Article Text

Abstract
Objective Gout, the most common inflammatory arthritis, is associated with premature mortality. Whether this mortality gap has improved over time, as observed in rheumatoid arthritis (RA), is unknown.
Methods Using an electronic medical record database representative of the UK general population, we identified incident gout cases and controls between 1999 and 2014. The gout cohort was divided based on year of diagnosis into early (1999–2006) and late (2007–2014) cohorts. We compared the mortality rates and HRs, adjusting for potential confounders between the cohorts. We conducted sensitivity analyses among patients with gout who received at least one prescription for urate-lowering therapy, which has been found to have a validity of 90%.
Results In both cohorts, patients with gout showed similar levels of excess mortality compared with their corresponding comparison cohort (ie, 29.1 vs 23.5 deaths/1000 person-years and 23.0 vs 18.8 deaths/1000 person-years in the early and late cohorts, respectively). The corresponding mortality HRs were 1.25 (95% CI 1.21 to 1.30) and 1.24 (95% CI 1.20 to 1.29), and the multivariable HRs were 1.10 (95% CI 1.06 to 1.15) and 1.09 (95% CI 1.05 to 1.13), respectively (both p values for interaction >0.72). Our sensitivity analyses showed similar findings (both p values for interaction >0.88).
Conclusions This general population-based cohort study indicates that the level of premature mortality among patients with gout remains unimproved over the past 16 years, unlike RA during the same period. This unclosing premature mortality gap calls for improved management of gout and its comorbidities.
- Gout
- Epidemiology
- Arthritis
Statistics from Altmetric.com
Introduction
Gout is the most common form of inflammatory arthritis.1–3 In addition to causing severe pain and joint damage, gout is associated with cardiovascular-metabolic comorbidities and premature mortality.4–11 For example, in the Health Professionals Follow-Up Study, men with gout had a 28% higher risk of death from all causes,9 and a study of over 50 000 Singapore Chinese individuals found that patients with gout had an 18% increased risk of all-cause mortality.11
Meanwhile, rheumatoid arthritis (RA), another common inflammatory arthritis also associated with premature mortality, was found to have a substantially narrowed mortality gap in the premature death risk compared with the general population in recent years (likely owing to improvements in RA care), including our own study spanning 1999–2014.12 However, no equivalent secular trend data are available for gout. Given the well-documented suboptimal gout care, opposing mortality trends may exist between RA and gout, as was recently shown in their hospitalisation trends.13 We evaluated this hypothesis by examining mortality trends among patients with gout over the same period as in our recent study of RA (ie, 1999–2014) based on the same general population database.12 As mortality in the UK has improved substantially over the past decades,12 we incorporated these background mortality trends to assess excess mortality in patients with gout.
Methods
Data source
The Health Improvement Network (THIN) is an electronic medical record (EMR) database involving general practitioners (GPs) throughout the UK. It has health information on over 10 million patients from over 575 general practices in the UK. Health information is recorded at each site using a computerised system with several procedures to maintain sufficient data completion rates and accuracy. The information includes social and demographic variables, anthropometrics, lifestyle factors, details from GP visits, diagnoses from specialist referrals and inpatient admissions and results of laboratory tests. The READ classification system is used to code specific diagnoses14 and a drug dictionary using data from the Multilex classification system is used to code drugs.15 Approximately 95% of the UK population is registered with a general practice, and prior research has shown that THIN is representative of the UK population in terms of patient demographics and the prevalence of common illnesses.16
Study design and cohort definition
We conducted a matched cohort study to examine the secular trends of all-cause mortality among patients with incident gout compared with individuals with no gout. We identified all individuals between 18 and 89 years of age who had a first-ever diagnosis of gout defined by at least one READ code for gout between 1 January 1999 and 31 December 2014. The date of gout onset (ie, the index date) was defined as the date of the first diagnosis of gout. We considered incident cases as those who had an index date occurring at least 1 year after the date of entry into the study cohort.
In our alternative definition of gout, we identified all patients with a diagnosis of gout who were prescribed urate-lowering therapy (ULT) within 3 months after the diagnosis of gout. A similar case definition of gout has been shown to have a validity of 90% in the UK General Practice Research Database.17 To evaluate changes in mortality, we then divided the gout cohort into two calendar time-based cohorts according to each patient's year of diagnosis, forming the early (1999–2006) and late cohorts (2007–2014).
For the comparison cohorts corresponding to each gout cohort, we matched up to five individuals without gout based on age, sex and calendar year of entry (ie, the index year). If there were more than five non-gout matches available per subject with gout, we assigned each a random number and randomly selected five among these, whereas we selected all available non-gout matches in cases where there were fewer than five matches. The non-gout subjects were also required to have at least 1 year of continuous enrolment and to have at least one GP visit within the year prior to cohort entry.
Assessment of outcome
The outcome of this study was all-cause mortality, defined using the death date recorded in THIN. Registering of a death triggers an update in a national database, the Personal Demographics Service, which holds patient demographic data for the National Health Service. This change in patient status to ‘deceased’ immediately updates the patient's EMR. Previous studies have shown that the mortality data from THIN has high concordance with national death rates in the UK.16
Assessment of covariates
Using the THIN database, we obtained information prior to the index date on sociodemographic and anthropometric characteristics (ie, age, sex, birth date and body mass index (BMI)), lifestyle factors (ie, cigarette use and alcohol consumption), medication use (ie, diuretics and other antihypertensive agents, including angiotensin II receptor antagonists, ACE inhibitors, calcium channel blockers, β-blockers and low-dose aspirin) and comorbidities (ie, myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, chronic obstructive pulmonary disease, ulcer, liver disease, diabetes mellitus, renal disease, rheumatologic disease, cancer and AIDS). Based on comorbidities recorded by GPs, we calculated the adapted Charlson Comorbidity Index.18 All medication use was assessed starting 1 year prior to the index date, and sociodemographic and anthropometric characteristics were assessed using the most recent available data prior to the index date. Comorbidities were assessed any time prior to the index date. We assessed health service utilisation by assessing the number of GP visits in the year prior to the index date.
Statistical analysis
We compared the baseline characteristics of individuals in the gout cohorts and corresponding non-gout cohorts. Person-years of follow-up for each subject were calculated as the amount of time from the index date to the first of any of the following events: death, disenrolment from the THIN database or the end of the follow-up (either 31 December 2006 for the early cohort or 31 December 2014 for the late cohort, ensuring that the follow-up time was equal between the two cohorts to allow for a fair comparison). We then calculated all-cause mortality rates and plotted Kaplan-Meier mortality curves for each cohort.
We used a Cox proportional hazard model to examine the relation of gout to all-cause mortality for each time-specific gout cohort, adjusting for the number of GP visits, BMI, smoking status (ie, non-smokers, ex-smokers and current smokers), alcohol consumption (ie, non-drinkers, ex-drinkers and current drinkers), comorbidities and medication use. We also examined the difference in all-cause mortality between the gout cohorts and comparison cohorts using an additive hazard model in which the hazard was modelled as a linear function of gout status.19 The effect estimate generated from the model can be interpreted as the number of excess deaths attributable to gout per 1000 person-years. To evaluate whether the relationship between gout and all-cause mortality varied according to time, we combined the two gout cohorts and tested an interaction term (ie, gout status × calendar time-based cohort) in the multivariable regression model. Given the predilection of gout among men, we also analysed the mortality trends according to sex.
For all analyses, missing values for covariates (ie, BMI, alcohol consumption and smoking status) were imputed by a sequential regression method based on a set of covariates as predictors (IVEware for SAS, V.9.2; SAS Institute, Cary, North Carolina, USA).20
Results
The early cohort consisted of 44 783 incident patients with gout and 223 365 matched individuals with no gout. During the follow-up period, 3898 and 15 605 individuals died in the gout and non-gout cohorts, respectively. The median age at death was 79.0 and 79.4 years, respectively. In the late cohort of 58 478 incident patients with gout and 291 552 matched individuals with no gout, 4354 and 17 530 died during the follow-up period, with a median age at death of 79.8 and 80.1 years, respectively. The mean follow-up time in the two comparison cohorts was similar, with approximately 3 years of follow-up in the early cohorts and 3.2 years in the late cohorts.
As shown in table 1, there was no difference in age and sex between patients with gout and individuals with no gout in the early cohort at baseline. However, patients with gout were more likely to be current drinkers, less likely to be current smokers and more often used cardiovascular medications with more comorbidities than their matched controls. Similar findings were observed among subjects in the late cohorts.
Baseline characteristics of participants according to calendar time-based subcohorts and gout status
Figure 1 depicts the cumulative all-cause mortality during the follow-up among gout and non-gout cohorts. Patients with gout had higher mortality rates compared with individuals with no gout in both the early and late cohorts, and the magnitude of excess mortality was similar between the two cohorts. The age-matched, sex-matched and entry time-matched HR for all-cause mortality was 1.25 (95% CI 1.21 to 1.30) in the early cohorts as compared with 1.24 (95% CI 1.20 to 1.29) in the late cohorts (table 2), indicating that there was no improvement in the mortality gap between patients with gout and the general population over time (p for interaction=0.73). The multivariable-adjusted HR of all-cause mortality from gout also did not differ between the early (1.10, 95% CI 1.06 to 1.15) and late (1.09, 95% CI 1.05 to 1.13) cohorts (p for interaction=0.85) (table 2).
Association between gout and all-cause mortality according to time period
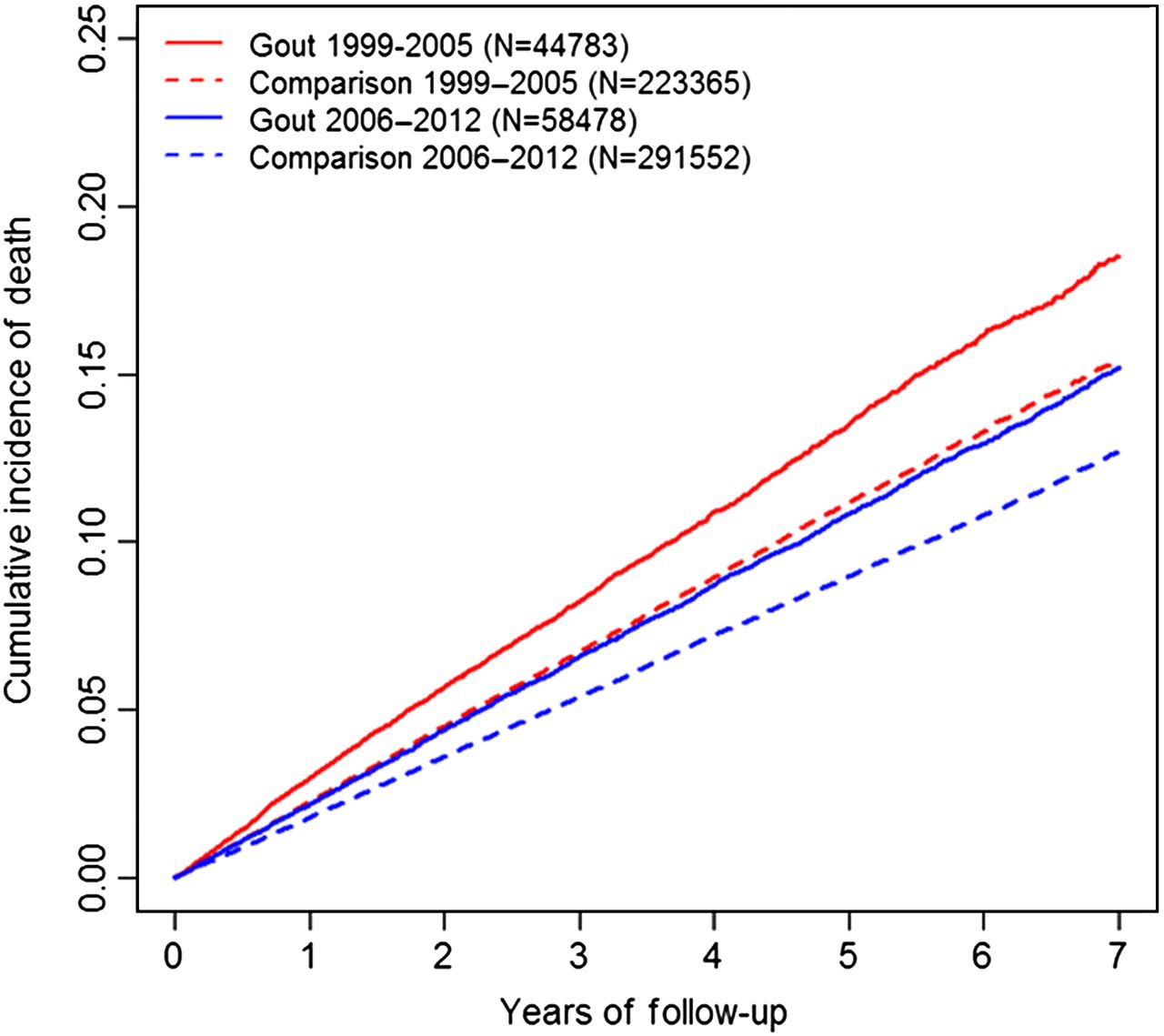
Cumulative mortality of patients with gout and corresponding individuals with no gout in the early versus late cohorts (1999–2006 vs 2007–2014, respectively).
The excess mortality rate between patients and matched controls before adjusting for covariates was slightly larger in the early cohorts than in the late cohorts (5.6 vs 4.1 deaths per 1000 person-years; p for interaction=0.03) (table 2). However, after adjusting for covariates, the corresponding multivariable-adjusted rate difference showed no significant difference (3.6 deaths per 1000 person-years in the early cohorts vs 3.2 per 1000 person-years in the late cohorts; p for interaction=0.51) (table 2).
When we repeated the analyses using our alternative definition of gout (ie, gout diagnosis plus ULT use), the results remained similar (figure 2 and table 3). The age-matched, sex-matched and entry time-matched rate ratio for all-cause mortality was 1.56 (95% CI 1.45 to 1.66) in the early cohorts as compared with 1.57 (95% CI 1.47 to 1.67) in the late cohorts, indicating no improvement in the mortality gap compared with the general population over time (p for interaction=0.89). After adjusting for covariates, the multivariable rate ratio did not differ significantly between the early and late cohorts (1.33; 95% CI 1.23 to 1.44 vs 1.32; 95% CI 1.22 to 1.43) (p for interaction=0.98). Similarly, the excess mortality rate between gout and matched controls did not differ significantly between the early and late cohorts (12.4 deaths per 1000 person-years (95% CI 10.1 to 14.6) vs 10.0 deaths per 1000 person-years (95% CI 8.2 to 11.7); p for interaction=0.10). The adjusted mortality rate difference also did not differ significantly between the two cohorts (9.6 deaths per 1000 person-years (95% CI 6.9 to 12.3) vs 7.4 deaths per 1000 person-years (95% CI 5.4 to 9.5); p for interaction=0.15).
Association between treated gout* and all-cause mortality according to time period

{kind=link}
{kind=link}
Cumulative mortality of patients with gout who received at least one prescription for urate-lowering therapy and corresponding individuals with no gout in the early versus late cohorts (1999–2006 vs 2007–2014, respectively).
Discussion
In this general population-based cohort study from 1999 to 2014, we found that the level of excess mortality among patients with gout remained unchanged. As such, the mortality trend among patients with gout over the past 16 years approximately paralleled that of the general population, leaving the premature mortality gap unimproved. This is in marked contrast to the aforementioned substantial reduction in excess mortality observed among patients with RA (likely due to improvements in RA care) during the same period in the same general population cohort.12 To our knowledge, this study is the first to investigate premature mortality trends in patients with gout over recent years, and our findings call for renewed attention and effort to improve and close the persisting mortality gap, as was achieved in RA.12
The unclosing mortality gap in gout may be related to the widely reported suboptimal gout care as well as its comorbidity management.21–29 For example, although the vast majority of patients with gout are indicated for a urate-lowering agent (eg, 87% within 5 years of diagnosis), only a small proportion receive treatment.25 Moreover, few patients receive a clear explanation about their gout and treatment expectations or appropriate lifestyle advice to reduce risk factors for gout and its associated comorbidities.30 ,31 These practices have led to poor medication adherence, with as few as 10% of patients with gout adhering to their treatment.32 Indeed, one study found adherence among patients with gout to be the worst among seven investigated chronic conditions.33 As a consequence, only a minority become free of gout, with the majority continuing to experience acute attacks, thereby contributing to an increased inpatient burden.28 ,34 which also contributes to many avoidable hospitalisations.13 ,35 ,36 A recent study based on the US national inpatient data found that primary hospitalisation rates for gout have increased substantially over the past two decades, whereas those for RA have declined considerably.13 Moreover, a recent abstract highlighted that up to 89% of hospitalisations with a primary diagnosis of gout were preventable, owing to inefficient or inadequate care.36
Proper urate control37 ,38 could have cardiovascular-metabolic-renal benefits39 ,40 via the hypothesised direct effect of lowering urate as well as reducing ongoing low-grade inflammation and the associated thrombogenic process.41 ,42 Furthermore, the prevention of gout flares by ULT could also have cardiovascular-metabolic-renal benefits via the reduced use of non-steroidal anti-inflammatory drugs and glucocorticoids that are often employed in ‘treat-to-symptom’ approaches.
Our excess mortality gap estimates of patients with gout using our primary definition (ie, 10% and 9% in the early and late cohorts, respectively) were comparable to those observed in the multiple risk factor intervention trial (MRFIT) study (9%) that defined gout using self-reported physician diagnosis of gout plus hyperuricemia8 and in another UK investigation using the same gout definition as the current study (13%).6 A Singapore Chinese Health Study that adopted self-reported physician diagnosis of gout with hyperuricemia or evidence of lifestyle intervention reported a slightly larger magnitude of association with all-cause mortality (18%).11 Finally, our estimates based on our secondary gout definition additionally requiring at least one prescription of ULT (33% and 32% in the early and late cohorts, respectively) were closer to those observed in the Health Professionals Follow-up Study that defined gout using the American College of Rheumatology preliminary criteria (28%).9 The larger mortality risk associated with our gout definition requiring ULT should be due to confounding by indication, as demonstrated in a previous analysis based on all (unmatched) allopurinol users compared with non-users.43 The same study also found that proper adjustment of potential confounders using propensity scores that incorporated the major imbalance of baseline serum uric acid (SUA) levels could overcome such confounding by indication and reveal the potential survival benefit of allopurinol in patients with gout.
Our study has several strengths and limitations. Our study is a general population-based cohort study; thus, our findings are likely to be generalisable. Unlike typical mortality trend study approaches that adjust only for age and sex to obtain standardised mortality ratios,44 ,45 we adjusted for potential key confounders prior to gout diagnosis (ie, obesity, smoking, comorbidities and medication use), thereby reducing a residual confounding effect. Furthermore, using incident gout cases minimises the selection bias that could underestimate the risk of death if prevalent gout cases were included in the analysis.46 However, uncertainty surrounding diagnostic accuracy is a potential concern in epidemiological studies such as ours. Nevertheless, the overall accuracy of using EMRs to assess important outcomes appears to be high as reflected in many validation studies.47 ,48 Furthermore, no other significant difference over the two periods was evident using our more specific alternative definition (ie, a physician-recorded diagnosis of gout plus at least one prescription of antigout medication, which has a positive predictive value of 90%).17 ,49 The mean duration of follow-up may appear short in each cohort; however, the aforementioned RA study during the same period in the same general population setting had a similar follow-up time in each cohort and showed a substantial mortality improvement. As such, the follow-up duration does not appear to be a reason for our finding. We did not have sufficient detail on the cause of death in a number of cases in our dataset, precluding investigations on the cause of death in this cohort. Nevertheless, the overall mortality trends are critically important in their own right, as all-cause mortality represents the overall net health outcome of various benefits and risks associated with disease management.50
In conclusion, this general population-based cohort study indicates that the survival of patients with gout has not improved over the past decade compared with the general population, unlike that of patients with RA during the same period.12 To that end, these data provide a key contrasting appraisal of the disease burden of gout and call for improved management of the disease and its comorbidities.
References
Footnotes
Handling editor Tore K Kvien
Contributors Study conception and design: MCF and HKC. Acquisition, analysis and interpretation of data: all authors. Drafting of the manuscript: all authors. Critical revision of the manuscript for important intellectual content: all authors.
Funding This project was supported in part by National Institutes of Health (NIH) grant P60-AR-047785 and NIH grant R01-AR-065944.
Competing interests HKC reports grants from AstraZeneca, consulting fees from Takeda and consulting fees from Selecta outside the submitted work.
Ethics approval The current study was approved by the Boston University Institutional Review Board and Multicenter Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.