Article Text

Abstract
Objectives Tumour necrosis factor-α inhibitor (TNFi) treatment has been shown to reduce the rates of anterior uveitis (AU) in patients with ankylosing spondylitis (AS). Our objective was to compare the effect of adalimumab (ADA), etanercept (ETN) and infliximab (IFX) on AU occurrence in AS, using real-world data.
Methods Patients with AS starting ADA, ETN or IFX as their first TNFi from January 2003 to December 2010 were extracted from the Swedish Rheumatology Quality Register. AU rates, based on visits to an ophthalmologist with International Classification of Diseases 10 codes for AU, were obtained by linkage to the Swedish National Patient Register. For each TNFi, AU rates 2 years before TNFi start and for the first 2 years on TNFi treatment were compared. In the subgroup of patients who were AU-free during the 2 years before TNFi start, we also compared the risk of a first AU event.
Results 1365 patients with AS were included (406 ADA, 354 ETN, 605 IFX). Compared with pretreatment rates, we noted a reduction in overall AU rates for ADA and IFX, and an increase for ETN. The adjusted HRs for AU in 1127 patients who were free of AU in the last 2 years before TNFi start were significantly higher for ETN versus ADA (HR: 3.86 95% CI 1.85 to 8.06) and ETN versus IFX (HR: 1.99, 95% CI 1.23 to 3.22), while the HR for IFX versus ADA was not statistically significant.
Conclusions The results suggest differences in effect on AU risk between ADA, ETN and IFX, with a clear advantage for ADA/IFX over ETN.
- Ankylosing Spondylitis
- Anti-TNF
- Treatment
Statistics from Altmetric.com
Introduction
Anterior uveitis (AU) is the most common extra-articular manifestation in ankylosing spondylitis (AS), with a recent meta-analysis describing a cumulative incidence of around one in four patients.1 While AU sometimes precede the onset of axial symptoms,2 a recent study also showed that the cumulative incidence of acute AU continues to increase for many years after the time-point of AS diagnosis.3
In AS, the visual prognosis after acute AU is excellent with adequate treatment, which usually includes topical (and at times oral and locally injected) corticosteroids.4 Observational studies have suggested that sulfasalazine (SSZ) may prevent recurrence of AU in patients with AS5 ,6 and some positive data also exist for methotrexate (MTX)7 and non-steroidal anti-inflammatory drugs (NSAID).8 Treatment with tumour necrosis factor-α inhibitors (TNFi) has also repeatedly been shown to reduce the occurrence of AU in patients with AS,9–11 with reports including both reduced rates compared with placebo-treated patients,10 ,12 ,13 and compared with rates pre-TNFi-treatment.11 ,14 One randomised controlled trial has also demonstrated effectiveness of adalimumab (ADA) against a variety of different types of intermediate and posterior uveitis.15
Observational studies have suggested that the soluble TNF receptor fusion protein etanercept (ETN) may be less effective in preventing AU, compared with the monoclonal TNF antibodies infliximab (IFX) and ADA.16–18 However, the previous studies have been heterogeneous in both design and in reporting of data, and two meta-analyses incorporating observational studies and randomised controlled trials (RCT) have reported conflicting results.10 ,19 Additional data are thus needed to elucidate whether TNFi have differential effects with regard to preventing AU.
The aim of this study was therefore to compare AU rates in patients with AS during ADA, ETN or IFX treatment.
Methods
Data sources and patients
Our study is based on data from the Swedish Rheumatology Quality Register (SRQ), the Swedish National Patient Register (NPR) and the Swedish Population Register.
The SRQ was established in 1995 and is integrated into clinical practice.20 The patients are registered in the SRQ with their clinical diagnoses, as determined by the treating rheumatologist, and disease activity and treatment is registered at initiation of biological disease-modifying antirheumatic drugs (DMARDs) and at regular follow-up visits. The SRQ coverage for patients with spondyloarthritis treated with TNFi has recently been estimated to be 86%.21
The NPR is kept by the National Board of Health and Welfare, and was started in 1964 as a hospitalisation register. Complete national coverage for inpatient care was reached in 1987, and since 2001 the register also includes specialised outpatient care.22 The Swedish Population Register contains demographic and socioeconomic data on all residents in Sweden.23
We included patients registered with a diagnosis of AS in SRQ and who started treatment with ADA, ETN or IFX as their first TNFi from January 2003 through December 2010. January 2003 was chosen as the starting point to allow for at least 2 years of pretreatment outpatient care data in the NPR.
From SRQ covariate data were retrieved on age, sex, start year for TNFi, disease duration at initiation of TNFi and baseline data (at the time-point of starting the first TNFi) on C reactive protein (CRP) and comedication with conventional synthetic DMARD (csDMARD), prednisolone and NSAID. Follow-up data through December 2011 were available at the time of analysis. Covariate data on a history of inflammatory bowel disease (IBD) and psoriasis were retrieved from the NPR and data on level of education was provided by the Population Register.
AU events were based on outpatient visits in ophthalmological specialist care with associated International Classification of Diseases (ICD-10) codes for AU (ICD-10: H20 and H22.1) extracted from the NPR. AU codes associated with outpatient visits to other specialists (eg, rheumatology, internal medicine) were disregarded. AU data were available from 1 January 2001 (start of the outpatient register). End of follow-up was set to 31 December 2011. All patients had at least 2 years (range: 2–10 years) of aggregated data in the registers before start of TNFi treatment.
Baseline characteristics and descriptive data
Demographics and baseline characteristics were compared across TNFi type (ADA vs ETN vs IFX). The proportion of patients in each TNFi group contributing AU events for different periods of time before TNFi start, and during TNFi treatment, were also described, primarily in order to assess possible channelling effects. Furthermore, the number of subjects in whom AU visits occurred before TNFi start was cross-tabulated with the number of subjects with AU visits during TNFi treatment, in order to assess to what extent the AU events after treatment initiation were new-onset AU, or occurred in subjects with previous AU.
Outcome, follow-up and main analyses
Three definitions of AU flare were analysed: (a) the total number of AU visits before and on TNFi treatment, (b) AU flare defined by a 60-day penalty from the index visit of one AU flare for a new flare to be counted (flare definition 1) and (c) AU flare defined by a >90-day gap between visits (flare definition 2). See online supplementary figure S1 for an illustration of the flare definitions.
supplementary figure
An illustration of the different definitions used for a flare of anterior uveitis.
Two main analytical approaches were applied to compare the three TNFi. First, we compared AU rates before TNFi start and during TNFi treatment, for each TNFi. In this analysis, the AU rates per 100 patient-years during the 2 last years prior to TNFi start were compared with the AU rates per 100 patient-years during the first 2 years on TNFi treatment. Only cases with at least 2 years of possible on-treatment observation time were included, thus only including patients starting with TNFi up until 31 December 2009. The on-treatment rates were based on observation time at risk, hence censoring patients either at the time-point of 2 years on-treatment, discontinuation of treatment, death or migration, whichever occurred first.
Second, we compared the hazard of the first on-treatment AU after start of treatment, within the subgroup of patients who had no diagnosis of AU during the 2 years before TNFi start. The rationale for the 2-year AU-free interval was: (1) to minimise channelling bias due to a lower pretreatment rate of AU in any of the three TNFi groups, (2) this was the minimal available pretreatment observation period, if calendar years for the three TNFi compared were to overlap (ADA was approved in 2003, 2 years after our period of data collection started).
Sensitivity analyses and stratification
Two sets of sensitivity analyses were performed regarding the AU rates. First, we calculated AU rates (as described in the previous section) using all available person time before and after treatment start (and thus not restricting it to a 2-year time frame before and after treatment start). In this analysis, cases were also censored at discontinuation of treatment, death or migration or 31 December 2011. Second, we calculated incidence rates for AU as described in the main analysis, but stratified by the presence or absence of AU during the 2 years before TNFi start. A third sensitivity analysis was performed regarding the hazard of first on-treatment AU, only including patients without csDMARD therapy at baseline.
Statistics
Baseline data are presented as frequencies with percentages, means with SDs and/or medians with 25 and 75 percentiles, depending on the type of data and the distribution. Demographics and baseline characteristics were compared across TNFi type by χ2 test, analysis of variance and Kruskal-Wallis test as appropriate; 95% CIs for AU rates were determined through Poisson regression.
HRs with 95% CI, for a first AU flare, were determined through Cox proportional hazard regression analyses, both unadjusted and adjusted for age, sex, start year for TNFi, disease duration at initiation of TNFi, history of IBD and baseline CRP, csDMARD comedication, prednisolone and NSAID. Due to a high proportion of missing data for CRP (22.7%), this variable was categorised as <10 mg/L, ≥10 mg/L and ‘missing’.
We used IBM SPSS Statistics V.21 and SAS V.9.3 for the analyses.
Results
Patients
The study included 1365 patients with AS starting treatment with ADA (N=406), ETN (N=354) or IFX (N=605) as their first TNFi. At baseline for TNFi start, the proportion using csDMARD was significantly higher in the IFX group (55.4% vs 28.1% and 30.5% for ADA and ETN, respectively) (table 1). The most frequently used csDMARD was MTX (ADA 13.5%, ETN 19.2% and IFX 44.0%), but SSZ was also slightly more frequently used in ADA (11.1%) compared with ETN (7.3%) and IFX (6.1%), the difference only being of statistical significance for ADA compared with IFX (p=0.04). Baseline erythrocyte sedimentation rate and CRP were lower in patients treated with ADA, and ADA was more commonly used in the second half of the period, that is, 2007–2010 (ADA was approved in Sweden 2003). The level of education was also lower for the IFX-treated patients (table 1).
Demographics and baseline characteristics across TNFi
Proportions of patients with AU before and during TNFi treatment
The proportions of patients with a registered AU visit before TNFi start were remarkably stable, regardless of having >2, >4 or >6 years of before-treatment observation time (22.9%–28.1%), but as expected lower when only including the last 2 years prior to TNFi start (16.4%–19.2%) (table 2). However, the relative proportion of patients with a history of AU before TNFi start, in the three TNFi groups, remained the same irrespective of the chosen time window, justifying the use of a 2-year pretreatment observation time period in the main analyses. Furthermore, the proportion contributing an AU visit prior to treatment was consistently the highest in the ADA group, followed by IFX and then ETN, suggesting channelling of treatment initiation towards ADA and IFX in patients with a history of AU.
Number and proportion of patients contributing with AU visits, before start of TNFi, during the first 2 years of follow-up and during the total follow-up
On-treatment, the proportion with AU was the lowest among patients treated with ADA and the highest among patients treated with ETN (table 2), and the pattern was similar for the first 2 years on treatment and the overall observed data.
Table 3 shows the relationship between AU before TNFi start versus on-treatment. Among patients treated with ADA, ETN and IFX, who had an AU visit after treatment start, 80.6%, 54.3% and 69.6%, respectively, also had an AU visit registered prior to TNFi start. Conversely, from table 3 it is also evident that the proportion with possible ‘de novo’ AU (ie, no AU events registered pretreatment in the available data from 1 January 2001) varied considerably between groups: 13.7% (37 of 270) for ETN, 5.3% (24 of 454) for IFX and 2.1% (6 of 286) for ADA.
Relationship between AU occurrence before TNFi start and on drug
AU rates during the 2 years prior to TNFi start and the first 2 years on treatment
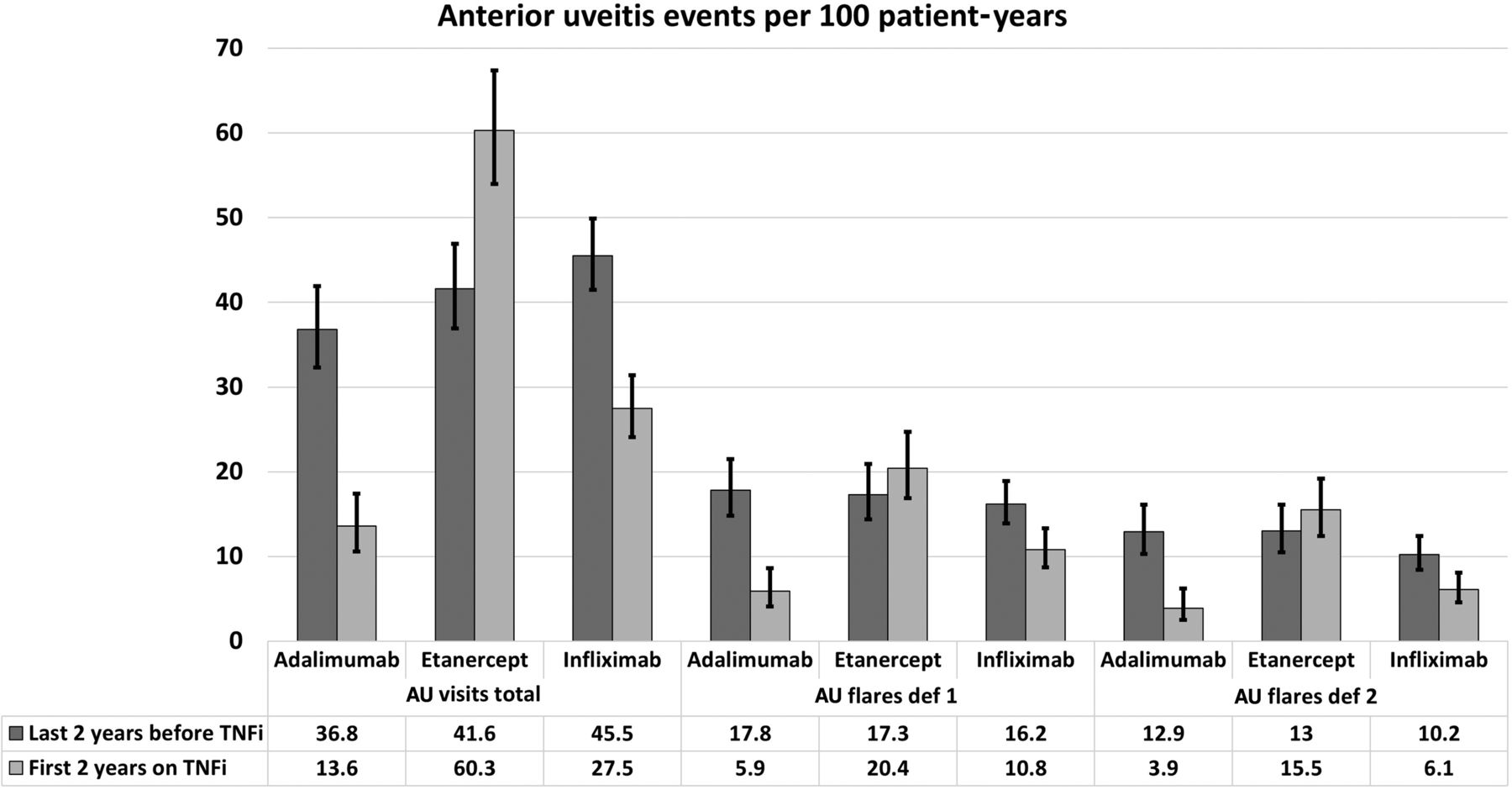
The number of events per 100 patient-years during the last 2 years prior to TNFi start was similar for ADA, IFX and ETN, with overlapping 95% CI (figure 1). However, the AU rates during the first 2 years on-treatment differed considerably, with the lowest rates for ADA and the highest for ETN. The two alternative flare definitions (definitions 1 and 2) as expected resulted in lower rates, compared with the total AU visit rates, but with an otherwise similar trend of increased rates of AU after initiating ETN, and decreased rates for ADA and IFX (figure 1), compared with the pretreatment rates.

{kind=link}
Anterior uveitis (AU) event rates during the 2 years prior to treatment with tumour necrosis factor-α inhibitors (TNFi) and during the first 2 years on treatment, according to number of visits with a diagnosis of AU and two definitions of AU flare, for adalimumab, etanercept and infliximab. The on-treatment rates are based on observation time ‘at risk’, censoring patients at either 2 years on treatment, death, discontinuation of treatment or migration, whichever occurred first.
Hazard of AU during TNFi treatment
In the adjusted Cox regression analysis, among patients who were uveitis-free during the 2 years before TNFi start, ETN was associated with higher hazard than ADA (HR 3.86, 95% CI 1.85 to 8.06) and IFX (HR 1.99, 95% CI 1.23 to 3.22), while there was no statistically significant difference between ADA and IFX (table 4). The HRs were similar in the unadjusted analysis (table 4).
Cox regression analyses of time to first AU flare after start of TNFi during the first 2 years of therapy among those without any AU visit (to ophthalmologist) within 2 years prior to start
Sensitivity analyses and stratification
In the sensitivity analysis analysing the AU rates based on all available observed person time at risk, before and on TNFi treatment (table 5a), the rates were generally lower during the pretreatment period, compared with the main analyses restricted to ±2 years, (range 23.1–31.7 vs 36.8–45.5), but similar or slightly higher on-treatment (range 15.7–55.2 vs 13.6–60.3).
Sensitivity analyses showing rates for visits and flares of AU: (a) including all observed person time at risk prior and after start of first TNFi and thus without restriction to a 2-year period, (b) among those having a recorded visit with AU within 2 years prior to start of follow-up and (c) among those without having a recorded visit with AU within 2 years prior to start of follow-up
In the analysis stratifying the main analysis on cases with AU and cases without AU in the 2 years prior to TNF, the on-treatment AU rates were, as expected, higher in the former group (table 5b) compared with the latter (table 5c).
Among those treated with ETN, without an AU event in the 2 years prior to treatment start (table 5c), the on-treatment rates were similar to the pretreatment rates overall for the ETN group (table 5a), possibly suggesting a lack of protective effect of ETN on AU flares. Furthermore, the CIs for the AU rates, in the group without a prior AU event in the 2 years prior to treatment start (table 5c), were non-overlapping between ADA versus ETN and IFX versus ETN, but not for ADA versus IFX, also supporting a significant difference between ETN and the monoclonal TNFi.
In the sensitivity analysis regarding hazard of first on-treatment AU, including only those without csDMARD at baseline, the HRs were slightly lower, but comparable to the HR in the whole population: HR (95% CI) ETN versus ADA 2.82 (1.28 to 6.26); IFX versus ADA 1.66 (0.70–3.93) and ETN versus IFX 1.70 (0.90–3.19).
Discussion
We found a fourfold increase in the risk for AU, during the first 2 years after treatment start, for patients with AS starting treatment with ETN compared with ADA, and a twofold increase for ETN compared with IFX, but no statistical difference between ADA and IFX. Compared with the rates pretreatment, the AU rates increased when initiating treatment with ETN, but decreased when starting ADA or IFX.
That monoclonal TNF antibodies may protect against AU flares more effectively than the soluble TNF receptor ETN, has been reported previously in one meta-analysis,10 two retrospective observational studies of different designs16 ,18 and one observational study based on a US claims database.17 In addition, data derived from adverse drugs events reporting (not including cases with AS) have supported this finding.24 In contrast, a recent meta-analysis, based on eight RCT of TNFi in AS, reported a contradictory finding, where ETN appeared to be more effective against uveitis than the monoclonal therapies.19 However, in this latter meta-analysis, none of the RCTs included was designed to specifically investigate the effect of TNFi on AU, and the numbers of AU events were small, which may explain the discrepant results. The findings of our study are in line with the study based on US claims data,17 although we found an even larger difference between ETN and ADA than the US claims study (HR 3.86 vs 1.91).17 The biological explanation for the differences in AU rates between monoclonal TNF antibodies and ETN is unclear, and suggested mechanisms include both a differential protective effect and the possibility of a paradoxical AU induction by ETN,17 but it should also be noted that previous studies have indicated that ETN still reduces the number of AU flares more effectively than placebo.12
In this study, the decrease in AU rates was in favour of ADA compared with IFX, but the CIs for the HR did not indicate a statistically significant difference. Similar trends have been observed previously,17 but it should be stressed that the IFX doses in the current study tended to be lower than the labelled dose in AS, which is 5 mg/kg. The comparative effect of ADA versus IFX should therefore be interpreted with caution. At baseline 50% used ≤200 mg IFX, and at the last registration 62% used ≤200 mg. Furthermore, changes in the doses of IFX, ADA and ETN, or changes in csDMARD during follow-up were not adjusted for in this study. In a previous publication of the same patient group, we have shown that changes in csDMARD therapy occurred in only 16% during follow-up.25 Nevertheless, since concomitant csDMARD therapy is often used as comedication in conjunction with TNFi treatment of AS in Sweden, it cannot be ruled out that the observed differences in baseline csDMARD therapy between the TNFi groups could affect the results. However, the sensitivity analysis excluding those on csDMARD at baseline resulted in similar HR as the main results, which further support the validity of the results.
A number of limitations of this study must be recognised. First, the AU flares are identified based on registered diagnoses at a visit to an ophthalmologist, with no information on whether each visit was for a new AU flare, a follow-up visit linked to a previous flare, or to AU of more chronic nature. According to uveitis nomenclature, AU flares are categorised as limited if the duration is <3 months and persistent if >3 months.26 Two alternative flare definitions were included, but these definitions are imperfect, since for example a persistent AU in one eye cannot be distinguished from a new flare in the contralateral eye, or unilateral versus bilateral AU. However, this limitation, as well as other misclassification and missing data in the registers, ought to be non-differential for the three TNFi, and therefore rather reduce the chances to detect differences between the TNFi. Second, there is an obvious risk for channelling bias, if ETN is less likely to be initiated in a patient with a history of AU (as supported by table 2), but it is also unlikely that this bias would alter the direction of the results. However, it cannot be determined from the register data to what extent the indication for TNFi treatment was in fact AU, or other manifestations of AS disease activity. Third, only including patients without AU 2 years prior to TNFi in the Cox regression, will result in a group that is less prone to develop AU flares. The effect of this restriction should also be non-differential between TNFi and thus again reduce the possibility of detecting differences between the different TNFi. Fourth, in determining the adjusted HR, we adjusted for a number of potential confounders, but there may still, as in all observational studies, be unobserved or residual confounders, such as human leukocyte antigen (HLA)-B27 status, which may affect the results.
The major strength of this study is that it is a large, nationwide study, based on an unselected population of TNFi-treated patients with AS. An additional strength is that the data are collected from several independent sources, providing pretreatment data on AU flares, and the possibility to adjust for a number of potential confounders.
In conclusion, a reduction in AU rates was observed when initiating ADA and IFX, and an increase when initiating ETN. Based on HR, there was a fourfold increase in risk for AU when starting ETN compared with ADA, and a twofold increase for ETN compared with IFX. These results, in addition to previously published data on this topic, support the choice of another TNFi than ETN in patients with AS with a history of AU.
References
Footnotes
Handling editor Hans WJ Bijlsma
EL and UL co-first authors
EL and UL contributed equally
Contributors All authors have contributed substantially in the process of completing this study and had full access to the data, specified as follows: Conception of the study: EL and LTHJ. Designing the study: All authors. Aggregation of data TZ-S. Statistical analysis TZ-S, ICO, EL and UL. Interpretation of data all authors. Drafting and revising, final approval and agreement to be accountable: all authors.
Funding The study received funding from the following sources, which did not influence either the design of the study, the collection and analysis of the data or the preparation of the manuscript: The Swedish Research Council, Gothenburg University, the Stockholm County Council (ALF), The Swedish National Rheumatism Association, the Swedish COMBINE public-private research programme, the Swedish Cancer Society, the EU-IMI BT Cure project and the Swedish Foundation for Strategic Research. ARTIS has entered into agreements with MAH for rheumatology biologicals (AbbVie, BMS, Merck, Pfizer, Roche, Samsung, UCB) regarding the safety surveillance of these drugs. All authors state their complete independence from the funders, with regard to this study.
Competing interests EL has received personal fees from AbbVie, Bristol-Myers Squibb, Hospira, Pfizer and UCB. LEK has received fees for speaking and consultancy from Pfizer, UCB, Roche, AbbVie, BMS, Novartis, Eli Lilly, Celgene, Biogen and MSD. LTHJ has received Advisory Board fees from AbbVie, Celegen, MSD, Novartis and UCB. JA has participated in advisory boards arranged by Lilly, AstraZeneca and Novartis but not received any personal remuneration.
Ethics approval The regional ethical committee in Stockholm, Sweden, approved the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Technical appendix and statistical codes are available from the corresponding author at request. Consent was not obtained but the presented data are anonymised and risk of identification is low.