takes dependencies of subsequent SI in one patient into account. It is implemented in the statistical software R27 ,28. A similar approach was applied in time-discrete analyses of competing risks of hospital-acquired methicillin-resistant Staphylococcus aureus infections by Barnett et al.29
A generalised estimating equations model with the binary outcome mortality yes/no was used in approach C. However, since only two patients developed sepsis twice, in approach B the analysis was restricted to the last sepsis per patient and multiple logistic regression was applied.
Sensitivity analyses
The consistency of results was investigated in four different sensitivity analyses. Analysis I comprised the subset of patients with pneumonia. In a second analysis we aimed to detect the influence of bDMARD discontinuation and therefore restricted the group of patients on csDMARD treatment at the time of SI to those naïve to biologics. The third sensitivity analysis addressed the impact of incomplete data and uncertain DMARD exposure and included 108 additional SIs with incomplete information. In these patients we assumed that the last known DMARD exposure during follow-up in RABBIT persisted at the time of SI. Analysis IV comprises dropouts with no reported events of sepsis or death and a follow-up of less than 180 days after the last SI. In this most conservative approach, we assumed that dropout occurred due to sepsis only for bDMARD-treated patients and artificially imputed these events to the data.
Results
Serious infection
Among all 1017 SIs with complete information, pneumonia was most frequent (n=332, 28.4%), followed by 131 infections of bones and joints (11.2%) and 120 respiratory infections other than pneumonia (10.3%). The complete spectrum of SIs is documented online (see online supplementary figures S1 and S2). We found no differences in the spectrum of SIs after stratification into (1) patients with and without subsequent sepsis and (2) bDMARD versus csDMARD treatment at the time of SI. 137 SIs escalated to sepsis within 30 days (11.7% of all SIs), two patients developed sepsis twice. The case fatality rate was 63% (85 deaths in 135 patients, figure 1). Out of 859 patients who did not develop sepsis, 53 died within 90 days following SI (6.2%).
Patient characteristics
Patients with SI were significantly older, had a longer disease duration, higher disease activity and more comorbidities at baseline than patients in the remaining cohort (table 1, p<0.01). Among patients with SI those who developed sepsis or died due to SI had significantly poorer clinical characteristics than patients with no further complications of SI, particularly heart failure and renal disease were considerably more frequent.
Characteristics of patients with complete information of SI (n=859) at baseline and at the time of SI, compared with the remaining cohort and stratified by outcome of SI
Baseline treatment was similar in patients with SI and the rest of the cohort. Disease activity (DAS28 and C reactive protein), at the last regular time point before the SI, was significantly reduced compared with baseline. The median time from the last regular study visit to SI was 3.7 months (IQR: 1.9 to 6.2). Treatment with bDMARDs was significantly less frequent at the time of SI than at baseline, especially in patients who developed sepsis or died after SI (table 1, p<0.01).
We categorised patients according DMARD exposure at the time of SI to investigate a possible patient channelling between enrolment and the SI (table 2). We found significant differences between treatment regimens only for age (p<0.01). Disease activity, physical function, erythrocyte sedimentation rate (ESR), CRP and prevalence of heart failure or chronic renal disease did not vary significantly between groups of DMARDs. Among patients treated with csDMARDs at the time of SI almost two-thirds (63.7%) were previously treated with bDMARDs.
Characteristics of patients stratified by the class of DMARD exposure at the time of SI
In the subpopulation of patients with pneumonia, male patients were more frequent in the csDMARD and other bDMARD groups. Further, patients treated with csDMARDs only were significantly older than those treated with bDMARDs (p<0.01). Other disease characteristics, for example, DAS28 and physical function, were not different (see online supplementary table S2).
Risk of sepsis and mortality
The adjusted OR of developing sepsis increased significantly with age. Risk was higher in patients with chronic renal disease and lower in patients with better function. The risk was significantly reduced when patients were exposed to TNFi or other bDMARDs at the time of the SI (table 3). Risk of death after SI was significantly higher in patients with congestive heart failure and in older patients. Treatment with any class of bDMARDs and better physical function (FFbH) had significant protective effects regarding mortality. No significant association with the risk of sepsis or death was found for sex. Disease activity (DAS28) was not included in the adjusted model because it was not associated with sepsis or mortality in the univariate analysis (see online supplementary table S1). Diabetes was significantly associated only in the univariate analysis, therefore we excluded diabetes from the multiple regressions for model sparsity and included only the strongest predictors, renal disease and heart failure (see online supplementary table S1). Similar results were obtained in a subsample of patients with pneumonia (n=298, see online supplementary table S3).
Results of the GEE model for longitudinal multinomial regression on the risks of sepsis (n=137) and death (n=53) after SI (n=1017)
Discontinuation of bDMARDs and the risk of sepsis
In the analysis above, the sepsis and mortality risks of patients exposed to bDMARDs at the time of SI were compared with those unexposed. In this approach we had pooled bDMARD-naїve patients and those who discontinued bDMARDs during follow-up. In the following analysis we considered first SIs only and categorised patients into (A) biologic-naїve, (B) exposed to bDMARDs and (C) bDMARD withdrawn prior to first SI. The restriction to first SI was applied to omit an effect of treatment decisions based on previous SI.
In bDMARD-naïve patients 133 first SIs were observed, 515 in patients exposed to bDMARDs and 211 in patients who had discontinued bDMARDs >1 month prior to the first SI. The latter patients had significantly longer disease duration, lower physical function, higher disease activity (DAS28) and were more often affected by heart failure and renal disease than bDMARD-naїve patients (see online supplementary table S4). Sepsis occurred in 39 (18.4%) out of 211 SIs which was similar to biologic-naïve patients (23/133, 17.3%) and more frequent than in patients exposed to bDMARDs at the time of the first SI (58/515, 11.3%).
Adjustment for age, sex, comorbid conditions (heart failure, renal disease), physical function and glucocorticoid dose by means of multinomial regression resulted in a similar risk of sepsis (adjusted OR: 0.97, 95% CI (0.56 to 1.70)) and mortality (adjusted OR: 0.96, 95% CI (0.42 to 2.17)) for patients who discontinued bDMARDs prior to first SI compared with biologic-naїve patients (reference category). The adjusted risks were significantly lower for patients exposed to bDMARDs at SI (OR (sepsis): 0.57 (0.34 to 0.97), OR (death): 0.34 (0.15 to 0.80)) compared with biologic-naїve patients (see online supplementary table S5).
Mortality after SI and sepsis
Adjustment in the analyses of mortality after sepsis was restricted to age, sex, treatment with bDMARDs and comorbid heart failure because of the low number of fatal outcomes of sepsis. Treatment with TNFi, but not with other bDMARDs, was significantly associated with a lower case fatality rate of sepsis (approach B). All-cause mortality after SI, irrespective of the development of sepsis, was significantly reduced for the use of TNFi and other bDMARDs (approach C, table 4).
ORs of multiple logistic regression for mortality after sepsis (85 deaths in 135 patients, approach B) and of a GEE-type regression model for all-cause mortality (138 deaths in 859 patients, approach C)
Sensitivity analyses
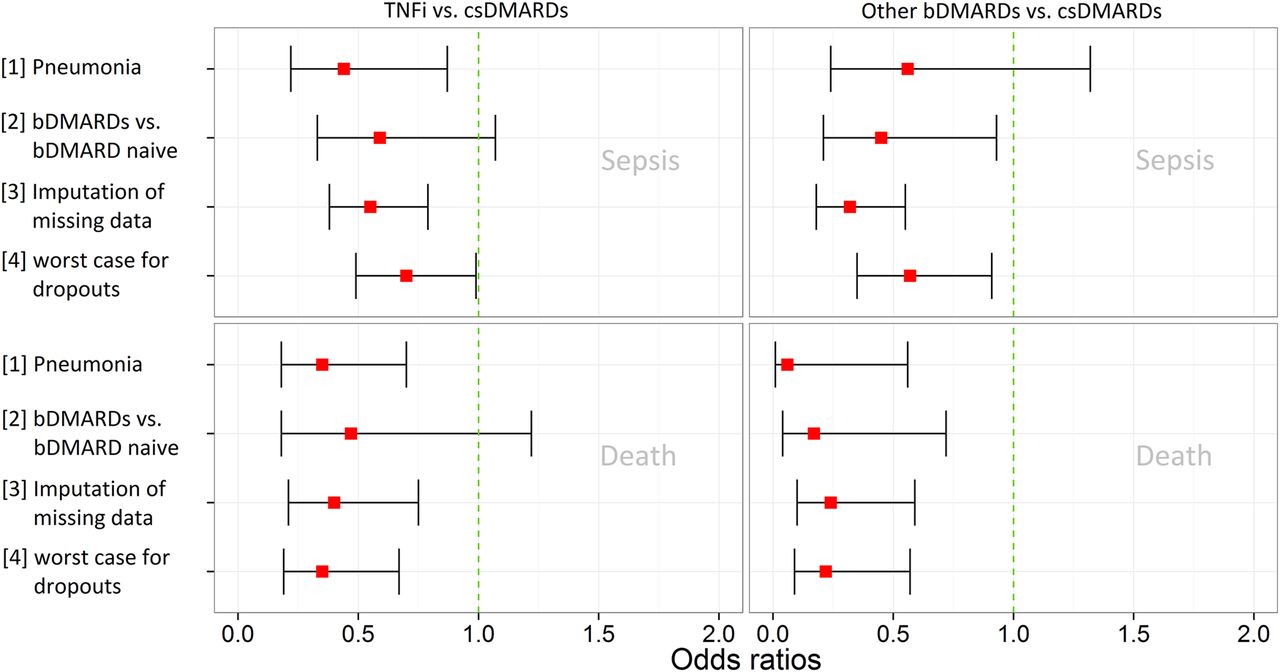
ORs of the risk of sepsis and death for exposure to bDMARDs compared with csDMARDs remained consistently below 1 throughout all four sensitivity analyses (figure 2). The reduction of the study population in analyses 1 and 2 produced wider CIs but consistent estimates. Analysis 3, incorporating 108 SIs with incomplete information, strengthened the results. In the most conservative analysis 4 we imputed the event of sepsis only to those 29 out of 50 dropouts who were exposed to bDMARDs (TNFi: n=17, other bDMARDs: n=12). However, the overall protective effect of bDMARDs remained significant.

{kind=link}
{kind=link}
Results of sensitivity analyses show ORs and respective confidence intervals of TNFi vs. csDMARDs and other bDMARDs vs. csDMARDs. Approach [1]: analysis in a subsample of patients with pneumonia, approach [2]: patients at csDMARD treatment were restricted to biologic naïve patients; approach [3]: 108 infections with unknown date and exposure were included, the last known DMARD exposure was ‘carried forward’ to the respective event of sepsis (n=47) or death (n=19), in approach [4] we assumed in a most conservative manner that all patients who dropped out but were previously treated with bDMARDs had a sepsis (n=29). bDMARD, biologic DMARD; csDMARD, conventional synthetic DMARD; DMARD, disease-modifying antirheumatic drug; TNFi, tumour necrosis factor α inhibitors.
Discussion
This is the first study that investigated simultaneously the risks of sepsis and mortality as possible outcomes of SIs in patients with RA. An SI escalated to sepsis or preceded the patient's death in one of five patients. Patients with heart failure, renal disease and at higher age exhibited an increased risk of both adverse outcomes. Patients who were exposed to bDMARDs at the time of SI had a significantly reduced risk of developing sepsis. Similarly, bDMARD treatment significantly lowered the risk of a fatal outcome of SI. A similar result concerning overall mortality after SI was made by Galloway et al30 with data from the British Society of Rheumatology: Biologics Register (BSRBR); they found for TNFi versus csDMARD an adjusted OR of 0.50 (95% CI (0.3 to 0.8)). We also found that mortality after sepsis was significantly lower when patients were exposed to bDMARDs at the time of SI. These findings are consistent with experimental studies in animals6 ,7 which suggest that TNFi effectively prevents sepsis.
A secondary but important result of this study addresses the impact of discontinuing bDMARD treatment on the risk of sepsis and death after SI. It is common knowledge that initiation of bDMARD therapy increases the risk of SI.14–19 Further, discontinuation of bDMARDs is supposed to decrease the risk of SI. Regarding the risks of sepsis or death after SI our results suggest a different mechanism: adverse outcomes of SI (sepsis and death) were more likely in biologic-naïve patients than in patients exposed to bDMARDs at the time of SI (see online supplementary table S5, Sensitivity analysis 2) which could indicate a protective effect of bDMARDs. This double-edged effect of bDMARDs has been described very recently as the ‘dual’ role of TNFi regarding septic arthritis.31 The authors referred to an experimental study which showed protective effects of TNFi against septic arthritis.32 In our study the protective effect receded when bDMARDs were discontinued: the risk of developing sepsis or of dying after SI was similar in patients who had discontinued bDMARDs at least 30 days before the SI and in biologic-naїve patients (see online supplementary table S5).
We performed four sensitivity analyses to test the robustness of the results. The most conservative, or worst-case scenario, which assumed that all bDMARD-treated patients with insufficient follow-up had developed sepsis (Sensitivity analysis 4, figure 2) did not reveal diverging results.
A strength of our study is the simultaneous investigation of sepsis and mortality after SI. This approach prevented the omission of cases which died from undetected sepsis. Furthermore, we adjusted for possible imbalances between DMARD groups in all analyses (age, sex and important risk factors).
There are possible shortcomings of our study. We have found a similar spectrum of SIs across bDMARDs and csDMARDs (see online supplementary figure S2), but a residual chance remains that subtypes of SI are differentially distributed. To minimise this bias we performed a subanalysis of patients with pneumonia which showed consistent results. However, our data do not comprise sufficient pathogen classification to investigate bacterial pneumonia and viral pneumonia separately. Additionally, the numbers of patients and events did not permit discrimination between effects of particular bDMARDs.
Another uncertainty rests with the complexity of the clinical course, the symptoms and the severity of SI and sepsis. There could be a suspicion bias, meaning that patients treated with bDMARDs who develop an SI could be hospitalised faster than those on csDMARDs. This would lead to earlier detection and treatment and thus better outcome of sepsis. We have no indication of such bias since the hospitalisation rates and the spectrum of SIs were equal among the treatment groups. In addition, in RABBIT all diagnoses and serious adverse events are validated and classified by the study physician in a blinded manner, that is, unaware of the DMARD exposure of the respective patient.
In conclusion, this study suggests that patients exposed to bDMARDs at the time of SI have a reduced risk of sepsis and mortality. The effective immunosuppression via bDMARDs may prevent an unregulated host response to SI and the development of sepsis. Discontinuation of bDMARDs seems to shift the risk from an increased susceptibility to SI to more severe outcomes. Nonetheless, we cannot conclude from our study that bDMARDs should be continued in case of an SI since this is the first study showing these results. They have to be confirmed by other studies before any clinical consequences can be drawn.
Acknowledgments
The authors thank all participating rheumatologists for their support of RABBIT. Particularly: Klopsch T, Krause A, Liebhaber A, Richter C, Bergerhausen H, Tony H, Dockhorn R, Rockwitz K, Eisterhues C, Bussmann A, von Hinuber U, Demary W, Grasler A, Kapelle A, Kekow J, Wassenberg S, Wilden E, Ochs W, Burmester G, Zinke S, Krummel-Lorenz B, Edelmann E, Remstedt S, Meier L, Bohl-Buhler M, Aringer M, Kellner H, Berger S, Balzer S, Pick D, Stille C, Tremel H, Lebender S, Kruger K, Korber H, Stander E, Thiele A, Karberg K, Wiesmuller G, Weis K, Kuhne C, Schwarze I, Burmester G, Backhaus M, Zanker M, Herzer P, Sorensen H, Fricke-Wagner H, Schulze-Koops H, Grunke M, Harmuth W, Spathling-Mestekemper S, Dexel T, Alliger K, Moosig F, Schneider M, Schuch F, Wendler J, Kleinert S, Grebe T, Manger K, Karger T, Menne H, Fliedner G, Gauler G, Walter J, Reck A, Hamann F, Krause D, Hantsch J, Rech J, Seifert A, Schmitt-Haendle M, Biewer W, Leumann K, Prothmann U, Mobius C, Gause A, Eidner T, Euler H, Wiesent F, Fischer K, Petersen V, Riechers E, Alten R, Mobius E, Mark S, Rump J, Sekura M, Teipel A, Dahmen G, Jahn A, Kittel G, Hauser M, Donath G, Henes J, Zeh G, Schroder J, Hohle M, Haux R, Zeidler G, Jendro M, Liman W.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
Contributors AR, JL, AZ and AS had full access to all data of this study and take responsibility for data integrity and accuracy of the analysis. Study concept and design: JL, AZ, AS. Acquisition of the data: MS, AK, TK, JK. Analysis and interpretation of the data: AR, JL, AZ, AS. Drafting the manuscript: AR. Critical revision of the manuscript for important intellectual content: AR, JL, MS, AK, TK, JK, AZ, AS. Obtained funding: JL, AZ, AS. Study supervision: JL, AZ, AS, MS.
Funding The German Biologics Register RABBIT is supported by a joint, unconditional grant from AbbVie, Bristol-Myers Squibb, MSD Sharp & Dohme, Pfizer, Roche and UCB.
Competing interests MS: Grant/Research Support: Abbvie, Actelion, Merck Serono, Pfizer, Roche. Consultant for: Abbvie, Roche, UCB. Speakers Bureau with: Abbvie, Chugai, Roche, Pfizer, UCB. AK: Consultant for: MSD, UCB, Chugai Roche, Research Support: Abbvie, Chugai, Roche, MSD, Pfizer, UCB, Lecture honoraria: Amgen, Pfizer, Abbvie, Chugai, Roche. AZ: Lecture honoraria: BMS, Merck-Sharp & Dohme, Pfizer, Roche, UCB. AS: Lecture honoraria: BMS, Merck-Sharp & Dohme, Pfizer, Roche, Sanofi-Aventis.
Patient consent Obtained.
Ethics approval The ethics committee of the Charité- Universitätsmedizin Berlin.
Provenance and peer review Not commissioned; externally peer reviewed.