Article Text

Abstract
Objectives To examine the incidence and temporal trends of psoriatic arthritis (PsA) in the general population in Denmark.
Methods Using nationwide registry data, we estimated the number of patients with incident PsA within each 1-year period between 1997 and 2011 and calculated the rate of PsA cases within gender and age subgroups. Incidence rates were presented per 100 000 person-years.
Results There was a female predominance ranging from 50.3% (1998) to 59.2% (2010), and the mean age at time of diagnosis was 47–50 years. We identified a total of 12 719 patients with PsA (prevalence=0.22%), including 9034 patients where the PsA diagnosis was made by a rheumatologist (prevalence=0.16%). Incidence rates of PsA (per 100 000 person-years) increased from 7.3 in 1997 to a peak incidence of 27.3 in 2010. Incidence rates were highest for women and patients aged 50–59 years, respectively. The use of systemic non-biologic agents, that is, methotrexate, leflunomide, ciclosporin or sulfasalazine increased over the 15-year study course and were used in 66.3% of all patients. Biologic agents (etanercept, infliximab, adalimumab, certolizumab pegol, golimumab or ustekinumab) were used in 17.7% of patients with PsA.
Conclusions We found a clear trend of rising PsA incidence on a national level. While the cause remains unclear, our findings might be explained by increased attention by patients and physicians.
- Psoriatic arthritis
- Incidence
- Prevalence
- Time trends
- Epidemiology
Statistics from Altmetric.com
Introduction
Psoriatic arthritis (PsA) is a chronic inflammatory musculoskeletal disease, which frequently develops in patients with cutaneous psoriasis.1 PsA is characterised by inflammation of the peripheral and axial joints as well as at the sites of tendon and ligament insertion into bone (enthesitis) and inflammation of the whole digit (dactylitis) and extra-articular manifestations, including nail dystrophy.2 3 Severity and prevalence of the different disease manifestations vary greatly, and the clinical picture may overlap with that of seronegative rheumatoid arthritis and ankylosing spondylitis.3
Although the prevalence of PsA is unclear, primarily due to lack of consensus on diagnostic criteria, it is estimated to occur in 0.04–0.1% of the general population; however, this figure may be underestimated.4 Studies have suggested that approximately 30% of patients with cutaneous psoriasis suffer from PsA, and one study reported that 42% of Danish patients with psoriasis had PsA when examined by rheumatologists, albeit that this may be limited to patients seen in a hospital setting.5 Although PsA may occur at any age, the onset typically begins in the patients mid-to-late 30s and affects men and women equally.2 3
Studies on the incidence of PsA in the general population remain scarce. While recent data suggest an incidence rate ranging from 3.6 to 7.2 per 100 000 person-years, older studies have reported a much wider incidence range (ie, from 0.1 to 23.1 per 100 000 person-years).6–10 The most recent study and the only prospective study of PsA in patients with psoriasis demonstrated an annual incidence of 2.8%.11 Consequently, the incidence and temporal trends of PsA in the general population remain poorly understood. In the present work, we therefore examined the incidence and prevalence of PsA in a Danish nationwide cohort.
Materials and methods
Data sources and study population
Study approval was obtained from the Danish Data Protection Agency (ref. 2007-58-0015, int. ref. GEH-2014–018, I-Suite 02 736) and approval from an ethics committee is not required for registry studies in Denmark. The study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology recommendations.12
Using the unique personal identification number assigned to all Danish citizens, we linked individual-level information from nationwide administrative registers. The Civil Registration System13 contains information on sex, date of birth and updated information on vital status and emigration, thus minimising loss to follow-up. All inpatient and outpatient (ambulatory) hospital consultations are recorded in the Danish National Patient Register14 (DNPR), including 1 primary and up to 19 secondary diagnoses coded by discharging physicians according to the International Classification of Diseases, eighth revision (ICD-8) (prior to 1994) and according to the tenth revision (ICD-10) thereafter. The primary diagnosis is the main reason for the hospital consultation or hospitalisation, and secondary diagnoses are additional conditions, including complications. Since 1994, detailed and accurate information on all pharmacy-dispensed medications has been registered in the Danish Registry of Medicinal Products Statistics according to the Anatomical Therapeutic Chemical classification.15 Hospital-administered pharmacotherapy is coded in the DNPR as treatment procedure (SKS) codes. We defined patients with incident PsA as those recorded with a corresponding first-time ICD-10 code (M07.0–3 and M09.0) and thus excluded all patients with a history of PsA before 1 January 1997. In estimations of prevalence, these patients were not excluded. The study period was divided into 1-year groups from 1997 to 2011. We identified the use of systemic therapy, that is, methotrexate, leflunomide, ciclosporin, sulfasalazine, etanercept, infliximab, adalimumab, certolizumab pegol, golimumab and ustekinumab. Although uncommon, methotrexate, sulfasalazine and ciclosporin can be prescribed by general practitioners in Denmark, whereas leflunomide and biologics are only prescribed by specialists. We did not consider corticosteroids, as these may be used primarily for short-term management and did not include non-steroidal anti-inflammatory drugs as these may also be purchased over the counter in Denmark.
Statistical analysis
We estimated the number of incident PsA cases within each of the predefined 1-year periods and calculated the frequency of PsA cases within gender and age subgroups (0–19, 20–29, 30–39, 40–49, 50–59, 60–69, 70+ years). We computed the incidence rate within each 1-year period as the number of newly diagnosed PsA cases divided by the risk time of the underlying population. We estimated the population size in each of the 1-year periods as the number of Danes alive in the mid-year of each period, as recorded in the Civil Registration System, and the risk time as 1 year times the estimated number of Danes in each period. The prevalence of PsA was estimated among all Danes alive and resident in the source population on 31 December 2012. Since it is possible that younger individuals may have been coded as having juvenile idiopathic arthritis (JIA) instead of PsA, we performed additional analyses to examine the incidence of having either PsA or JIA in individuals aged 0–19 years. Due to data security requirements, data on one or two subjects are shown as ‘less than 3’, and the derived percentages are not shown. SAS statistical software version 9.4 (SAS Institute, Cary, North Carolina, USA) was used for statistical analysis.
Results
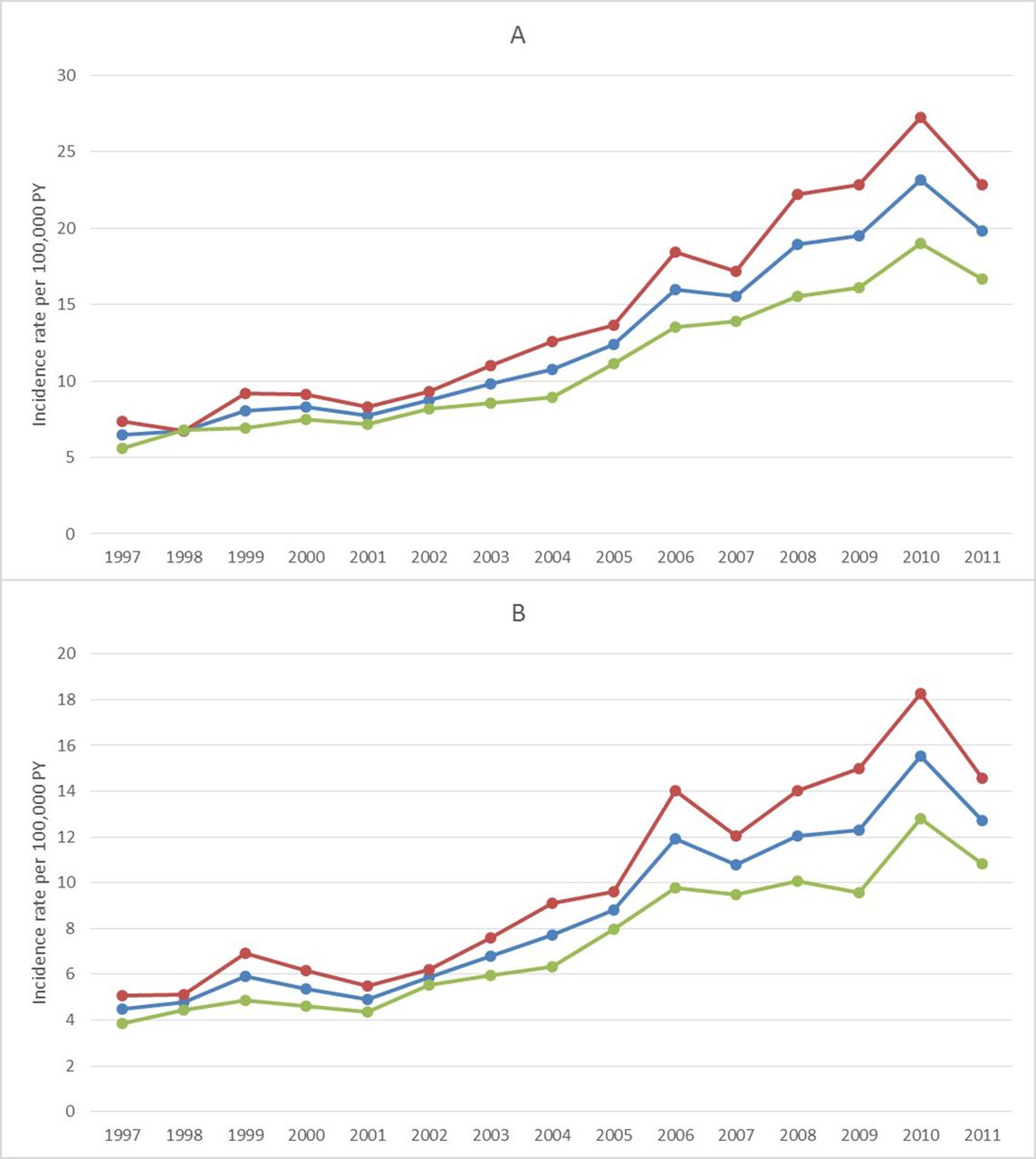
During the study period, the total Danish population comprised approximately 5.7 million individuals with equal gender distribution. Among patients diagnosed with PsA, there was a female predominance ranging from 50.3% (1998) to 59.2% (2010), and the mean age at time of diagnosis was 47–50 years (table 1 and see online Supplementary table S1). The incidence of PsA (presented as incidence rates per 100 000 person-years) increased almost fourfold, from 7.3 in 1997 to a maximum of 27.3 in 2010 (see online Supplementary Table S2 and figure 1). The highest percentage of patients with incident PsA was among individuals aged between 50 and 59 years, whereas PsA was the least frequent among younger individuals aged 0–19 years (table 1 and figure 2). Similarly, age-specific incidence rates revealed the greatest absolute increase in PsA incidence among subjects aged 50–59 years and the lowest increase among individuals aged 0–19 years (see online Supplementary table S2 and supplementary figure S1).

Incidence rates of psoriatic arthritis (PsA). Total and gender-specific incidence rates per 100 000 person-years of PsA over the study period 1997–2011. (A) Diagnoses from all specialties. (B) Diagnoses made by rheumatologists. Blue,Overall; Red, Women; Green, Men.

Age-specific incidence rates per 100 000 person-years of psoriatic arthritis over the study period 1997–2011.
Characteristics of patients diagnosed with first-time psoriatic arthritis (PsA) in Denmark, all specialties
The use of systemic non-biologic agents, that is, methotrexate, leflunomide, ciclosporin or sulfasalazine increased over the 15-year study course. The first recorded use of biologic agents (etanercept, infliximab, adalimumab, certolizumab pegol, golimumab or ustekinumab) for patients diagnosed with PsA within the same year occurred in 2004 from whereon their use steadily increased (table 1 and see online supplementary table S1).
As shown in table 2, we identified a total of 12 719 patients with PsA (prevalence=0.22%), including 9034 patients where the PsA diagnosis was made by a rheumatologist (prevalence=0.16%). When limited to adults (≥18 years), the PsA prevalence was 0.28% across specialties and 0.20% when the diagnosis was made by a rheumatologist. Among patients not diagnosed by a rheumatologist, the majority received their diagnosis from a dermatologist. Patients were predominantly women (58%) with a mean age of 47 years. The highest prevalence was among patients aged between 50 and 59 years, followed by those aged 60–69 years (table 2 and figure 3). Approximately two-thirds of patients had received treatment with systemic non-biologic agents, whereas biologics were used in one-fifth of patients (table 2). Similar characteristics were observed when analyses were limited to patients diagnosed by a rheumatologist (see online Supplementary figures S2-3). The trend in incidence of PsA and JIA combined for individuals aged 0–19 years are shown in online Supplementary figure S4.

{kind=link}
{kind=link}
{kind=link}
Distribution of prevalent psoriatic arthritis, stratified by age.
Characteristics and prevalence of patients diagnosed with psoriatic arthritis (PsA)
Discussion
In this nationwide study of the Danish population, we observed an increasing incidence of PsA between 1997 and 2011. This finding is in contrast to cutaneous psoriasis which appears to have a stable or even slightly decreasing incidence in Northern Europe.16 Notably, the increasing incidence was most pronounced among older individuals, and a strong female predominance was observed. Overall, the prevalence of PsA in Denmark was 0.22%, whereas the prevalence was 0.16% when limited to diagnoses made by rheumatologists. Two-thirds of patients received treatment with systemic non-biologic therapy, and one-fifth of patients were at some point treated with biologics.
While the aim of the present study was to examine the incidence and prevalence of PsA in the general population, studies have reported that most patients with PsA develop cutaneous psoriasis prior to the development of arthritic symptoms.17 18 Notably, however, data suggest that the risk of PsA remains constant following diagnosis of cutaneous psoriasis.19 Several studies have examined the incidence and prevalence of PsA in patients with cutaneous psoriasis, yet general population studies of PsA incidence remain conflicting, although a recent meta-analysis reported a PsA prevalence of 0.19% in Europe.20 Based on self-reported questionnaire data from 2006 to 2008, a Norwegian study of 50 806 citizens found a PsA incidence rate of 41.3 per 100 000 person-years and a prevalence of 0.67% among individuals older than 20 years.21 In one previous study from Denmark, 34 944 Danish twins were surveyed in 2002, and reported an incidence rate of 6 per 100 000 person-years.22 The observed differences between previous studies and our findings may be due to methodological differences, as well as the time period in which the incidence and prevalence was examined. A fundamental limitation of the aforementioned studies is the lacking assessment of the developments in PsA incidence over time. However, one small study comprising a total of 147 patients with incident PsA reported an increasing incidence from 3.6 to 9.8 per 100 000 person-years between the periods from 1970–1979 to 1990–1999.23 Similarly, a study from Taiwan reported an increasing PsA prevalence from 1014 in 2003 (prevalence rate: 0.45/10 000 individuals) to 3072 in 2013 (prevalence rate: 1.31/10 000 individuals).24 Until now, only one prospective study has been published of patients with psoriasis developing PsA. The study reported a constant risk in these patients.11 Indeed, this finding was corroborated by a cross-sectional observational study of 1560 patients with psoriasis, of which 126 had PsA.19
We found a mean age of 47–50 years at time of PsA diagnosis, a somewhat higher estimate compared with certain other studies.25 Our population-based study also included cases diagnosed by dermatologists only, which together with milder more insidious cases of onset could explain the higher mean age of diagnosis identified in this study. The female predominance observed in our study is supported by some previous publications, including data from biologics registers.20 21 26 Although the cause remains speculative, it is conceivable that female patients may be more likely to seek medical treatment for arthritic symptoms compared with men. The increasing PsA incidence is in contrast to rheumatoid arthritis, for example, where recent population-based studies have reported a reduction in incidence and prevalence.27 Although speculative, decreasing number of active smokers together with less air pollution in the major cities over the last decades, together with an increase in obesity may explain these differences. Moreover, we observed an increase in use of systemic therapies, in particular biologics, in newly diagnosed patients with PsA. It is plausible that the increasing PsA incidence may reflect use of screening questionnaires as well as increased targeted educational initiatives provided to patients and physicians. The increasing use of systemic therapies may also be due to emerging data suggesting that early and aggressive treatment results in improved prognosis,28 29 and the introduction of the classification criteria for psoriatic arthritis (CASPAR) criteria which may have enabled increased focus on specific symptoms, consequently resulting in earlier disease recognition. However, in daily practice few clinicians use the CASPAR criteria outside of clinical trials and computerised databases. Also, the lack of evidence supporting the use of synthetic disease-modifying antirheumatic drugs may have influenced the use of biologics. For example, studies have suggested that methotrexate does not significantly modify relevant disease outcome measures in PsA,30 whereas a tight control of disease activity was recently shown to significantly improve PsA.31
Strengths and limitations
Because of its nationwide and population-based design within a setting with equal access to healthcare for the entire population, our study is virtually unaffected by referral and selection biases and is likely to provide highly generalisable results. Nonetheless, a few limitations need to be addressed. Although we find it unlikely that misclassification can explain our findings, we acknowledge that an increase in the completeness of PsA coding over time might play a role in the observed increase in PsA incidence. The ICD-10 classification has been used in Denmark since 1995. Selection of patients with PsA in this study was based on ICD codes recorded, which may introduce a selection bias towards more severe cases being included while failing to capture patients with mild disease who are managed entirely at primary care units. However, according to a previous study in Sweden (a neighbouring Scandinavian country closely resembling Denmark), this is a minor problem and would only increase the number of cases by less than 4%, at the expense of a larger degree of misclassification.32
Regarding the case definitions of PsA used in this study, data and results from another group suggest that rheumatic misclassification occurs in less than 10%.33 Moreover, our findings were corroborated by analyses limited to diagnoses given by rheumatologists, which yielded similar results as our primary analyses. Nevertheless, we cannot refute that our results may be underestimated. Indeed, a recent meta-analysis found that up to 15.5% of patients with cutaneous psoriasis may have undiagnosed PsA.34 Since we dealt with confounding by age and gender in stratified analyses, we find it unlikely that confounding plays a substantial role in our findings of an increase in PsA incidence over time. We lacked data on clinical measures of disease severity and used systemic treatment as a measure thereof, which may have biased our results slightly. Lastly, our study was limited by the lack of information on clinical as well as radiographic findings among patients with PsA and we were therefore unable to evaluate the impact of the systemic treatment, for example, on time trends of disease severity and progression.
In conclusion, we found a clear trend of rising PsA incidence on a national level in Denmark. While the cause remains unclear, it is likely that our findings are partly explained by increased attention by patients and physicians, the availability of classification criteria, increased information on disease severity and a need for earlier therapy. Future research is warranted to examine whether early and aggressive treatment of cutaneous psoriasis, for example, with systemic agents such as biologics, may prevent a continuous increase in PsA incidence.
References
Footnotes
Contributors AE and GHG had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: AE. Acquisition, analysis and interpretation of data: all authors. Drafting of the manuscript: AE. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis: AE and GHG. Obtained funding: AE and LM. Administrative, technical or material support: AE and GHG. Study supervision: AE and GHG.
Disclaimer Eli Lilly and Company, the funding source, participated in interpretation of the final analysed study results, but had no access to the raw data and did not participate in data collection, management or analysis.
Competing interests AE has received research funding from Pfizer and Eli Lilly and honoraria as consultant and/or speaker from Pfizer, Eli Lilly, Novartis, Galderma and Janssen Pharmaceuticals. LEK has received fees for speaking and consultancy from Pfizer, MSD, AbbVie, UCB, Eli Lilly, Novartis, Celgene, Janssen Pharmaceuticals, Roche, Forward Pharma and BMS. JPT is supported by an unrestricted grant from the Lundbeck Foundation and has received speaker honoraria from Galderma and MEDA. GHG is supported by an unrestricted research scholarship from the Novo Nordisk Foundation. ABG has received honoraria as consultant and/or speaker from Amgen Inc.; Astellas, Akros, Centocor (Janssen), Inc.; Celgene Corp., Bristol Myers Squibb Co., Beiersdorf, Inc., Abbott Labs. (Abbvie), TEVA, Actelion, UCB, Novo Nordisk, Novartis, Dermipsor Ltd, Incyte, Pfizer, Canfite, Lilly, Coronado, Vertex, Karyopharm, CSL Behring Biotherapies for Life, Glaxo Smith Kline, Xenoport, Catabasis, Meiji Seika Pharma Co., Ltd, Takeda, Mitsubishi, Tanabe Pharma Development America, Inc., Genentech, Baxalta, Kineta One, KPI Therapeutics, Crescendo Bioscience, Aclaris, Amicus and Reddy Labs and received research funding (paid to Tuft Medical Center) from Centocor (Janssen), Amgen, Abbott (Abbvie), Novartis, Celgene, Pfizer, Lilly, Levia, Merck, Xenoport, Dermira and Baxalta. LCC has reported no conflicts of interest. DJ has received research funding from Pfizer and honoraria as consultant and/or speaker from Abbvie, Amgen, Celgene, Eli Lilly, Janssen Pharmaceuticals, MSD, Novartis and Pfizer. PG has received honoraria as consultant and/or speaker from AbbVie, Celgene, Eli Lilly, Janssen, Leo Pharma, MSD, Novartis, Pfizer and UCB. DDG has received consultancy fees and/or grant support from AbbVie, Amgen, BMS, Celgene, Eli Lilly, Janssen, Pfizer, Novartis and UCB. LS has received consultancy and/or speaker honoraria from Abbvie, Pfizer, Janssen-Cilag, Merck Sharp & Dohme and Leo Pharma and is a member of the advisory boards of Abbvie, Pfizer, Leo Pharma, Janssen-Cilag, Merck Sharp & Dohme, Eli Lilly, Celgene and Novartis. LM is currently employed by Eli Lilly and Company.
Patient consent Patient consent is not required for register studies per Danish law.
Provenance and peer review Not commissioned; externally peer reviewed.