Article Text

Abstract
Objective To investigate sick leave and disability pension in rheumatoid arthritis (RA) in relation to the initiation of biological and non-biological antirheumatic therapies in clinical practice.
Methods Patients aged 19–60 years initiating non-biological mono (n=2796) or combination disease-modifying antirheumatic drug (DMARD) therapy (n=973), or biological agents (n=4787) were identified in the Swedish Rheumatology Quality Register between 1999 and 2007. Sick leave and disability pension data (1995–2010) were retrieved from national registers.
Results During the year before the start of mono DMARD, combination DMARD and biological treatment, 10%, 12% and 43% of patients received disability pension benefits, respectively. The corresponding combined annual sick leave and disability pension days were 78 (54+25), 132 (105+27) and 190 (79+111). Irrespective of treatment type, initiators were characterised by a history of increasing sick leave and disability pension. Treatment start was associated with a break in this trajectory: sick leave decreased while disability pension increased, resulting in a net stabilisation of total days. Higher levels of days on sick leave and disability pension at treatment start were observed in patients initiating biologics in 1999 (236 days/year) compared with 2007 (150 days/year; p<0.001), but the trajectory thereafter remained largely similar and contrasted markedly with the level in the general population.
Conclusion Sick leave and disability pension increased rapidly before the initiation of antirheumatic therapy, which was associated with a halt but not a reversal of this development. Work ability is a metric of importance for clinical practice, signalling large remaining needs in the RA population, and the need for intervention earlier in the disease process.
Statistics from Altmetric.com
The therapeutic armamentarium in rheumatoid arthritis (RA) offers a series of efficacious treatments. Newer therapies, including biological agents, together with more ambitious treatment goals, have dramatically increased the direct treatment costs of RA.1 For instance, tumour necrosis factor inhibitor sales in Sweden increased ninefold from 2000 to 2009, and constituted 5% of the national drug expenditure in 2009.2
Apart from treatment costs, RA is also associated with dramatic indirect costs;3 average annual productivity losses in the Swedish RA population are estimated at €16 000 per patient of working age, with €9000 attributable to RA.4 An improvement in work ability through effective disease control thus holds the potential for offsetting some of the increased treatment cost.
Evidence to date on work ability in relation to antirheumatic treatments mainly comes from small samples with limited or no information on sick leave history,5,–,9 and from trials of biological and non-biological disease-modifying antirheumatic drugs (DMARD).10 11 Sick leave has commonly been assessed by self-report, which is associated with non-response and recall bias. Furthermore, lack of control groups, the use of completers analysis and the use of time windows as short as weeks or months (capturing flare effects) may limit the usefulness of findings that ideally should reflect long-term treatment of a chronic disease such as RA. In the absence of large and long-term randomised trials, the work ability trajectory after the initiation of biological agents also needs to be put into perspective of the pattern associated with other pivotal treatment events. For instance, in the extension of an adalimumab trial, no improvement of work ability was found compared with treatment start,6 but the authors noted that no further deterioration may be a good result, as productivity losses tend to increase with disease duration and age.4 12 Finally, as sick leave only makes up approximately 20% of total lost work days in the RA population and disability pension the remaining 80%,4 13 it is recommended to take both metrics into account jointly in analyses of productivity losses.10
The primary aim of this study was to assess the pre-treatment and post-treatment development of work ability (defined as sick leave and disability pension) in relation to standard therapeutic options in RA, in clinical practice. In particular, using national longitudinal registers on sick leave and disability pension, we describe the development of work ability before and after the start of three well-recognised antirheumatic therapies: non-biological DMARD monotherapy, non-biological DMARD combination therapy and biological therapy.
Methods
Patients with RA, and their treatment initiations, were identified in the Swedish Rheumatology Quality Register. This register contains the Swedish Biologics Register ARTIS (1999–), as well as follow-up of incident RA (1995–).14 Based on each Swedish resident's personal identification number, the dataset was merged with the Social Insurance Office database including day-level data on sick leave and disability pension (1995–2010). Ethical approval was granted by the regional ethics committee, Stockholm, Sweden.
Setting
In 2008, Sweden had a population of 9.2 million (Statistics Sweden; http://www.scb.se). The Swedish healthcare system is tax funded and offers universal access, while prescription drugs are provided free of charge above a threshold of SEK1800 annually (≈€180/US$230). In Sweden, patients with inflammatory rheumatic diseases are typically diagnosed and treated by rheumatologists rather than general practitioners. Care for RA is provided in outpatient and inpatient facilities, with the vast majority of rheumatologists working at hospitals rather than as private practitioners. The nationwide prevalence of RA (in 2008) has been estimated as 0.6–0.8% depending on definition.15 In this RA population, the penetration of biological agents has been estimated as 15–18% overall and 20–25% in working age patients.15 For non-biological DMARD, the corresponding percentages were 64–74% and 71–82%.
The Swedish social insurance system provides compensation for sick leave and disability pension, both of which may be complete or partial. Data are recorded by the Swedish Social Insurance Office (Försäkringskassan). The retirement age is generally 65 years, but workers have the right to continue working until age 67 years or start retirement at age 61 years. In this study, the analyses were restricted to patients aged 19–60 years at treatment initiation.
Treatment initiator cohorts
Four cohorts were identified in the Swedish Rheumatology Quality Register based on antirheumatic treatment start between 1999 and 2007: (1) non-biological DMARD monotherapy; (2) non-biological DMARD combination therapy; (3) biological initiators with less than 5 years of RA duration; and (4) biological initiators irrespective of RA disease duration. Cohort selection was based on treatment starts, and therefore the same patient may be included in more than one cohort. Patients in cohorts I–II were identified from the RA inception cohort in the Swedish Rheumatology Quality Register. Patients in cohorts III–IV were identified through ARTIS, covering 87% of all biological agent-exposed RA patients in Sweden.14 15
Data were retrieved from the Register of the Total Population to ascertain whether patients were alive and registered in Sweden on 31 December each year.
Outcome
The primary outcome was net annual sick leave and disability pension days (maximum 365 days per year). Net days were used as both sick leave and disability pension may be complete or partial, and were calculated by multiplying the extent of sick leave or disability pension by the number of days. For example, a net day may equal 1 day of 100% sick leave, 2 days with 50% sick leave, or 1 day of 50% sick leave plus 1 day of 50% disability pension (if having partial sick leave and disability pension simultaneously).
Sick leave
During the study period, the first day of a sick leave episode was unpaid (‘waiting period‘). Compensation for the second to 14th day of sick leave episodes was paid by the employer (‘sick pay period’; 28 days between 1995 and 31 March 1998). Therefore, only episodes exceeding 14 days were recorded in the Social Insurance Office database. After the seventh day of the sick pay period, a doctor's note confirming the medical problem was required.
Disability pension
In 2003, disability pension was replaced by ‘sickness compensation’ (‘sjukersättning’) for 30–64 year olds, and ‘activity compensation’ (‘aktivitetsersättning’) for 19–29 year olds. Both sickness and activity compensation may be time limited or permanent, and require at least a 25% reduction in work ability expected to remain for 1 year or longer. In this study, disability pension was defined as sickness or activity compensation (2003– 2010), or disability pension (1995–2002).
Statistics
Statistical analyses were performed using SAS (version 9.2). Mean days per year of sick leave and disability pension were used as main summary measure. Median days and the percentage of participants with different levels of days of sick leave and disability pension were also calculated for each year.
For the main analysis, mean days per year were calculated from 4 years before the treatment start day until 3 years after. A closer analysis by month from 12 months before to 12 months after treatment start was also conducted. In addition, calendar period trends were investigated for the full biological agents cohort, as the RA patient population selected for biological treatment initiation has changed markedly since 1999.16 17
A p-value of less than 0.05 was considered statistically significant.
Results
Age and sex were similarly distributed, while RA duration differed markedly across the four treatment cohorts, with mono and combination DMARD therapy starting near diagnosis, whereas the mean disease duration among all biological agent initiators (cohort IV) was a decade (table 1). Mean values of the health assessment questionnaire (HAQ), disease activity score using 28 joint counts (DAS28), joint counts, C-reactive protein, erythrocyte sedimentation rate and pain were lowest at combination DMARD initiation, and highest at biological agent initiation.
Characteristics at treatment initiation of working age patients with RA
At therapy initiation, approximately 50% had non-steroidal anti-inflammatory drug treatment registered, and 40% were on steroids (table 1). Methotrexate dominated in both the mono and the combination non-biological DMARD treatment regimes, with methotrexate plus sulfasalazine being the most common combination. Adalimumab (16%), etanercept (36%) and infliximab (45%) accounted for 97.5% of biological agent treatment starts. In the 76% of patients initiating biological agents with a concomitant DMARD, co-medication with methotrexate or sulfasalazine accounted for close to 100%.
Sick leave and disability pension before treatment initiation
The prevalence of partial or complete disability pension was lowest at the start of DMARD monotherapy and highest at the start of biological agents (table 2). Mean days of disability pension per year was four times higher the year before biological treatment start compared with mono and combination DMARD start (111 vs 25 and 27 days). Days on sick leave showed a different pattern, with lower levels for biological agent and DMARD monotherapy initiators, and higher at combination DMARD start (79 and 54 vs 105 days). As evidenced by the medians, the distribution of days tended to be skewed.
Productivity losses during the year (=365 days) before the day of treatment initiation
Monthly sick leave and disability pension in relation to treatment initiation
In all cohorts, the mean monthly days of sick leave and disability pension increased monotonically during the 12 months before treatment start, and peaked 1 month thereafter (figure 1). During the remaining 11 months, the mean stabilised at a level below the peak.

Trajectory of mean days of sick leave and disability pension (per month; max 31) in relation to initiation of therapy with mono disease-modifying antirheumatic drugs (DMARD), combination of DMARD, biological agents in early rheumatoid arthritis (RA) (RA duration <5 years), and biological agents in early and established RA. Error bars are 95% CI.
Annual sick leave and disability pension in relation to treatment initiation
From an annual perspective, mean and median days on sick leave and disability pension also increased in all cohorts until treatment initiation, and peaked during the year after treatment start (figure 2). For all but the mono-DMARD cohort, treatment start was associated with a break in the trajectory in the form of a slower increase, followed by a small rebound after the peak.

(A) Trajectory of mean days of sick leave and disability pension (per year; max 365) in relation to initiation of therapy with mono disease-modifying antirheumatic drugs (DMARD), combination of DMARD, biological agents in early rheumatoid arthritis (RA) (RA duration <5 years), and biological agents in early and established RA. Error bars are 95% CI. (B) Distribution of days of sick leave and disability pension (per year; maximum 365) in relation to initiation of mono-DMARD (top left), combo-DMARD (top right), biological agents in early RA (RA <5 years; bottom left), and biological agents in early and established RA (bottom right). Median shown on secondary y-axis. Note: ‘0’ days may contain sick leave episodes of 14 days or less.
As most patients initiate DMARD monotherapy in conjunction with being diagnosed with RA, the results for this cohort were similar to analyses made in relation to RA diagnosis, as described elsewhere.4 Patients starting DMARD combination therapy stabilised at the initiation year level for at least 3 years after treatment initiation. A similar pattern (although at a higher level) was observed for all patients starting biological agents (cohort IV). However, for patients with less than 5 years RA duration starting biological agents (cohort III), a decrease in sick leave and disability pension was observed at 3 (−11 days/year; 95% CI −17 to −6) but not 2 years (−5 days/year; −10 to 1) after treatment start, compared with the initiation year level.
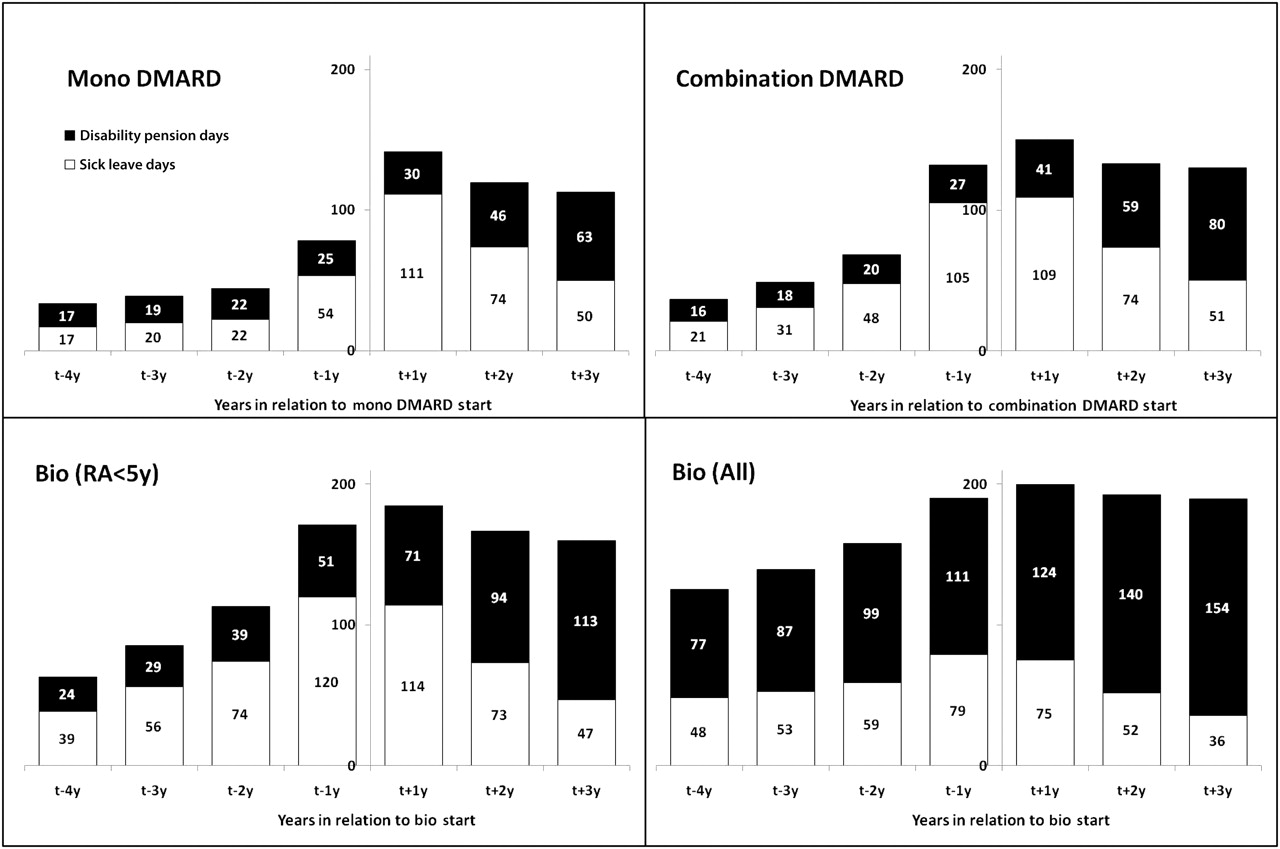
When sick leave and disability pension were assessed separately, sick leave tended to increase until the treatment initiation year, but decreased thereafter (figure 3). By contrast, days on disability pension increased, largely offsetting the decrease, with one exception; in patients with less than 5 years RA duration starting biological agents (cohort III), the decrease in sick leave was not fully compensated for, resulting in a small net improvement in work ability 3 years after initiation compared with the year before (160 vs 171 days; mean difference −11 days, 95% CI −17 to −6).
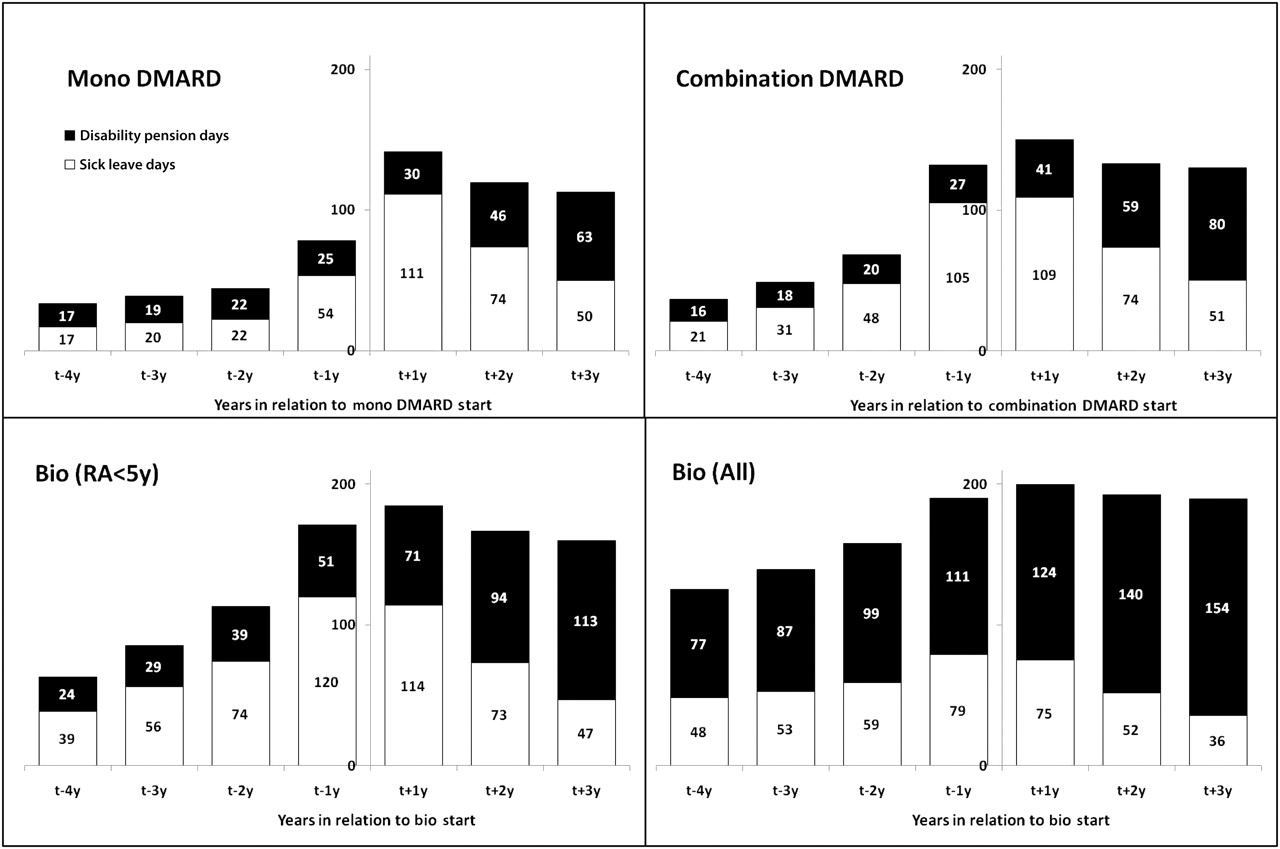
Contribution of mean days from sick leave and disability pension (per year; max 365) in relation to initiation of therapy with mono disease-modifying antirheumatic drugs (DMARD), combination of DMARD, biological agents in early rheumatoid arthritis (RA) (RA <5 years), and biological agents in early and established RA (Bio All).
Calendar period effects
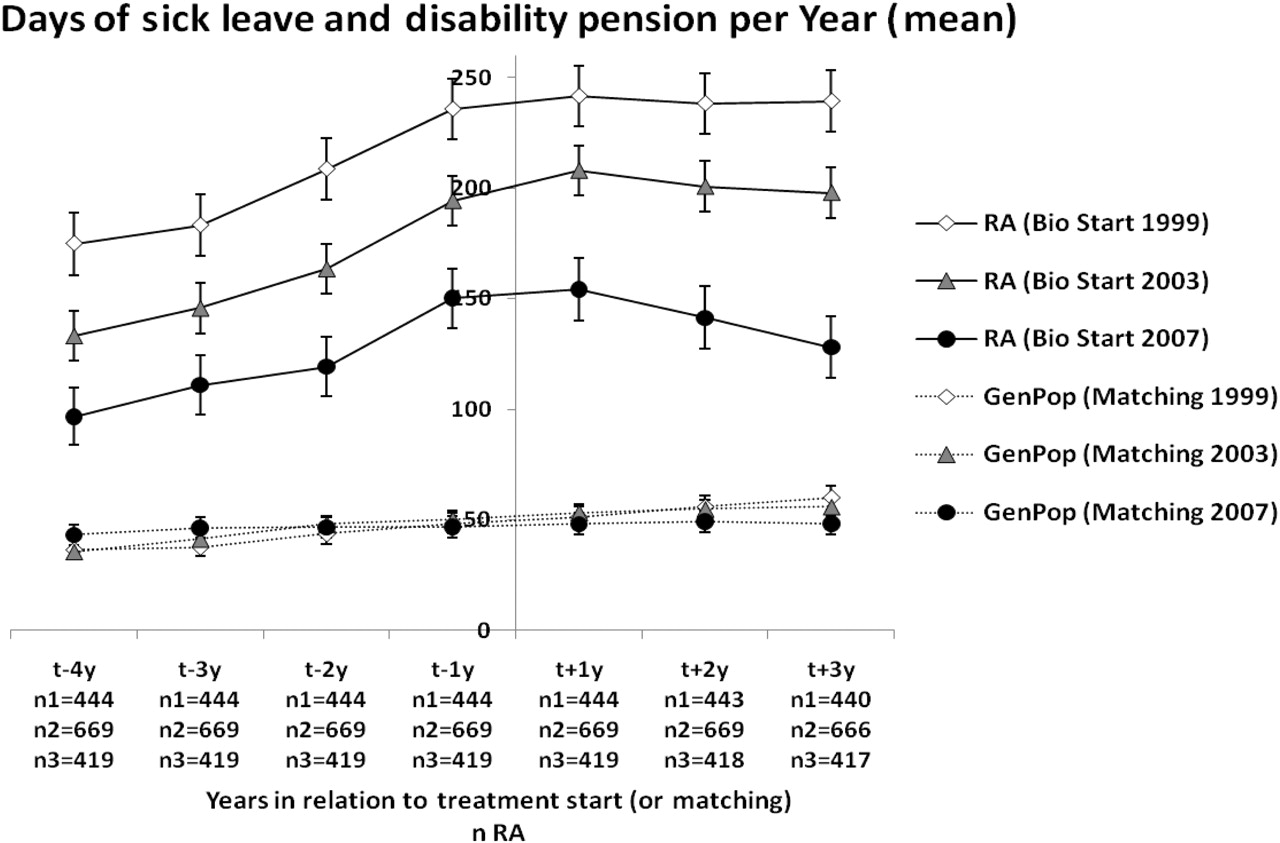
Among all patients initiating biological agents (cohort IV), days on sick leave and disability pension during the year before treatment initiation decreased from 236 days per year (95% CI 222 to 249) in patients starting biological agents in 1999 to 150 (137 to 164) in 2007 (p<0.001). During this period, baseline values for HAQ, DAS28 and other disease measures decreased significantly.17 Although the level of sick leave and disability pension at biological therapy initiation changed during the study period, the shape of the trajectory was largely similar over time, and contrasted markedly with both the level and shape in matched general population comparators (figure 4; data shown for biological agent initiators in 1999, 2003 and 2007). However, for patients initiating biological agents in 2007 there was a decrease from 1 year before treatment start to 3 years thereafter (150 vs 128 days; mean difference −22 days, 95% CI −32 to −14).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Calendar period trends: Mean days of sick leave and disability pension per year (max 365) in patients with rheumatoid arthritis (RA) initiating biological treatment (in 1999, 2003 or 2007) and general population comparators (GenPop; matched for age, sex, county, education and biological agent initiation year). Error bars are 95% CI.
Discussion
We investigated days on sick leave and disability pension in patients with RA before and after the initiation of standard antirheumatic therapies in clinical practice. We made a series of important observations: (1) Irrespective of treatment type, initiators had on average a long history of gradual deterioration in work ability, although, as expected, the level of days off work was higher among patients selected for biological therapy than those starting a first non-biological DMARD monotherapy. (2) Irrespective of treatment type, patients selected for these treatments were characterised by a breakpoint in the deteriorating work ability following treatment start. (3) The halted deterioration in work ability harboured, on average, limited to no reversal in days off work, as treatment-associated declines in sick leave were reciprocated by increased disability pension.
Similar to the study by Mittendorf et al6 on work ability following adalimumab treatment, we found little evidence of improvement in work ability after biological agent initiation. However, when contrasting the dramatic pretreatment and stable post-treatment work ability trajectories, no further deterioration may reflect an important positive outcome in these patients. Our study further demonstrated that this pattern is not exclusive for biological agents but is also characteristic of other antirheumatic treatments with documented (average) effectiveness, and thus that these breakpoints seem to be the work ability counterpart of the (average) clinical response. To this end, our observational findings extend the observations of decreasing sick leave and increasing disability pension in the FIN-RACo trial of non-biological DMARD combination versus monotherapy in early RA.11
Our national data should also be compared with previous findings from two small regional Swedish studies.8 18 Augustsson et al8 reported improvements in weekly work hours after biological agent initiation over up to 5 years in 594 patients. Olofsson et al18 found decreasing monthly sick leave and stable disability pension episodes in 365 patients followed for 360 days after biological agent initiation compared with age and sex-matched general population comparators. Apart from shorter follow-up in the study by Olofsson et al,18 those studies had differently selected patients compared with our study: the first study looked at patients free of disability pension continuing on their first biological agent, while the second was based on a regional subset of patients with median disease duration of 4.5 years (compared with 7.6 years in our study). In the main analysis, we also used a wider time window (year-on-year vs month-on-month changes) and longer pretreatment and post-treatment follow-up.
We found intensive drug treatment to halt but not reverse the deterioration of work ability. The average annual level of sick leave and disability pension after biological agent initiation was close to 200 days out of a maximum 365, and greater than 150 days for combination DMARD starters, indicating a substantial remaining need. Even for early RA patients selected for biological therapy, who experienced improvement after initiation, sick leave and disability still amounted to more than 150 days annually. Given the increase observed already before treatment start, there is an obvious need to identify patients at risk of work ability deterioration much earlier than currently, and potentially break the development. Interestingly, these observations provide an additional argument for the earlier and more precise identification of arthritis patients with a bad prognosis, as the early RA patients (cohort I) were diagnosed according to the 1987 American College of Rheumatology criteria19 less than 1 year before initiation of the first monotherapy. Changes in diagnostic criteria for RA20 should be helpful in this respect, but efforts aimed at the early identification of individuals at risk of RA will also be needed. Work loss history may also be of value to identify patients at risk of future work ability deterioration.21 22
The strengths of this study include the prospectively reported data, both before and after treatment starts. Hereby the flat work ability trajectory after treatment start could be put into the perspective of rapid deterioration in the preceding years, and the effect of biological agents be put into perspective of non-biological DMARD therapies. Another strength was the access to national routinely collected objective data on work ability for large population-based cohorts, instead of repeated self-reports affected by non-response and recall bias. Also, information was available on both sick leave and disability pension. This proved important, as an isolated analysis of sick leave would have resulted in the spurious finding of rapid and continuing improvements in work ability as the post-initiation decrease in sick leave co-occurred with disability pension increases in all cohorts.
The sample size allowed for the examination of calendar period heterogeneity. While these analyses revealed differences in the level of productivity losses, the shape of the trajectories were largely similar. There is a risk that investigations of productivity losses are influenced by legislative and labour market changes. This study included outcome data from 1995 to 2010 and was affected by such changes, but it is unlikely that they explain the associations found: the same pattern was reproduced in different calendar periods and in relation to matched general population comparators. However, a slightly different pattern was seen in the 2007 cohort, with a decrease in total days compared with the year before treatment start in RA patients, and a stable instead of increasing trend in the general population comparators. This calendar period effect has also been seen in relation to RA diagnosis,4 and is probably caused by policy changes. Finally, Sweden has a generous safety net, which may limit generalisability to other countries. However, a review of productivity losses in RA concluded that ‘rates of work disability were similar in the USA and in Northern European countries, despite differences in social systems and study methodologies’,3 and Finnish sick leave and disability pension data show similar levels in relation to diagnosis as described in Sweden.4 23
It should be emphasised that this study was based on patients selected for each of the three therapies under study in standard care, and the treatment groups were not directly comparable. Therefore, we do not offer direct comparisons of one therapy versus the other. The aim was not to make head-to-head comparisons of treatment regimes, but to provide long-term real world data on sick leave and disability pension in relation to the start of different treatments. We conducted the analysis from an intention-to-treat perspective, from the time a patient initiated a certain therapy. Some patients discontinued therapy, although most continued on other therapeutic alternatives if discontinuing their first.17 It is common practice for patients not responding to combination DMARD to initiate biological agents, and for DMARD monotherapy non-responders to start combination therapy or biological agents. Hereby there was a selection of patients when moving up the treatment ladder, which was demonstrated by the greater baseline disease duration and days off work in the biological compared with the non-biological DMARD groups. It should also be pointed out that we assessed mean and median trajectories, but that variation between individual patients was substantial.
In conclusion, patients with RA selected for standard antirheumatic therapies were characterised by a history of gradually deteriorating work ability. Apart from underscoring indication for treatment, this reveals a potential for intervening earlier in the disease course to preserve work ability. The prompt break after treatment start in the deterioration of work ability indicates treatment effectiveness, but the lack of reversal calls for earlier intervention or further improvements to avoid irreversible damage (and labour market inertia), largely precluding patients from returning to work. The profound effects of treatment on work ability suggest that this metric may deserve a role in parallel to standard outcome metrics of inflammation (eg, DAS28) and disability (eg, HAQ) in the delivery and evaluation of clinical care.
Acknowledgments
The authors would like to express their gratitude to all rheumatologists (listed below) contributing data to the Swedish Rheumatology Quality Registers, as well as to Elizabeth Arkema for language revision. Yngve Adolfsson, Sunderby Hospital, Luleå; Ewa Berglin, Norrland's University Hospital, Umeå; Torgny Smedby, Östersund County Hospital; Rüdi Götze, Sundsvall County Hospital; Anna-Carin Holmqvist, Hudiksvall's Hospital; Sven Tegmark, Gävle County Hospital; Jörgen Lysholm, Falu Lasarett, Falun; Solveig Gustafsson, Karlstad's Central Hospital; Eva Baecklund, Akademiska Hospital, Uppsala; Rolf Oding, Västerås Hospital; Per Salomonsson, University Hospital, Örebro; Birgitta Nordmark, Karolinska University Hospital, Solna; Ingiäld Hafström, Karolinska University Hospital, Huddinge; Göran Lindahl, Danderyd's Hospital, Stockholm; Gun Sandahl, Queen Sophia Hospital, Stockholm; Martin Mousa, Visby Lasarett, Visby; Anders Lindblad, Visby Privat, Visby; Åke Thörner, Mälarsjukhuset, Eskilstuna; Lars Cöster, University Hospital, Linköping; Sören Transö, County Hospital Ryhov, Jönköping; Olle Svernell, Västervik's Hospital; Claudia Jacobs, Oskarshamn's Hospital; Bengt Lindell, Kalmar County Hospital; Maria Söderlin, Växjö's Central Hospital; Olof Börjesson, Växjö Privat; Göran Kvist, Centrallasarettet Borås; Karin Svensson, Kärnsjukhuset, Skövde; Tomas Torstenson, Uddevalla Hospital; Ingeli Andreasson, Göteborg privat; Lennart Bertilsson, Sahlgrenska University Hospital, Gothenburg; Tore Saxne, University Hospital, Lund; Miriam Karlsson, Lasarettet Trelleborg; Annika Teleman, Spenshult, Oskarström; Catharina Keller, Helsingborg's Lasarett; Astrid Schröder, Ängelholm's Hospital; Jan Theander, Kristianstad's Central Hospital; Christina Book, MAS University Hospital, Malmö.
References
Footnotes
-
The ARTIS Study Group E Baecklund (Uppsala University), L Cöster (Linköping University), C Dackhammar (Sahlgrenska Academy), N Feltelius (Medical Products Agency), P Geborek (Lund University), L Jacobsson (Lund University), L Klareskog (Karolinska Institutet), S Lindblad (Karolinska Institutet), S Rantapaa-Dahlqvist (Umeå University), T Saxne (Lund University) and R van Vollenhoven (Karolinska Institutet).
-
Competing interests The ARTIS Study Group conducts scientific analyses using data from the Swedish Biologics Register ARTIS run by the Swedish Society for Rheumatology. For the maintenance of this register, the Swedish Society for Rheumatology has received funding, independent of the conduct of these scientific analyses, from Schering-Plough, BMS, Wyeth, Abbott Laboratories, UCB and Roche.
-
Ethics approval This study was conducted with the approval of the regional ethics committee at the Karolinska Institute, Stockholm, Sweden.
-
Provenance and peer review Not commissioned; externally peer reviewed.
↵* See end of paper for members of the ARTIS Study Group.