Article Text

Abstract
Introduction Bone marrow oedema (BMO) of the sacroiliac joints (SIJs) is a hallmark of axial spondyloarthritis (SpA). However, the relationship between the extent of BMO and disease phenotype is poorly understood.
Objective To assess the link between BMO of the SIJs and gut inflammation. We have also evaluated the correlation between BMO and established disease activity parameters.
Methods Sixty-eight patients with axial SpA from the Gent Inflammatory Arthritis and spoNdylitis cohorT underwent ileocolonoscopy and MRI of the SIJs. Histopathological analysis and SPondyloArthritis Research Consortium of Canada (SPARCC) scores were performed.
Results A significant higher SPARCC score (median (range)) was observed in axial SpA patients showing chronic gut inflammation (16.9 (3.8–68.3)) compared with axial SpA patients showing normal gut histology (9.8 (0.0–45.0); p<0.05). In a multiple linear regression model, we identified, besides chronic gut inflammation (effect size of 11.3, 95% CI (2.1 to 20.4)), male sex (effect size of 10.5, 95% CI (3.3 to 17.8)) to be independently associated to the extent of BMO. There was a low to moderate correlation between the degree of BMO and C-reactive protein(r=0.39, p=0.002) and Ankylosing Spondylitis Disease Activity Score (r=0.35, p=0.007).
Conclusions Higher degrees of BMO were observed in patients showing chronic gut inflammation. These data solidify a link between mucosal inflammation and progressive disease in axial SpA.
- Spondyloarthritis
- Magnetic Resonance Imaging
- Inflammation
Statistics from Altmetric.com
Introduction
In spondyloarthritis (SpA), an intriguing link between gut and joint inflammation exists. About half of the patients show microscopic inflammatory gut lesions, a fraction of which evolves into Crohn's disease. Over the past decade a marked progress has been achieved to diagnose SpA at an earlier stage before structural damage has occurred. New imaging modalities such as MRI of sacroiliac joints (SIJs) and spine have been widely validated. The results of these studies have led to new insights into how the disease emerges and are reflected by new SpA classification criteria developed by the Assessment of SpondyloArthritis international Society (ASAS) consortium.1 Therefore, the terms axial and peripheral SpA have been introduced to define primarily axial versus peripheral joint involvement. Recently, the high prevalence of microscopic gut inflammation was confirmed in a patient cohort fulfilling the ASAS criteria for axial and peripheral SpA (Gent Inflammatory Arthritis and spoNdylitis cohorT (GIANT)), and several risk factors for microscopic gut inflammation were identified.2
MRI is one of the modalities that enables us to identify early in the disease course patients with non-radiographic axial SpA (nr-axSpA) by assessing bone marrow oedema (BMO) of the SIJs (imaging arm). However, the correlation between the extent of BMO and different measures of disease activity remains unclear. This study was designed to assess the link between BMO of the SIJs and gut inflammation. Furthermore, we have evaluated the correlation between BMO and established disease activity parameters.
Methods
Study population
The GIANT is a prospective observational cohort in which patients diagnosed with SpA and classified according to the ASAS criteria are prospectively followed. Ileocolonoscopy was performed in 68 consecutive patients, naive to tumour necrosis factor-α (TNF-α) blockers. MRI of the SIJs was performed in all patients. Patients with complete ankylosis of the SIJs were excluded from the analysis as they showed no BMO.
History and investigations
MRI
Images were obtained on a 1.5 T MRI unit (Avanto/Symphony, Siemens Medical, Erlangen, Germany). The SIJs were imaged in a body flexed array coil (Siemens Medical, Erlangen, Germany). Sequence protocol included semicoronal (along long axis of the sacral bone) T1-weighted turbo spin echo (TSE) (slice thickness (ST) 3 mm; repetition time/echo time (TR/TE) 595/20 ms); semicoronal STIR (ST 3 mm; TR/TE/inversion time (TI) 5030/67/150 ms); axial T2-weighted FS TSE (ST 6 mm; TR/TE 5260/13 ms); axial STIR (ST 5 mm; TR/TE/TI 7540/67/150 ms). The SPondyloArthritis Research Consortium of Canada (SPARCC) method was used for scoring BMO in the SIJs.3 All scores were performed by an experienced musculoskeletal radiologist (LJ), who was trained and calibrated by the SPARCC online MRI training module. As we used ST 3 mm in the semicoronal STIR sequence, we scored eight coronal slices instead of the usual six slices. All scores were converted to a maximum score of 72 by multiplying the obtained score by 3/4.
Ileocolonoscopy
In each patient, 4–14 biopsies were taken of ileum and colon, with a median number of six specimens per patient. The biopsies were read and classified by an experienced pathologist (CC), who was unaware of macroscopic findings and the patient's diagnosis.
Other
Laboratory tests included inflammatory parameters, human leucocyte antigen-B27 (HLA-B27) determination and peripheral blood cell examination. All patients were asked to complete the following questionnaires: Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath Ankylosing Spondylitis Functional Index (BASFI) and visual analogue scale (VAS) global disease activity.
Histological classification
Two histological types of microscopic gut inflammation can be distinguished in SpA—acute and chronic inflammation—as previously reported.4 This classification refers to the observed morphological characteristics, not to the disease duration. Similar to previous ileocolonoscopic studies,5 a diagnosis of chronic inflammation was made whenever a biopsy featured chronic lesions, regardless of acute inflammation in other fragments.
Statistical analysis
Data were analysed using SPSS V.19. Non-parametric independent sample testing (Kruskal–Wallis and Dunn–Bonferroni posthoc testing with correction for multiple testing) was performed to compare the SPARCC scores between the patients according to histological classification. Subsequently, multiple linear regression analysis was performed to adjust for confounding factors (age, sex, HLA-B27 positivity). The intraobserver reproducibility was assessed by calculating an intraclass correlation coefficient (ICC). A two-way random model for absolute agreement was used. The correlations were studied with Spearman’s rank-based correlation coefficient. The data are expressed as median (range); for all analyses p<0.05 was considered statistically significant. Analyses were restricted to the individuals with complete data.
Results
Patients
Sixty-eight patients were screened, of which 62 were included in the analysis. Because of total ankylosis of the SIJs, six patients were excluded from the study analysis. Median time between MRI and ileocolonoscopy was 1.44 months. Baseline demographic and clinical characteristics are presented in table 1. In total, 3 of 16 patients with histology of chronic gut inflammation had a recent or an established diagnosis of inflammatory bowel disease (IBD).
Baseline demographic and clinical characteristics of the study population
Degree of BMO in patients with and without gut inflammation
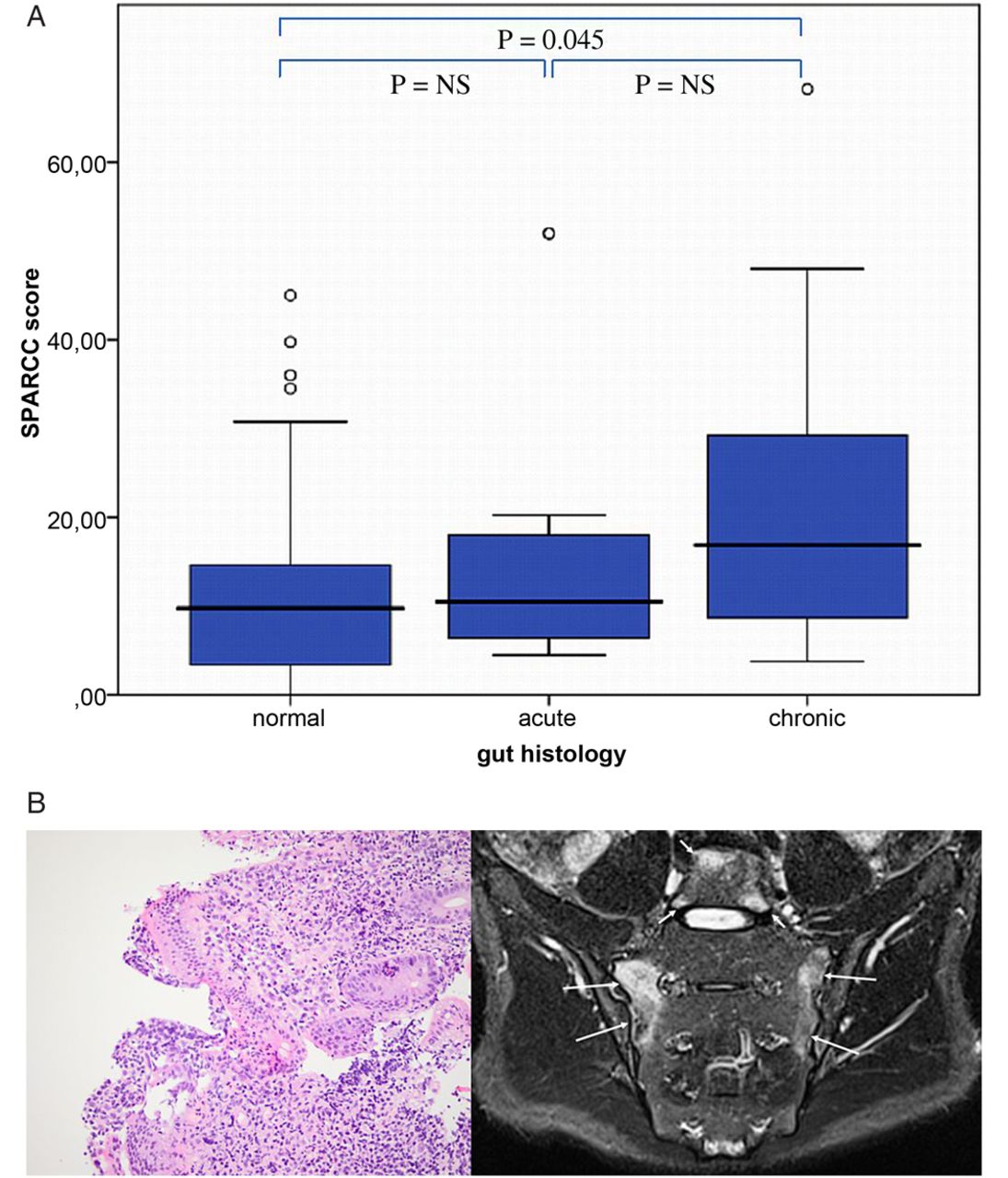
The median SPARCC score of each group is presented in figure 1A. A significant difference was found between axial SpA patients showing chronic gut inflammation (16.9 (3.8–68.3)) and patients with normal gut histology (9.8 (0.0–45.0); p<0.05). This is clearly illustrated by figure 1B, showing chronic gut inflammation on ileal biopsy in a patient with extensive BMO on MRI (SPARCC score 48/72).
{kind=link}
(A) Comparison of the median SPARCC-scores of patients with normal, acute and chronic gut histology. NS, not significant. (B) Left: Active granulocytic infiltration of villus epithelium and chronic dense lymphoplasmocytic cellular infiltrate in the lamina propria (H&E; original magnification ×20). Right: Semicoronal STIR MR image shows active inflammation as bilateral bone marrow oedema of the sacroiliac joints (long arrows) and at the corners of the L5 vertebral body (short arrows).
These results were confirmed in a multiple linear regression analysis: adjusted for age, HLA-B27 positivity and male sex, chronic gut inflammation was associated with higher SPARCC scores compared with normal gut histology, with an effect size of 11.3 (95% CI (2.1 to 20.4)). Additionally, we identified male sex to be independently associated with higher SPARCC scores, with an effect size of 10.5 (95% CI (3.3 to 17.8). No significant association with age or HLA-B27 positivity was found.
Reliability of the SPARCC scoring system
For a subset of 30 patients, a second reading was performed. The intraobserver variability was very small, with an ICC of 0.99.
Correlation between BMO and established disease activity parameters
As a next step, we evaluated the correlation between BMO and established disease activity parameters. These results are presented in table 2. C-reactive protein (CRP) (r=0.39, p=0.002) and Ankylosing Spondylitis Disease Activity Score (ASDAS) (r=0.35, p=0.007) showed a low to moderate correlation with the SPARCC score. No correlation with BASDAI or patient global VAS score was found.
Spearman correlation coefficients (and p values) between disease activity parameters and SPARCC score
Discussion
In this study, we found that gut inflammation is linked to degree of BMO in SIJs of patients with axial spondyloarthritis. More specifically, highest levels of BMO were found in patients with chronic gut lesions. In the current analysis, patients with overt IBD (n=3) were not excluded, as we were interested in the link between disease activity and gut inflammation in general, not restricted to microscopic involvement. However, results were similar when patients with overt IBD were excluded from the analysis. Thus, our findings indirectly illustrate the evidence of a relationship between inflammation and progressive disease6–8 as SpA patients with chronic gut inflammation are known to evolve more frequently to ankylosing spondylitis.9
One of the major reasons for designing the new ASAS classification criteria for axial and peripheral SpA was the well-known ascertainment that by applying modified NY criteria for AS there is a rather long delay between symptom onset and definitive diagnosis.10 This was partly alleviated by the Amor11 and the ‘European Spondyloarthropathy Study Group’ (ESSG) criteria,12 as radiographic sacroiliitis was not longer required to fulfil these criteria. However, especially with the latter, there was the fear for less specificity,13 which is important if these criteria would be used for decisions on the use of expensive new (biologic) drugs. The ASAS criteria allow classification of both classic AS (radiographic axSpA) as well as an entity, which is named nr-axSpA. In our study, 66.1% of patients did not fulfil the modified New York criteria for AS and could thus be classified as nr-axSpA. At present, long-term data are lacking to determine which proportion of nr-axSpA patients progresses to the radiographic stage of the disease. Preliminary data suggest that the progression rate from non-radiographic to radiographic axial SpA over 2 years is about 10%, and around 20% in patients with active inflammation on MRI of the SIJ.14 Identifying patients at risk for early progression, who would benefit from more aggressive therapeutic strategies, is probably one of the greatest challenges for the future. The results of this study add a novel factor, chronic gut inflammation, to this risk stratification.
The multiple regression analysis confirmed the independent association, not related to HLA-B27 positivity or age, and additionally identified male sex as a predictor of higher degrees of BMO. Indeed, male sex is a well-established parameter of MRI inflammation and progressive disease.15–18 Previous reports have suggested a link between HLA-B27 positivity and MRI inflammation of the SIJs.17–19 However, in these studies, either no adjustment for confounding factors was done or only the absence or the presence of BMO was assessed (not the extent).
We have also evaluated the correlation between BMO of the SIJs and established clinical disease activity parameters. SPARCC scores correlated weakly to moderately with CRP (r=0.39, p=0.002) and ASDAS (r=0.35, p=0.007). Machado et al20 and Konca et al21 performed similar analyses assessing BMO in the spine and also found weak to moderate correlations with CRP and ASDAS. In a smaller study by Soliman et al,22 MRI features of activity were not related to CRP; however, BMO was not assessed quantitatively in this study, making a comparison difficult. Similar to our and previous reports,23–25 there were no correlations between MRI scores and other disease activity measures, namely BASDAI and patient global VAS score. Therefore, our data regarding clinical disease activity and BMO of the SIJs are entirely consistent with the data in the referred studies on BMO in the spine. As we did not perform MRI of the spine systematically, we cannot comment on this in our study population.
There are some limitations to our study. We clearly established the link between chronic gut lesions and BMO of the SIJs. Possibly because of the smaller number of patients with acute gut histology, we cannot draw definite conclusions on this type of gut inflammation. However, prospective follow-up studies have shown that these acute lesions resolve spontaneously in most cases.5 Furthermore, we used the SPARCC score to quantitate BMO in the SIJs. However, this scoring method only assesses six (eight) coronal slices that demonstrate the cartilagenous portion of the SIJs, providing no information on the other parts. It would be interesting to confirm our results in future studies with other validated scoring systems (Berlin, Leeds or Danish SIJ MRI scoring method).
As chronic mucosal inflammation seems to be linked to active inflammation (BMO) on MRI of the SIJs, with the latter having an approximately twofold higher progression rate from nr-axSpA to classic AS,14 our data on the link between BMO of the SIJs and gut inflammation provide clinicians with an extra tool to stratify patients at higher risk for progression.
References
Footnotes
Handling editor Tore K Kvien
-
Contributors LVP, LJ, FVdB, PJ, PC, MDV, HM and DE are responsible for study conception and design. LVP, PJ, EG, MDV and HC are responsible for acquisition of data. LVP, CC, RC, LJ and DE are responsible for analysis and interpretation of data.
-
Funding This study was supported by a grant of the Clinical Research Funding of Ghent University Hospital to LVP. DE is supported by a fund of Scientific Research–Flanders (FWO) and the Research Council of Ghent University. DE is also a member of a multidisciplinary research platform (MRP) of Ghent University and is supported by Interuniversity Attraction Pole (IUAP) grant Devrepair from the Belspo Agency(project P7/07). This project received funding from the EU's seventh framework program under EC-GA n° 305266 ‘MIAMI’.
-
Competing interests None.
-
Patient consent Written informed consent was obtained from all patients, prior to any study related procedure.
-
Ethics approval The study protocol was approved by the Ethical Committee of Ghent University Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.