Article Text

Abstract
Objectives Events in the lungs might contribute to generation of anticitrullinated protein antibodies (ACPA) in rheumatoid arthritis (RA). We investigated if signs of immune activation are present in bronchial biopsies and bronchoalveolar lavage (BAL) of patients with early-untreated RA without clinical signs of lung involvement.
Methods Twenty-four patients with RA with symptom duration <1 year and naïve to disease-modifying antirheumatic drugs were subjected to bronchoscopy where BAL and mucosal bronchial biopsies were retrieved. For comparison, 15 bronchial biopsies and 79 BAL samples from healthy volunteers were available. Histological examination was performed to evaluate lymphocyte infiltration, presence of immune cells (T and B cells, plasma cells, dendritic cells and macrophages) and immune activation markers. Cell composition of BAL samples was analysed by differential counting and T cell subsets by flow cytometry.
Results Lymphocyte infiltration was more frequently found in ACPA-positive patients (50%) as compared with ACPA-negative patients (17%) and controls (13%). Germinal centres, B cells and plasma cells were only found in ACPA-positive patients. The frequency of T cells in bronchial biopsies of patients with ACPA-positive RA was positively associated with expression of immune activation markers. BAL samples of patients with ACPA-positive, but not ACPA-negative, RA had significantly higher relative numbers of lymphocytes and expressed higher levels of activation markers compared with controls.
Conclusions Signs of immune cell accumulation and activation are present both in the bronchial tissue and in BAL of untreated patients with early RA without concomitant lung disease, strengthening the role of the lung compartment as an important player in ACPA-positive RA.
- Rheumatoid Arthritis
- Ant-CCP
- T Cells
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA) is an autoimmune disease characterised by chronic inflammation of the joints. Presence of anticitrullinated proteins antibodies (ACPA) in approximately two-thirds of the patients with RA defines a more aggressive disease phenotype.1 ACPAs develop prior to the onset of symptomatic joint disease2 ,3 and associate with smoking,4 suggesting that the RA-associated autoimmune responses are initially generated outside the joints, and perhaps at a mucosal site.5 Smoking increases expression of citrullinated proteins and peptidylarginine deiminase type 2 (PAD2) in the lungs of healthy smokers,6 ,7 and we have recently confirmed this finding in patients with early untreated RA as well.8 Interestingly, increased expression of citrullinated proteins in RA was present in smokers as well as in ACPA-positive non-smokers, suggesting that factors other than smoking might also contribute to generation of citrullinated epitopes in the lungs. Identification of shared citrullinated epitopes in the lungs and joints of patients with RA 9 together with local enrichment of ACPA in the bronchoalveolar lavage (BAL) of patients with early untreated RA and in the induced sputum of arthritis-free individuals at risk for developing RA10 support the notion that RA-associated autoimmunity might indeed initiate in the lung compartment.11 In line with this, ectopic lymphoid structures containing citrullinated protein-binding B cells have previously been reported in patients with established RA and associated lung disease.12 More recently, similar structures were described in lung biopsies of ACPA-positive individuals with associated interstitial lung disease, but no signs of joint inflammation.13 However, no such studies are available in patients with untreated and/or early RA.
In this study, we, therefore, wanted to characterise lymphocytic infiltration both in the large and small airways from patients with early untreated RA without clinical lung disease. To accomplish this, we analysed bronchial biopsies from the large airways and BAL samples reflecting the small airways and alveoli. Our results show the presence of lymphoplasmacytic infiltration and immune cell activation, with occasional germinal centre formation. These changes are restricted to patients with ACPA-positive RA, both smokers and non-smokers. Our findings further support a potential important role of the lung compartment in the pathogenesis of ACPA-positive RA.
Material and methods
Patients and controls
Patients included in the LUng investigation in early RA (LURA) cohort8 at Karolinska University Hospital in Stockholm, referred from primary care centres because of recent onset of self-reported joint problems, were asked at inclusion in the study about their willingness to participate in bronchoscopy. Twenty-one per cent (24/105) of the patients agreed to undergo bronchoscopy, with retrieval of mucosal bronchial biopsies and BAL. Disease activity using DAS28-ESR score, presence of IgM and IgA rheumatoid factor and IgG ACPA (anti-CCP2 kit, Immunoscan RA Mark 2; Euro-Diagnostica, Arnhem, The Netherlands) and smoking history were assessed at inclusion. High-resolution CT (HRCT) was performed in all patients within 1 week after the diagnosis was made at the rheumatology clinic and reviewed for abnormalities in random order and double blinded in accordance with the criteria included in the International Classification of HRCT for occupational and environmental respiratory diseases,14 as previously described in detail.8 Spirometry was performed according to a standard protocol measuring forced expiratory volume in 1 s (FEV1) and vital capacity (VC) using a spirometer (Vmax 229-6200 Legacy, USA). The carbon monoxide diffusing capacity (DLCO) was measured by single breath method, and corrected for haemoglobin. The values are expressed as percentages of the predicted values according to European Coal and Steel Community references.15
Non-steroidal anti-inflammatory drugs and joint injection with glucocorticoids were allowed according to clinical indication. Antirheumatic treatment with methotrexate and glucocorticoids was started after bronchoscopy.
As a control group, healthy age-matched never smokers and current smokers with normal lung function from the Karolinska COPD and Smoking from an OMIC Perspective (COSMIC) cohort was used16 consisting of 79 healthy volunteers who underwent bronchoscopy and BAL. Another 15 individuals served as a control group for comparison of biopsies.
Demographic characteristics of the patients and controls are summarised in table 1.
Demographic characteristics of the patients
Bronchoscopy, BAL and biopsy retrieval
Bronchial mucosal biopsies were taken from segmental and subsegmental septa in the lung. In order to obtain BAL fluid, the bronchoscope (Olympus) was wedged in a middle lobe bronchus and five aliquots of 50 mL each of phosphate buffered saline were instilled. The fluid was gently suctioned back into a bottle kept on ice. Dwell-time was kept to a minimum in agreement with the guidelines.17 No aspirate was discarded. The bronchoscopic procedure and handling of BAL fluid have previously been described in detail.18 ,19 Bronchial biopsies were either embedded in paraffin or snap-frozen in dry ice-cooled methanol. Serial cryostat sections of 7 µm thickness were 2% formaldehyde fixed and stored at −80°C.
Histology and immunohistochemical staining
Paraffin embedded and/or frozen section biopsies obtained from both patients with RA (n=24) and controls (n=15) were stained with H&E for standard histology. Additionally, frozen biopsies obtained from patients with RA (n=24) were evaluated by immunohistochemistry for detection of activation-induced cytidine deaminase (AID), T cells (CD3), B cells (CD19), dendritic cells (DCIR), plasma cells (CD138), macrophages (CD68) peptidyl arginine deiminase 2 (PAD2) and immune cell activation markers (HLA-DR and HLA-DQ) according to a previous published protocol.20 Results were evaluated by double blind semiquantitative evaluation (GR and ME) on a four-point scale: 0, no staining; 1, low amount of staining; 2, intermediate amount of staining and 3, high amount of staining. Results are expressed as a median of the two independent observations. Additionally, biotinylated citrullinated and native forms of the enolase-peptide 5–21 were used to stain infiltrates in bronchial biopsies. Details on the antibodies used for immunohistochemistry are summarised in online supplementary table S1.
Flow cytometric analyses
BAL fluids from both patients with RA (n=24) and healthy volunteers (n=79) were strained through a Dacron net (Millipore, Cork, Ireland) and centrifuged. Cell pellets were resuspended in phosphate buffer saline (PBS) and stained for CD4, CD8, CD25, CD27, CD28, CD69, CD103, CXCR3, HLA-DR (all antibodies from BD Biosciences, San Jose, California, USA) and FOXP3 (eBioscience) as previously described.21 A detailed summary of the monoclonal antibodies used is given in online supplementary table S2.
Statistical analysis
Differences between groups were analysed using non-parametric (Mann–Whitney) or parametric (non-paired t test) tests when appropriate. One-way analysis of variance with Tukey post hoc test was used for multiple group comparisons. Statistical comparisons and graphs were performed using the GraphPad Prism software V.5.02. A p value of <0.05 was considered statistically significant.
Results
Lung function and HRCT findings
Higher proportions of ACPA-positive patients as compared with ACPA-negative patients had both evidence of airflow limitations with an FEV1/VC <0.7 (10/18, 56% as compared with 2/6, 33%; non-significant) and decreased gas transfer with a DLCO <80% of predicted values (9/18, 50% as compared with 1/6, 17%; non-significant). A large majority of patients with RA (22/24, 92%) had lung abnormalities on HRCT, with patients with ACPA-positive RA having a higher prevalence of both parenchymal (12/18, 67%) and airway (6/18, 30%) changes as compared with patients with ACPA-negative RA (3/6, 50% having parenchymal changes and none having airway changes). Air trapping was detected in 38% of the ACPA-positive patients and 67% of the ACPA-negative patients. ACPA-positive patients were more often ever (83%) and current (50%) smokers compared with ACPA-negative patients (67% ever smokers and 17% current). Heavy smoking (more than 10 pack-years) was, however, equally occurring in patients with both APCA-positive (65%) and ACPA-negative (75%) RA.
Histopathological characterisation of bronchial biopsies in early untreated RA
Examination of H&E stainings revealed frequent presence of lymphocytic infiltration in patients with ACPA-positive RA (9/18 patients, 50%) and to a lesser extent in patient with ACPA-negative RA (1/6, 17%, p>0.05) and controls (2/15, 13%, p<0.05), (figure 1A–D). Occasional formation of germinal centre-like structures (2/18, 11%) was observed only in patients with ACPA-positive RA (figure 2A). These structures were positive for B-cell markers (figure 2C) and AID (figure 2B) and stained positively with biotinylated cit-enolase (figure 2F).

Lymphocytic infiltration is present in the bronchial biopsies of patients with anticitrullinated protein antibodies (ACPA)-positive untreated early rheumatoid arthritis (RA). H&E representative stainings of bronchial biopsies from patients with ACPA-positive (A) and ACPA-negative RA (B), as well as healthy volunteers (C). Graph showing the frequency of lymphocytic infiltration in ACPA-positive patients versus ACPA-negative patients and healthy volunteers (D). *p<0.05.
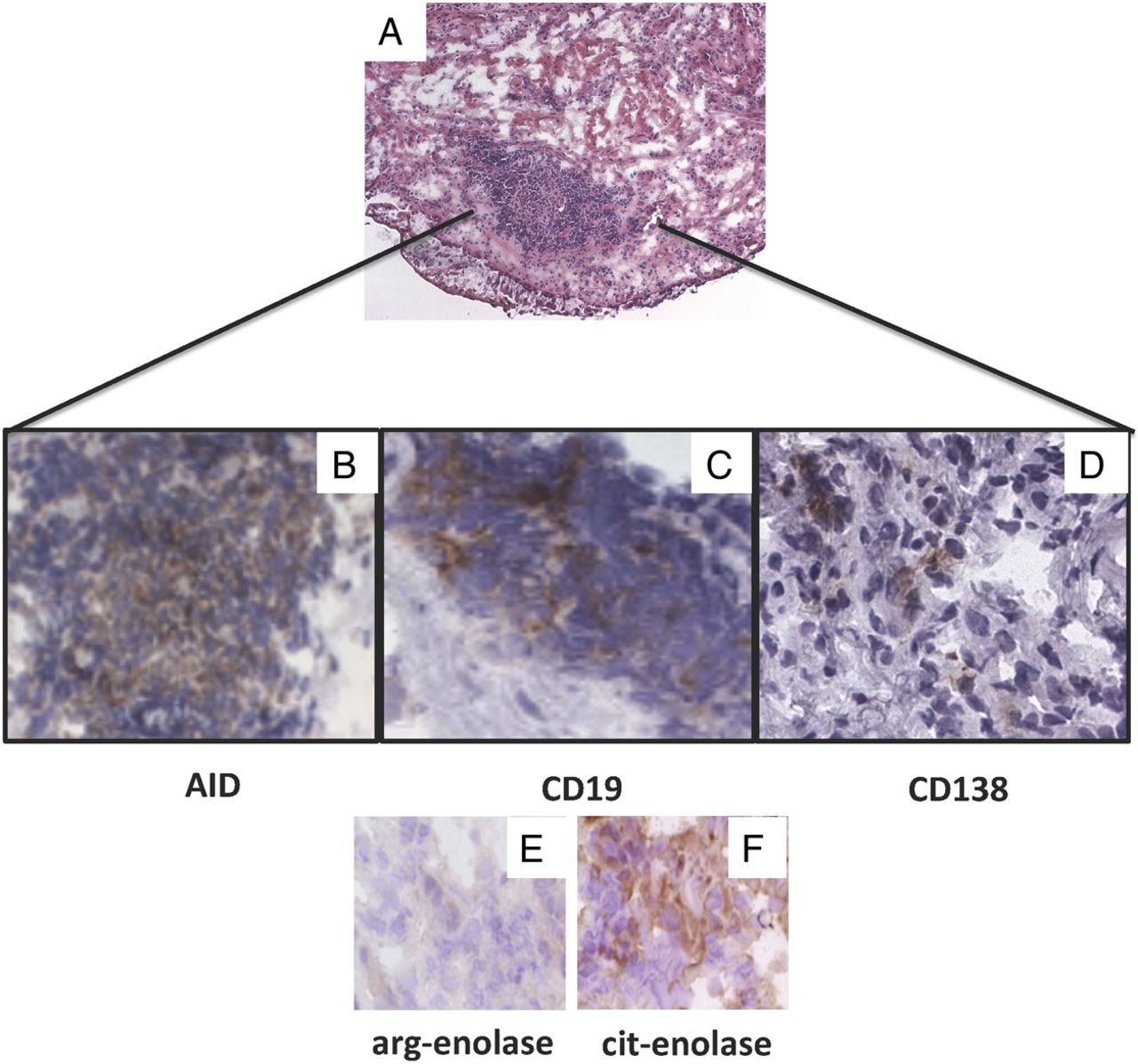
Germinal centre-like structures are present in bronchial biopsies of patients with anticitrullinated protein antibodies (ACPA)-positive untreated early rheumatoid arthritis (RA). Histological analysis of H&E stainings showing germinal centre formation in the bronchial biopsies of a patient with ACPA-positive untreated early RA (A). Immunohistochemistry showing brown diaminobenzidine (DAB) staining of germinal centre structures using antibodies against activation-induced cytidine deaminase (AID, B), CD19 (C), CD138 (D) and biotinylated citrullinated (F), but not native (E) enolase peptide 5–21.
B cells (CD19+ cells) and plasma cells (CD138+ cells) were only found in ACPA-positive patients (4/18 for CD19+ cells and 6/18 for CD138+ cells). T cells showed a tendency to be more frequent in ACPA-positive patients (median score 2, range 1–3) as compared with ACPA-negative patients (median score 1, range 1–3), but the difference did not reach statistical significance (figure 3A, D, G). Expression of immune activation markers was higher in patients with ACPA-positive RA as compared with those with ACPA-negative RA for both HLA-DR (median of 3, range 2–3 as compared with a median of 2, range 1–3, p<0.05, figure 3C, F, I) and HLA-DQ (median of 2, range 0–3 as compared with a median of 1, range 1–3, p<0.05, figure 3B, E, H). No difference in expression levels of PAD2 was detected.
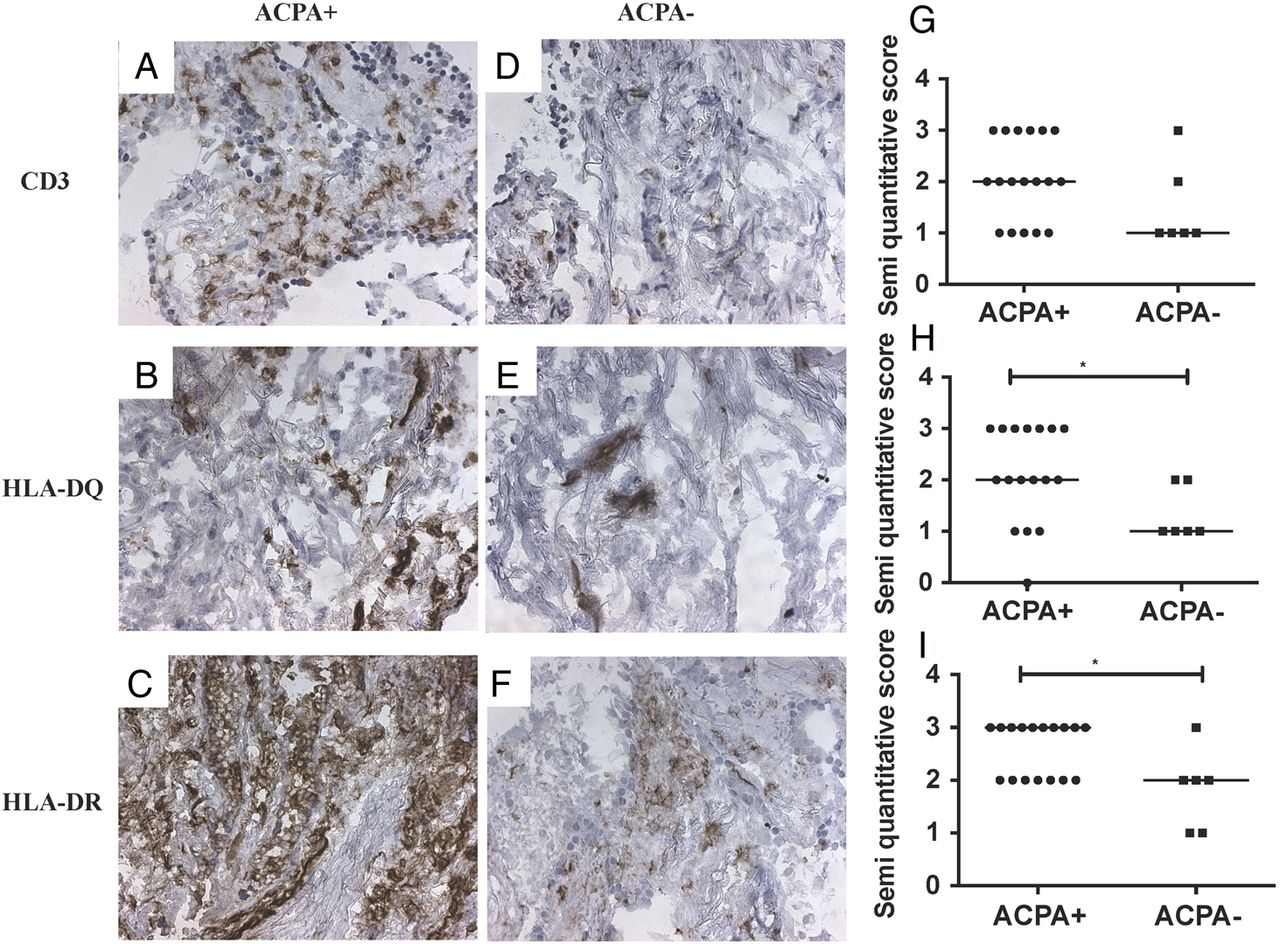
Signs of immune activation are present in bronchial biopsies of patients with anticitrullinated protein antibodies (ACPA)-positive untreated early rheumatoid arthritis (RA). Immunohistochemistry showing brown diaminobenzidine (DAB) staining for cell surface markers in bronchial biopsies of ACPA-positive (A–C) and ACPA-negative (D–F) untreated early RA. Graph showing results from the semiquantitative analysis of CD3 (G), HLA-DQ (H) and HLA-DR (I) expression. *p<0.05.
Characterisation of BAL cell populations
ACPA-positive patients had significantly higher relative numbers of BAL lymphocytes (p<0.05, figure 4A) and significantly reduced relative numbers of BAL macrophages (p<0.05, figure 4B) as compared with controls, while no such differences were observed for ACPA-negative patients. The same differences were observed when patients with ACPA-positive RA who smoked (n=9) were compared with smoking controls (n=40).

The relative number of lymphocytes is increased in bronchoalveolar lavage (BAL) fluid of patients with anticitrullinated protein antibodies (ACPA)-positive untreated early rheumatoid arthritis (RA). Graphs showing results from cell counts of lymphocytes (A) and macrophages (B) and expressed as percentage of total number of cells. *p<0.05.
BAL cells of ACPA-positive patients show a tendency towards a higher CD4:CD8 ratio as compared with controls (p=0.07). There were significantly more CD4+ BAL T cells expressing CD69 (p<0.001, figure 5A) and CD103 (p<0.05, figure 5B) and significantly reduced numbers of cells expressing CD25 (figure 5C), CD27 (figure 5D) and CXCR3 (figure 5E) (p<0.05 for all) in ACPA-positive, but not ACPA-negative, patients versus controls. FOXP3-positive BAL T cells did not differ between any of the groups. PAD2 was detectable by immunohistochemistry in 33% of the BAL samples obtained from ACPA-positive patients (6/17, 5 missing data), and only 17% of the BAL samples obtained from ACPA-negative patients (1/6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Markers of T-cell activation are increased in the bronchoalveolar lavage (BAL) fluid of patients with anticitrullinated protein antibodies (ACPA)-positive untreated early rheumatoid arthritis (RA). Graphs showing expression, as quantified by flow cytometry, of T-cell markers CD69 (A), CD103 (B), CD25 (C), CD27 (D) and CXCR3 (E) in BAL samples of ACPA-positive and ACPA-negative untreated early RA and healthy volunteers.
Discussion
Early inflammatory events in the lungs may represent a critical initiating factor in the development of ACPA-positive RA. In the current study, we identify novel histological traits supporting this hypothesis, demonstrating the presence of lymphoid aggregates and signs of immune activation in two different lung compartments of patients with early untreated ACPA-positive RA.
A major strength of our study is the unique study material consisting of bronchial biopsies and BAL of patients with early untreated RA with short symptom duration and no clinical signs of lung involvement. This material allows a detailed and sensitive characterisation of lung changes, even when these are not clinical and/or HRCT evident. Previous histological studies of RA lung biopsies have only included treated patients, with long disease duration and associated lung disease.12 ,22 ,23 Even though our study is the first of a kind, the low number of patients and even fewer numbers of ACPA-negative patients included are important limitations, impacting on the statistical strengths of some of our findings. The relative low percentage of patients agreeing to undergo bronchoscopy (21%) prevented further classification according to smoking status and potentially facilitated selection bias towards smokers. ACPA-positive patients were more often ever and current smokers compared with ACPA-negative patients. This might explain the higher, although not significant, degree of airflow limitation and lower DLCO in ACPA-positive patients as compared with ACPA-negative patients, in accordance with our previous report in a larger cohort of patients.8 However, ACPA has been previously associated with classic smoking-related disorders such as bronchiectasis independent of smoking status in patients with24 or without RA.25 ,26 In line with this, heavy smoking (defined as more than 10 pack-years) was equally present in both ACPA-positive and ACPA-negative RA groups. Also lymphocyte aggregates were detected in all biopsies of never-smoking patients with ACPA-positive RA, but absent from biopsies of healthy current smoker volunteers. Taken together, these data suggest that the observed lung changes are at least partly independent of smoking, in accordance with previous studies showing that increased citrullination in lungs (and other tissues)27–29 is related to a general increase in inflammation rather than to more tissue-specific events.
A central novel finding of our study is that lymphocytes (both B and T lymphocytes) are enriched and express increased activation markers in both bronchial biopsies and BAL samples of patients with ACPA-positive, but not ACPA-negative untreated early RA without associated lung diseases. Well-organised germinal centres were only observed in a minority of the samples, but when present, they did show features compatible with local production of ACPA (presence of plasma cells, postgerminal mature B cells and reactivity with citrullinated, but not arginine enolase peptide). Increased level of citrullinated proteins,8 paralleled by more frequent detection of PAD2 in bronchial biopsies of patients with ACPA-positive RA, is in agreement with previous observations.6 ,7 A larger number of patients and biopsies from several different anatomical segments would potentially increase the chance to identify mature germinal centres in more patients. Our findings are in agreement with previous identification of lymphoid aggregates and germinal centres in both patients with established RA and concomitant manifest lung disease12 and in ACPA-positive individuals with interstitial lung disease, but no RA.13
The presence of lung changes has previously been associated with longstanding seropositive and active disease in RA and thought to be a consequence of inflammation and secondary damage to the lungs,30 while no previous study to examine early untreated RA disease is currently available. The possibility that early changes (such as the ones described here) might also to a certain extent be due to a direct antibody-mediated injury and/or low-grade inflammation already before disease onset cannot be completely excluded. Isolation of ACPA-producing B cells from the lung compartment would be the final proof of local immune activation and antibody production, and this still remains to be done.
In conclusion, we have demonstrated signs of immune activation in BAL and bronchial biopsies of patients with early untreated ACPA-positive RA. This strengthens the hypothesis that the lung plays an important role in the immunological reactions responsible for the development of ACPA-positive RA, and warrants further functional and interventional studies to address this pathogenic link.
Acknowledgments
We thank Mikael Mikko, Benita Engvall, Gunnel de Forest, Heléne Blomqvist and Margitha Dahl for their excellent technical assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
Footnotes
Handling editor Tore K Kvien
Contributors All authors have made substantial contributions to (1) conception and design, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content and (3) final approval of the version to be published.
Funding This work was supported by research funding from the Swedish Foundation for Strategic Research, Innovative Medicine Initiative BTCure (115142-2), FP7-HEALTH-2012-INNOVATION-1 Euro-TEAM (305549-2), the Initial Training Networks 7th framework program Osteoimmune (289150), the Swedish Research Council, the Swedish Heart Lung Foundation, the Society for Rheumatology in Iceland and through the Regional Agreement on Medical Training and Clinical Research (ALF) between Stockholm County Council and Karolinska Institutet.
Competing interests None declared.
Ethics approval Regional Ethics Review Board in Stockholm.
Provenance and peer review Not commissioned; externally peer reviewed.