Article Text

Abstract
Objective The primary objective of this prospective case-control study was to assess the diagnostic value of several intra-articular and periarticular ultrasound (US)-detected abnormalities in the upper and lower limbs in gout. The secondary objective was to test the concurrent validity of US abnormalities using as gold standard the microscopic demonstration of monosodium urate (MSU) crystals.
Methods Ninety-one men with gout and 42 age-matched controls were prospectively recruited. All patients with gout and controls underwent US assessment of several US abnormalities in 26 joints, six bursae, eight tendons, 20 tendon compartments, four ligaments, and 18 articular cartilages by experts in US blinded to the patients’ group. Patients with gout and controls with US abnormalities were asked to undergo US-guided aspiration for microscopic identification of MSU crystals. Interobserver and intraobserver reliability of the US assessment was evaluated in a web-based exercise.
Results The assessment of one joint (ie, radiocarpal joint) for hyperechoic aggregates (HAGs), two tendons (ie, patellar tendon and triceps tendon) for HAGs and three articular cartilages (ie, first metatarsal, talar and second metacarpal/femoral) for double contour sign showed the best balance between sensitivity and specificity (84.6% and 83.3%, respectively). Intraobserver reliability was good (mean κ 0.75) and interobserver reliability was moderate (κ 0.52). The aspirated material from HAGs was positive for MSU crystals in 77.6% of patients with gout and negative in all controls.
Conclusions Our results suggest that US bilateral assessment of one joint, three articular cartilages and two tendons may be valid for diagnosing gout with acceptable sensitivity and specificity.
- Ultrasonography
- Gout
- Arthritis
Statistics from Altmetric.com
Introduction
Gout is a common disease caused by monosodium urate (MSU) crystal deposition, which is a consequence of the degree and duration of chronic hyperuricaemia.1 MSU crystals mainly appear in the subcutaneous tissue and inside and around joints, where they can produce acute and/or chronic arthritis.2 Furthermore, gout has been associated with renal impairment and cardiovascular disease.3 Effective urate-lowering therapy leads to tophi dissolution and prevents crystal formation.4–6
Diagnosis of suspected gout is based on typical clinical (eg, recurrent self-limited podagra) and laboratory (ie, hyperuricaemia) findings, while definitive diagnosis requires identification of MSU crystals in aspirated synovial fluid or tophi.7 This procedure is easy to carry out in inflamed joints during acute attacks or chronic gouty arthritis but may not be feasible in non-inflamed joints during intercritical periods.
Tophi, the characteristic deposits of gout, are composed of a core of MSU crystals, encased by dense connective tissue.8 Physical methods detect only subcutaneous tophi whereas imaging techniques such as ultrasound (US), MRI, CT and dual energy CT (DECT) identify deep MSU crystal deposits.9 Among these imaging modalities, US is by far the most available imaging tool in clinical practice.
There are a number of published studies that have shown the capability of US to detect certain intra-articular (ie, synovial recesses, articular cartilage) and periarticular (ie, tendons, ligaments, bursae) abnormalities in patients with gout compared with healthy controls10 ,11 or patients with other joint diseases.10 ,12–15 A variety of US abnormalities have been identified as MSU crystal deposits in these studies.10–15 Among them, US-detected tophi have demonstrated construct validity compared with MRI findings16 and concurrent validity compared with microscopic observation of MSU crystals in US-detected tophus samples aspirated under US guidance.16 The above studies have separately analysed the diagnostic value of some US-detected gout abnormalities in a variable number of target joint areas, mainly in the lower limbs.10–16 However, to the best of our knowledge, no study has addressed the optimal combination of US-detected abnormalities and target locations in the diagnosis of gout.
The primary objective of the present prospective case-control study was to assess the diagnostic value of the combinations of intra-articular and periarticular US-detected abnormalities typical of gout in the upper and lower limbs and to select the best minimal combination of anatomic structures to diagnose gout in intercritical periods. The secondary objective was to test the concurrent validity of the US-detected abnormalities that were accessible and appropriate for US-guided internal aspiration using as gold standard the microscopic demonstration of MSU crystals.
Methods
Study population
Ninety-one men with MSU crystal-proven primary gout and 42 age-matched controls (ie, 16 patients with rheumatoid arthritis (RA), 11 patients with spondyloarthritis (SpA) and 15 healthy subjects) were prospectively recruited at six Spanish centres. Patients with gout and controls were recruited and clinically assessed by trained general practitioners (ie, healthy controls) or rheumatologists (ie, gout, patients with RA and SpA) at each centre.
Inclusion criteria for patients with gout were the following: age ≥18 years; MSU crystal proven primary gout diagnosed by a rheumatologist; no history of any inflammatory, degenerative or infectious musculoskeletal disease; not to have received corticosteroid injections in the studied anatomic areas in the 3 months previous to study entry; no gout attack at study entry; patient acceptance and capability to participate in the study. Exclusion criteria for patients with gout were severe renal insufficiency (ie, glomerular filtrate rate <30%), psoriasis, drug-induced gout and other secondary gout types.
Inclusion criteria for patients with RA and SpA are listed in the online supplementary text17 ,18. The study was conducted in accordance with the Declaration of Helsinki and was approved by the local ethical committee of the Hospital Universitario Severo Ochoa, Hospital Universitario de Móstoles, Hospital Puerta de Hierro, Hospital Universitario de Alicante Hospital de la Princesa, and Hospital Ramón y Cajal. Written informed consent was obtained from all patients before study enrolment.
Clinical assessment
All patients with gout and controls underwent a clinical assessment which included the following data: demographics (ie, sex, age, disease duration), alcohol and medication consumption in the year previous to the inclusion, and body mass index (BMI). In addition, patients with gout were questioned about the time since the first attack, the number of attacks per year and in the last year, and the type and duration of the urate-lowering therapy. In patients with RA and SpA, presence of rheumatoid factor (RF) and cyclic citrullinated peptide (CCP) antibodies, and HLA-B27 antigen, respectively, and disease activity19–21 were also recorded (see online supplementary text). The presence and location of subcutaneous tophi was investigated in patients with gout and controls. For each patient with gout and each control, total cholesterol, triglycerides, glycaemia, uricaemia, C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) were obtained from laboratory tests at study entry.
US assessment
The recruited patients with gout and controls were referred to a rheumatologist highly experienced in musculoskeletal US at each centre (ie, 10–15 years of experience in musculoskeletal US). This was done in a predetermined fashion. Each rheumatologist ultrasonographer received the same proportion of patients with gout and controls and a similar number of patients. These experts were unaware of the patients' group (gout or control group) and the clinical findings. They had a similar background in musculoskeletal US. In addition, further standardisation of scanning technique and identification of abnormalities typical of gout was conducted among investigators prior to the study (see online supplementary text).
For each patients with gout and each control, a systematic longitudinal and transverse multiplanar US examination on B mode (ie, grey scale (GS)) of 26 joints (42 synovial recesses), six bursae, eight tendons and 20 tendon compartments, four ligaments and 18 articular cartilages (30 cartilage areas) (see online supplementary text) was carried out with real-time scanners in all centres (Logiq 9; GE Medical Systems Ultrasound & Primary Care Diagnostics, LLC, Wauwatosa, Wisconsin, USA, in five centres; Logiq 7, GE Medical Systems Ultrasound & Primary Care Diagnostics, LLC, Tokyo, Japan, in one centre) using multifrequency linear array transducers (8–14 MHz). To reduce the possibility of bias, the patients were asked not to talk about their clinical data to the US examiner. We also maximised the level of darkness in the examination room. GS machine settings were standardised among investigators prior to the study to optimise US scanning of superficial and deep anatomic areas. These settings were as follows: dynamic range of 40–50 dB, GS frequency of 12–14 MHz and GS gain of 60 dB.
US features of MSU crystal deposition were defined based on the literature10–16 22–31 and the experience of the authors as follows. Intra-articular and intrabursal tophi were defined as heterogeneous hyperechoic (relative to subdermal fat) aggregates with poorly defined margins with or without areas with acoustic shadowing within the synovial recesses or bursae, respectively. Tendon and ligament tophi were defined as heterogeneous hyperechoic (relative to tendon/ligament fibres) aggregates with poorly defined margins with or without areas with acoustic shadowing within and/or around the tendon or ligament, respectively. MSU crystal deposition in tendons was also defined as hyperechoic (relative to tendon fibres) linear bands (HLBs) within the tendon substance. MSU crystal deposition in articular cartilage was defined as hyperechoic irregular enhancement of the chondrosynovial margin of the cartilage that is independent of the insonation angle of the ultrasound beam (ie, double contour sign).
Microscopic assessment
Patients with gout or controls with positive US findings for MSU crystal deposits appropriate for percutaneous internal aspiration, that is, intra-articular, intrabursal or tendon/ligament hyperechoic aggregates (HAGs), were asked to undergo aspiration of the most superficial and accessible site. For those who agreed, a US-guided aspiration with a 21 G needle was performed following a standard sterile procedure. The material obtained was immersed in isotonic saline 0.9% in the same syringe and examined for negatively birefringent MSU crystals with polarised, red-compensated light microscopy. Only one puncture per patient was allowed. Crystal microscopic examination was performed by experts at each centre who were blinded to the patients' group (gout or control group) and the clinical findings.
US intraobserver and interobserver reliability
Interobserver and intraobserver reliability of the US assessment was evaluated in a web-based exercise. The investigators collected 40 US images representative of intra-articular, intrabursal, tendon and articular cartilage MSU crystal deposits from patients with gout and 30 US images of synovial recesses, bursae, tendon and articular cartilage without MSU crystal deposits from healthy controls or patients with RA or SpA. The anatomic locations were those included in the study. These images were randomly displayed twice in the web-based exercise. Each set of images was evaluated separated by 2 weeks. The investigators assessed the images for the presence or absence of MSU crystal deposits in the above anatomic structures.
Statistical analysis
Statistical analysis was performed using SPSS, V.15.0 (SPSS, Chicago, Illinois, USA). Quantitative variables were presented as the mean±SD and range. Categorical variables were presented as absolute frequencies and percentages. Comparisons between two independent means were analysed using the Student t test or Mann–Whitney test, and analysis of variance with post hoc Tukey pairwise comparisons or the Kruskal–Wallis test were used to compare three or more independent means. Relationships between categorical variables were evaluated by Fisher's exact test (2×2 tables) or χ2 test (tables bigger than 2×2), using Haberman standardised residuals to determine cells contributing to the overall χ2 statistic.
To select optimal combinations of US-detected gout abnormalities and anatomic locations, we investigated what combinations of joints, bursae, cartilages, tendons and ligaments were more frequently involved in patients with gout as a first step. In the second step, we calculated separately the sensitivity and specificity for each combination obtained in the previous step to determine which combinations showed better sensitivity and specificity. In the third step, we mixed the three combinations that showed better sensitivity and specificity. This mixed model increased sensitivity but decreased specificity. Then, we removed anatomic structures from the mixed model to obtain the minimal combination of US-detected abnormalities and anatomic locations that yielded the best balance between sensitivity and specificity for diagnosing gout. Positive predictive value and negative predictive value were also calculated for all combinations.
Interobserver reliability was assessed by Light's κ (mean κ for all pairs of observations). Intraobserver reliability was assessed by unweighted Cohen's κ. κ values of 0–0.20 were considered poor, 0.20–0.40 fair, 0.40–0.60 moderate, 0.60–0.80 good and 0.80–1 excellent.32 p Values less than 0.05 were considered significant.
Results
Demographics and clinical characteristics of patients with gout and controls
Table 1 displays demographics and clinical and laboratory findings in patients with gout and controls. Alcohol consumption was significantly greater among patients with gout (74 (81.3%)) than controls (21 (50%)) (p=0.001). Subcutaneous tophi were detected in nine (9.9%) patients with gout in the elbows, five (5.5%) with gout in the hands, two (2.2%) with gout in the knees, six (6.6%) with gout in the heels, and 13 (14.3%) with gout in the feet. None of the controls showed subcutaneous tophi.
Demographics and clinical and laboratory findings in gout patients and controls
Clinical data for patients with gout, RA and SpA are shown in the online supplementary text.
Global US findings in patients with gout versus controls
With US, we evaluated in total 3822 joint sites, 2912 tendons/tendon compartments/ligaments, 2730 cartilage areas, and 546 bursae in patients with gout and 1764 joint sites, 1344 tendons/tendon compartments/ligaments, 1260 cartilage areas, and 252 bursae in controls. Table 2 shows the prevalence of each US abnormality and the mean number of these abnormalities in patients with gout and controls. There was a significantly higher percentage of patients with gout than controls who showed the following abnormalities: intra-articular or intrabursal HAGs, tendon/ligament HAGs, tendon HLBs, and cartilage double contour sign (DCS).
Prevalence and number per patient of US abnormalities in patients with gout and controls
When we analysed tendons that showed only HAGs (ie, without HLBs), there was also a significantly higher percentage of patients with gout who showed these findings compared with controls (30 (33%) patients with gout vs four (9.5%) controls) (p=0.005). However, there was no significant difference in the presence of tendon HLBs without tendon HAGs between patients with gout and controls (23 (25.3%) vs 11 (26.2%), respectively) (p=1.000). The distribution of US abnormalities among patients with RA, those with SpA and healthy controls is shown in the online supplementary text.
Representative US intra-articular and periarticular abnormalities in patients with gout are shown in figures 1⇓⇓–4, respectively.

Longitudinal US image of the wrist joints. Hyperechoic aggregates (arrowheads) are seen within the synovial recesses of the radiocarpal and midcarpal joints. r, radius.
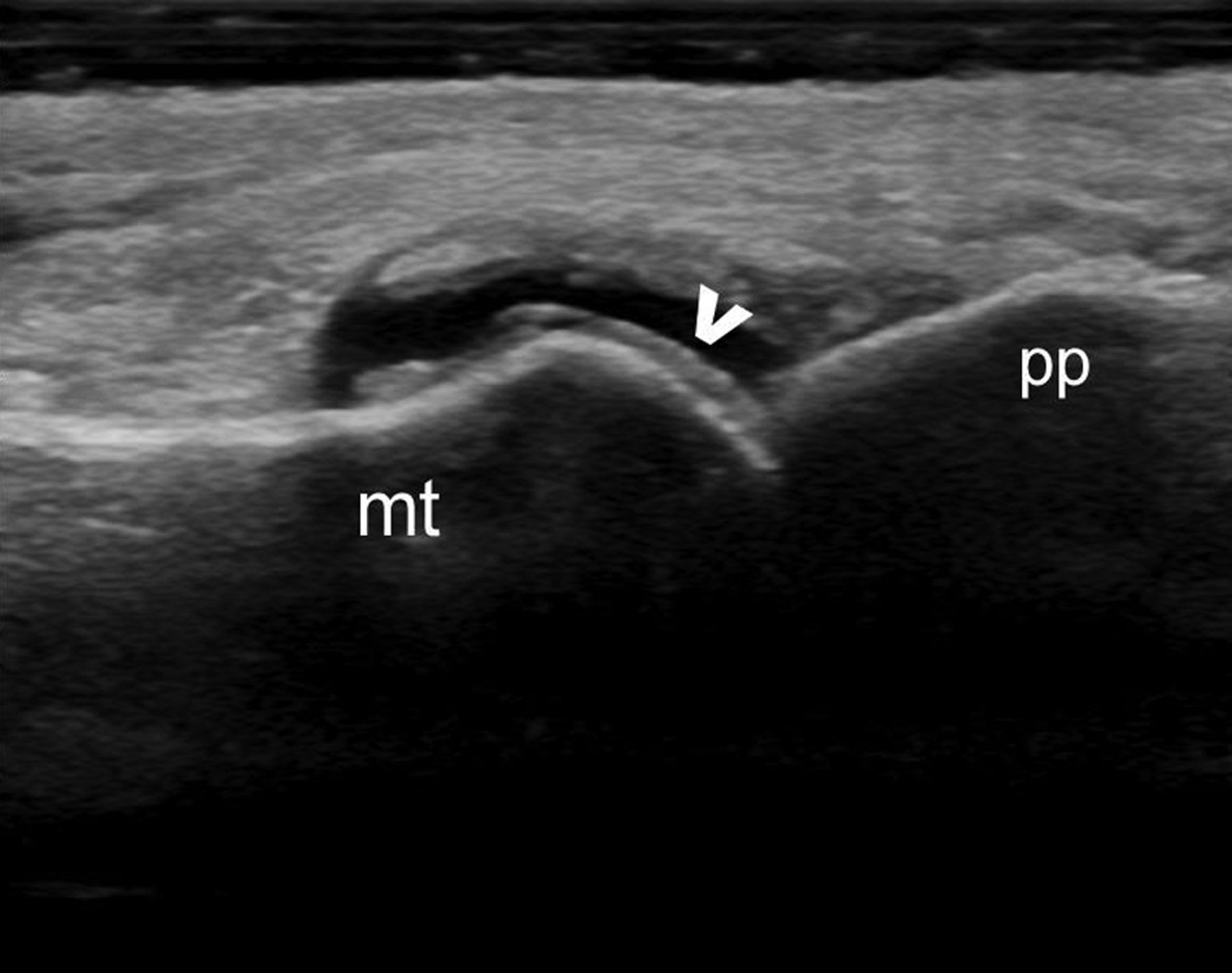
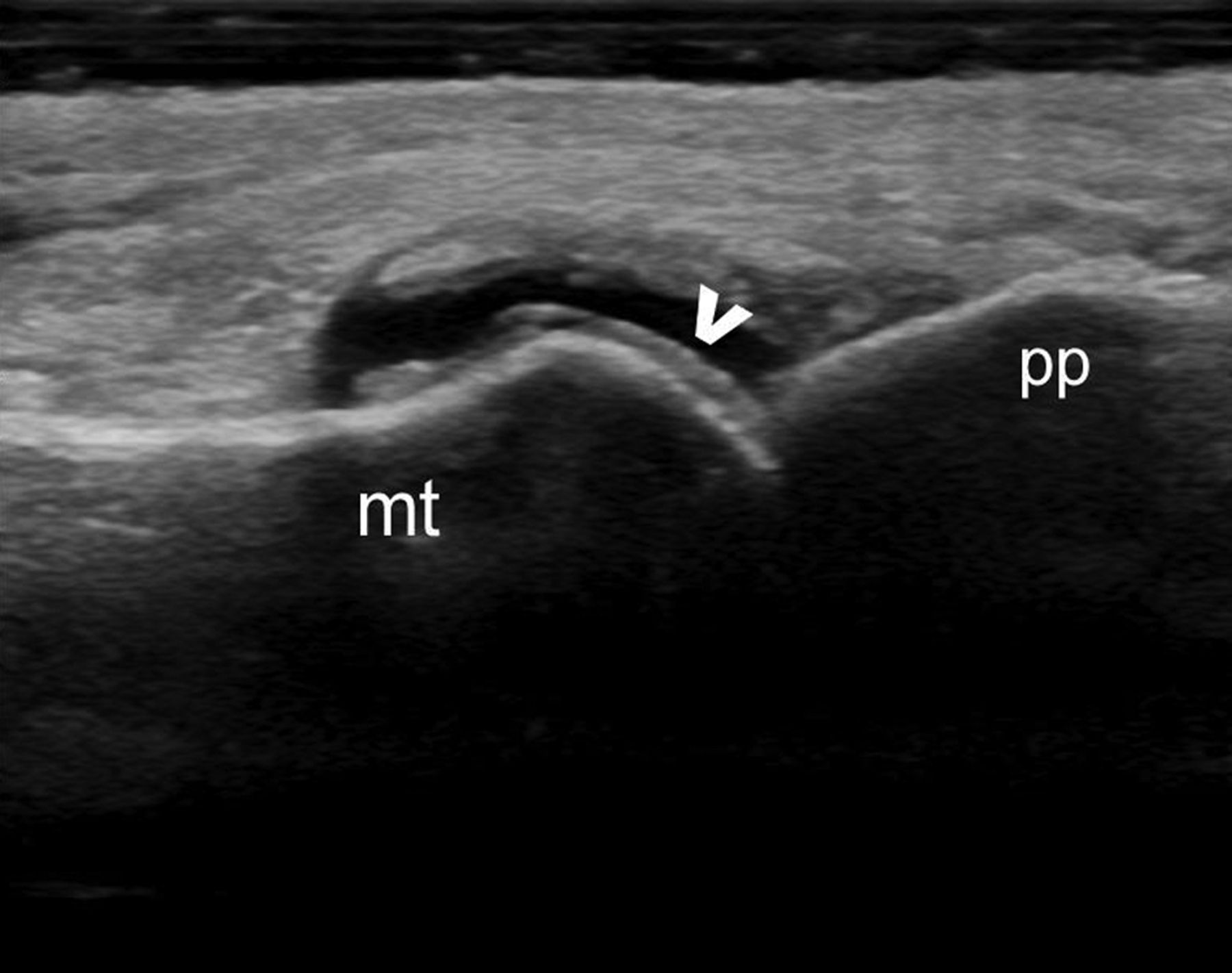
Longitudinal US image of the dorsal aspect of the first metatarsophalangeal joint. Hyperechoic irregular enhancement of the chondrosynovial margin of the cartilage (ie, double contour sign) (arrowhead) is detected in the metacarpal articular cartilage. mt, metatarsal bone; pp, proximal phalanx.

Longitudinal US image of the distal aspect of the patellar tendon. Hyperechoic aggregates (arrowheads) with (left side) and without (right side) acoustic shadowing are seen within the tendon. t, tibia.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
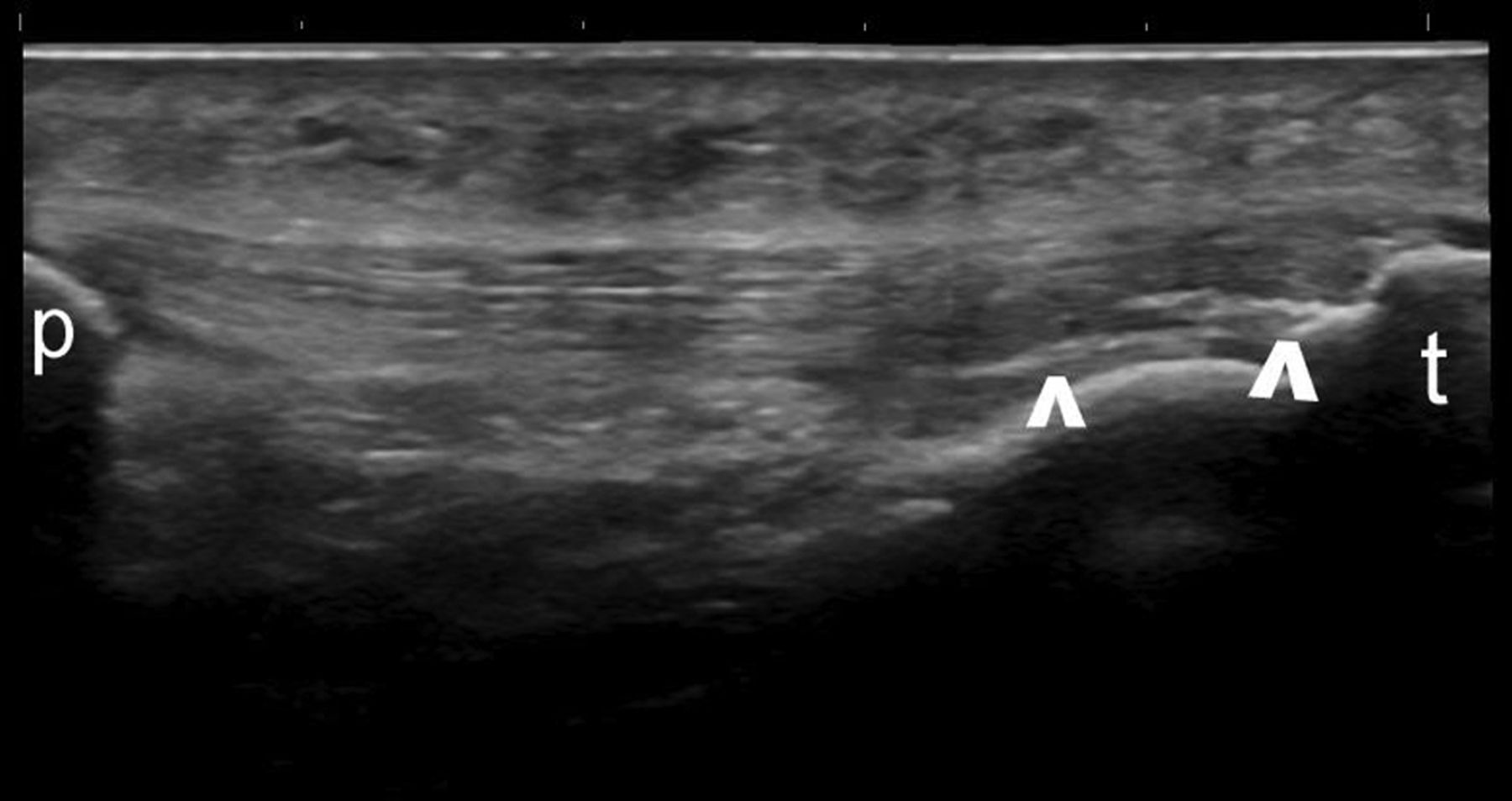
Longitudinal US image of the patellar tendon. Hyperechoic linear bands (arrowheads) within the tendon substance. p, patella; t, tibia.
US findings by anatomic locations in patients with gout versus controls
Online supplementary table S1 shows the distribution of US-detected abnormalities in anatomic locations (ie, unilateral or bilateral) in patients with gout and controls. The first metatarsophalangeal (MTP) and the radiocarpal were the most frequently involved joints for HAGs in patients with gout (57.1% and 38.5% of patients, respectively). The midcarpal and the knee joints were also frequently involved in patients with gout (28.6% and 25.3%, respectively). Tendon abnormalities were most frequently found in the patellar tendon and the triceps tendon in patients with gout (60.4% and 47.3%, respectively), followed by the quadriceps tendon and the Achilles tendon (38.5% and 34.1%, respectively). Articular cartilage DCS was most frequently detected in the dorsal aspect of the first metatarsal head and the femoral condyles (61.5% and 41.8%, respectively). All these abnormalities were detected in a significantly higher percentage of patients with gout than controls (p<0.05).
Diagnostic value of the combination of US abnormalities and anatomic locations
Online supplementary table S2 displays the sensitivity, specificity, positive predictive value and negative predictive value of the comprehensive assessment for each US-detected abnormalities in diagnosing gout, the minimal US assessment of anatomic structures affected by US abnormalities that showed the best balance between sensitivity and specificity, and the minimal assessments that yielded the highest sensitivity and the highest specificity, respectively. The assessment of one joint (ie, radiocarpal joint), two tendons (ie, patellar tendon and triceps tendon), and three articular cartilages (ie, first metatarsal dorsal and plantar cartilage, talar cartilage, and either second metacarpal cartilage (dorsal aspect) or femoral condyle cartilage) showed the best balance between sensitivity and specificity (84.6% and 83.3%, respectively), positive predictive value and negative predictive value (91.7% and 71.4%, respectively). If three joints were added to this model (i.e. midcarpal joint, first MTP joint and knee joint), the sensitivity increased (94.5%) but the specificity decreased (71.4%). The minimal US assessment that showed highest specificity (97.6%) consisted of the patellar tendon and the triceps tendon; however, this assessment showed low sensitivity (46.2%). With regard to tendon US abnormalities, we only considered the presence of HAGs in the above combinations as the presence of only HLBs showed no significant difference between patients with gout and controls.
Microscopic assessment of US findings
Forty-nine (53.8%) patients with gout and eight (19%) controls who consented to the procedure underwent US-guided aspiration of intra-articular HAGs (ie, 30 patients with gout and 6 controls) or tendon HAGs (ie, 19 patients with gout and 2 controls). The aspirated material was positive for MSU crystals in 38 (77.6%) patients with gout and negative in all controls, positive for other crystals in 1 (2%) patient with gout and 1 (12.5%) control (ie, calcium pyrophosphate crystals), and negative for crystals in 10 (20.4%) patients with gout and 7 (87.5%) controls. No patient had complications from the aspiration procedure.
US intraobserver and interobserver reliability
The κ values for the interobserver concordance in the first and second rounds were 0.74 (p<0.0005) and 0.69 (p<0.0006) for the cartilage DCS, 0.50 (p<0.0005) and 0.54 (p<0.0006) for intra-articular/intrabursal and tendon/ligament HAGs, and 0.35 (p<0.0005) and 0.36 (<0.0006) for tendon HLBs, respectively. Global interobserver κ values were 0.52 (<0.0005) for the first round and 0.52 (p<0.0005) for the second round. The mean κ values for the intraobserver concordance were 0.88 (p<0.0005) for the cartilage DCS, 0.67 (p<0.0005) for intra-articular/intrabursal and tendon/ligament HAGs, and 0.70 (p<0.0005) for tendon HLBs. The global intraobserver κ value was 0.75 (p<0.0005).
Discussion
US may play an important role in different aspects of gout, such as differential diagnosis between gout and other arthritis in intercritical periods and/or in patients with normal uricemia,33 the decision-making process regarding the indication of urate-lowering therapy based on the presence of thopi,6 the monitoring of therapeutic response, and the identification of MSU crystal deposit that can be aspirated for definite microscopic diagnosis of the disease.
To the best of our knowledge, this is the first study that has comprehensively assessed US-detected abnormalities described in gout and has tested the diagnostic value of the different combinations of US abnormalities and target anatomic locations in upper and lower limbs. Although lower limb joints are most frequently involved in acute attacks, a relevant frequency of MSU deposition in the upper limbs of patients with gout (ie, 40–50%) has been reported with DECT, a recently developed technology able to detect uric acid deposits in the body.34
Our gout population was representative of the actual spectrum of patients who attend general practitioners or rheumatology outpatient clinics. They had a wide range of disease duration and number of gout attacks per year. Some patients with gout had received urate-lowering therapy in the previous year while others had not. As expected,10 ,35 patients with gout had significantly higher serum urate level, BMI, and alcohol consumption. However, patients with gout and controls were similar in other demographics, occupational musculoskeletal demand and laboratory parameters.
We studied the principal US abnormalities described in the literature10–16 22–31 and those observed by the authors in their practice in patients with gout. We did not investigate the finding called ‘snowstorm appearance’ (ie, presence of hyperechoic spots floating within synovial fluid)23 because it has been described in acute gouty arthritis and seems to be non-specific for gout.25 ,31 In addition, we did not assess the presence of synovial effusion, synovial hypertrophy or synovial Doppler signal because these US findings are frequently found in any type of inflammatory arthritis.10 ,13
As previously reported,10–15 we found a high prevalence of individual US abnormalities in patients with gout and this prevalence was significantly higher in patients with gout than in controls. The anatomic locations most frequently involved with synovial and cartilage US abnormalities in patients with gout were the wrist, the knee and the first MTP joint. Tendon involvement, particularly patellar tendon, triceps tendon and Achilles tendon was also relevant.
A wide range of sensitivity (eg, 21–92%) with very high specificity (eg, 98–100%) for US-detected intra-articular tophi and the cartilage DCS in diagnosing gout have been reported in the literature.10 ,12 ,14 ,15 It should be noted, however, that the different designs and methodologies (eg, joints assessed, blinding, retrospective vs prospective, treated vs untreated patients with gout) of the above studies make it difficult to compare their results. When we tested different combinations of US abnormalities and anatomic locations, we obtained some interesting results. The assessment of only two bilateral tendons, the patellar tendon and the triceps tendon, showed a very high specificity (98%) and positive predictive value (98%) for diagnosing gout. As the sensitivity of this reduced assessment was low, we suggest that the additional US bilateral assessment of one joint (ie, radiocarpal) and three articular cartilages (ie, first metatarsal, talar, and second metacarpal or femoral condyle) can show a well balanced and acceptable sensitivity (85%), specificity (83%), positive predictive value (92%) and negative predictive value (71%) for diagnosing gout. In addition, if sensitivity needs to be prioritised over specificity, the additional scanning of three joints (ie, midcarpat, first MTP and knee) can show a very high sensitivity (95%).
In any case, the sensitivity yielded by the 12-structure US assessment (ie, bilateral radiocarpal joint, first metatarsal cartilage, talar cartilage, second metacarpal or femoral condyle cartilage, patellar tendon and the triceps tendon) was higher than that reported in several studies36–39 in which MSU crystals were identified in synovial fluid aspirated from asymptomatic joints during intercritical periods in 70% of patients with gout. In addition, the absence of invasiveness, adverse effects and complications of US should be weighed against the puncture of asymptomatic joints.
Despite the absence of history of gout or hyperuricaemia as inclusion criteria for controls, we found US abnormalities in control patients and healthy controls. The prevalence of US abnormalities in controls was higher than that reported in some studies.10 ,12 ,15 This result may have several interpretations. According to the results of the US-guided aspiration of HAGs in controls, these US abnormalities seemed to be other crystal deposition (ie, one control) or simply false positives of US (ie, seven controls). The fact that we did not aspirate synovial fluid from controls to demonstrate the absence of MSU crystals, as Ottaviani et al15 did, may suggest that some of our controls actually had MSU crystal deposits or asymptomatic gout. Moreover, the different design and methods of the above studies, such as retrospective nature12 or non-blinding of the main US examiner 15 could have contributed to these discrepancies in the presence of US abnormalities in controls.
Besides demonstrating a good balance between sensitivity and specificity, the 12-structure US assessment can be feasible in clinical practice. Peiteado et al40 reported that a 6-min US assessment of four joints (ie, bilateral knee and first MTP joints) showed a prevalence of 97% of two US abnormalities (ie, hyperechoic cloudy areas and cartilage DCS) in 29 patients with gout. However, these authors did not assess controls, therefore specificity was not obtained.
Although we did not perform US-guided puncture in all patients with gout and controls, aspirated material from HAGs was positive for MSU crystals in a high percentage of patients with gout (78%) and negative for MSU crystals in all controls. The frequency of MSU crystals in aspirated HAG from patients with gout was slightly lower than that reported by Perez-Ruiz et al16 who detected MSU crystals in 83% of US-guided aspiration from US nodules suspected of being tophi in 12 out of 20 patients with gout who agreed to undergo this procedure. Nevertheless, as tophi are composed of a core of MSU crystals embedded in connective tissue,8 the negativity of the puncture cannot rule out the presence of MSU crystals in the lesion.
Consistent with the findings of previous studies,10–12 ,14 ,15 ,29 ,40 we found good to excellent intraobserver agreement and moderate to good interobserver agreement for the presence of US-detected gout abnormalities. Interobserver agreement was fair only for the presence of tendon hyperechoic linear bands, which were excluded from the analysis of a combination of US abnormalities because this finding showed no significant difference between patients with gout and controls.
Some limitations to our study should be noted. We did not assess intraobserver and interobserver reliability for US acquisition but only for image interpretation, However, the ultrasonographer investigators had an extensive common training in musculoskeletal US and specific training focused on gout US abnormalities prior to the study. Moreover, the concurrent validation process was biased for ethical reasons because we performed only US-guided aspiration of HAGs in patients who accepted this procedure.
In conclusion, our results suggest that US bilateral assessment of one joint (ie, radiocarpal), three articular cartilages (ie, first metatarsal, talar, and second metacarpal or femoral condyle) and two tendons (ie, patellar tendon and triceps tendon) may be valid for diagnosing gout with acceptable sensitivity and specificity. Future studies should confirm our results in other gout populations.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online tables
Footnotes
-
Handling editor Tore K Kvien
-
Contributors Study design: EN, EP, MJ-P, JU. Acquisition of data: EB, EB, SC, FJC, MJ-P, AM, MJM, IM, EN, AR, JS, JU, EV. Analysis and interpretation of data: EN, EP, JU, JG. Manuscript preparation: EN, JU, EP. Statistical analysis: JG.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Hospital Universitario Severo Ochoa, Hospital Universitario de Móstoles, Hospital Puerta de Hierro, Hospital Universitario de Alicante Hospital de la Princesa, and Hospital Ramón y Cajal.
-
Provenance and peer review Not commissioned; externally peer reviewed.