Article Text

Abstract
Aims Topical ciclosporin A (CsA) is a therapeutic option for dry eye disease (DED) to control ocular surface inflammation and improve tear function. The aim of this study is to systematically review data from randomised clinical trials (RCTs) evaluating efficacy and safety of topical CsA treatment for DED.
Methods Articles published up to December 2012 were identified from Medline, Embase and the Cochrane Controlled Trials Register. A total of 18 RCTs that evaluated the efficacy and safety of different topical CsA formulations for the treatment of DED were selected according to the set criteria. The Jadad score was calculated to assess RCT quality.
Results The mean Jadad score of the included RCTs was 2.8±0.6. All CsA formulations proved safe for the treatment of DED. Symptoms improved in 100% (9/9) RCTs, tear function improved in 72% (13/18) RCTs and ocular surface damage was ameliorated in 53% (9/17) RCTs in patients with DED. No improvements with CsA treatment versus control were observed in DED resulting from surgical procedures, contact lens use and thyroid orbitopathy. Statistical comparison of CsA efficacy through a meta-analysis of data was not possible due to a lack of standardised criteria and comparable outcomes among studies.
Conclusions Although topical CsA appears to be a safe treatment for DED, evidence emerging from RCTs is limited, and this affects the strength of recommendations to healthcare providers and policymakers for optimal management. Standardised diagnostic criteria to assess the efficacy of topical CsA are recommended to improve the design of future RCTs in DED.
- Cornea
- Conjunctiva
- Clinical Trial
- Immunology
- Ocular surface
Statistics from Altmetric.com
Introduction
Dry eye disease (DED) is estimated to affect between 5% and more than 30% of the worldwide population at various ages, with very high socioeconomic costs and a substantial burden with regard to the quality of life of patients.1 ,2 The management of patients with DED requires the use of tear substitutes to protect the ocular surface from desiccation and damage and, in more severe cases, anti-inflammatory or immunosuppressive treatments to control ocular surface inflammation.3 However, while DED diagnosis has seen several technological advancements in recent years, novel therapeutic options proven to be safe and effective in clinical trials are facing more difficulties to be widely accepted. For instance, topical steroids remain a hallmark of DED treatment in spite of their long-term side effects such as cataract formation and glaucoma. However, the use of topical ciclosporin A (CsA) in patients with DED, which is not limited by long-term ocular side effects, remains relegated to some countries due to the lack of market availability.
Ciclosporin A is a fungal antimetabolite used as an anti-inflammatory drug due to its ability to inhibit interleukin 2 (IL-2) activation of lymphocytes.4 It is used systemically to prevent rejection of various solid-tissue transplants. From the 1980s onwards, several reports have highlighted that topical CsA can be used to treat a variety of ocular inflammatory conditions including DED, high-risk corneal transplants, autoimmune uveitis and vernal keratoconjunctivitis.5 Nevertheless, CsA has been approved only by the US Food and Drug Administration (FDA), and only for use in patients with moderate-to-severe DED. One problem in assessing CsA treatment effects in DED is that no meta-analyses are available to provide recommendations on which CsA eyedrop formulation is more effective in different DED populations.
In the present report, we systematically reviewed the results of all randomised clinical trials (RCTs) on safety and efficacy of topical CsA in patients with DED. Specifically, all CsA eyedrop formulations, ranging from 0.05% to 2% concentration, including emulsions, oil and oil-in-water preparations, and all DED types were revised to understand the potential role of CsA in DED management via an evidence-based approach.
Materials and methods
Literature search
Six observers, divided in three groups of two, independently performed a literature search of all publication years up to December 2012. The articles were identified through a computerised search for clinical trials in the Cochrane Controlled Trial Register (CENTRAL/CCTR, which contains the Cochrane Eyes and Vision Group trials register) on the Cochrane Library, Medline and Embase. The search strategy was used to identify RCTs, as recommended by the Cochrane Collaboration.
The following search strategy was used:
-
Publication type: clinical trial.
-
Keywords/search terms for disease were: eye and dry*, ocular and dry*, explode dryness/all subheadings, tear*, xerophtalmi*, keratoconjuncti* and sicca, Sjogren* or Sjögren* and syndrome.
-
Keywords/search terms for medications were: topic* or topical and eye* and/or ophthalmi*, emulsi* and eye, immuno* and immunosuppressive, cyclosp*, cyclosporine/all subheadings.
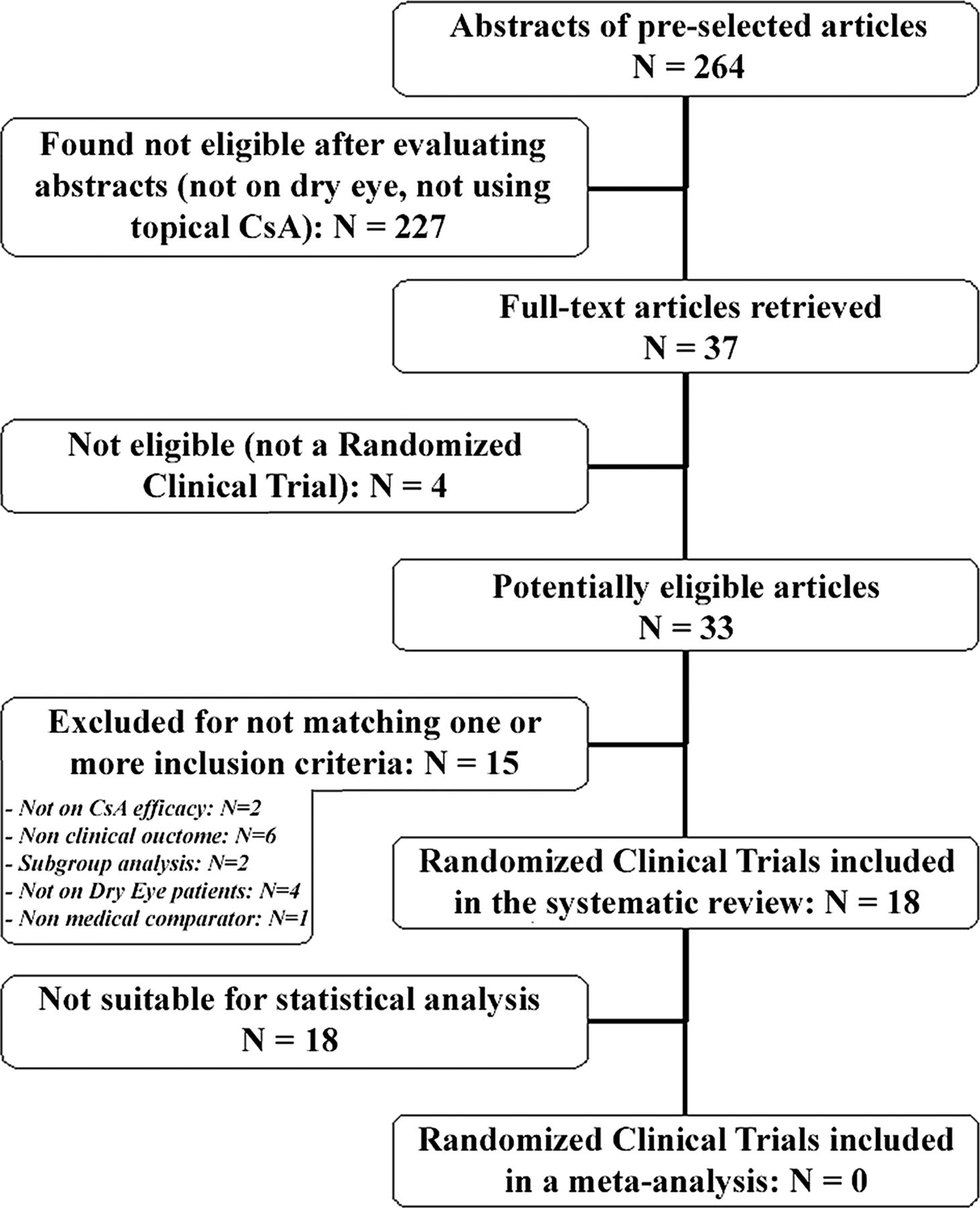
In addition, linked references in all relevant articles were searched. The search resulted in a total of 264 abstracts.
Inclusion and exclusion criteria
Articles potentially eligible for inclusion in this meta-analysis were RCTs on topical CsA treatment for DED published up to December 2012, written in English, French, German, Italian, Portuguese or Spanish. Additional inclusion criteria for the trials were: follow-up of at least 4 weeks and participants ≥18 years old with a diagnosis of DED (at least one of the following inclusion criteria: (i) symptoms of ocular dryness; (ii) reduced Schirmer and/or tear film break-up time (TF-BUT) test; (iii) ocular surface staining), without restrictions of gender or ethnicity. Only medical cointerventions applied topically were considered.
This review focused on the following clinical outcomes: subjective report of symptomatic improvement, ocular surface staining, tear function tests (Schirmer test and TF-BUT test), change in the frequency of artificial tear use, tear film osmolarity, Ocular Surface Disease Index (OSDI) score and safety parameters (ocular and systemic adverse events). Articles were excluded if they did not satisfy one or more inclusion criteria, or if they were irretrievable after performing all available search strategies, including request to authors and editors.
The eligibility of an article was initially determined by evaluating the title, abstract and MeSH (medical subject headings) data. A team of 4 observers divided into 2 groups of 2 examined all 264 retrieved abstracts to consider their eligibility. After matching the decisions of the 2 groups, 227 articles were immediately excluded because they were either not randomised, not on topical CsA treatment or they were related to different kinds of ocular disease. The remaining 37 complete articles were obtained and printed to identify whether they were suitable for inclusion in the revision and distributed to 4 researchers also randomly divided into 2 groups of 2. The observers were blinded to the names of the authors and institutions, the name of the journals, the sources of funding and the sponsors of the studies. The observers of each group were also blinded to the decisions of the other group and trial selection was matched between them. In all, 19 trials were excluded because they did not match 1 or more of the inclusion criteria.
All 18 remaining RCTs were included in the systematic review (figure 1).
{kind=link}
Decision tree of randomised clinical trial selection for inclusion in the systematic review and meta-analysis.
Data collection and analysis
An evaluation of trial quality based on trial design was conducted using the Jadad scale.6 ,7
This scoring system is based on a 3-point questionnaire in which each question has to be scored with ‘YES’ (1 point) or ‘NO’ (0 points). The questions to be addressed were the following:
-
Was the study described as randomised?
-
Was the study described as double blind?
-
Was there a description of withdrawals and dropouts?
Based on the method of randomisation and blinding used in the trials, an additional 2 points may be given, resulting in a final score ranging from 0 (poor quality) to 5 (excellent quality). Specifically, 1 additional point is given if: for question 1, the method to generate the sequence of randomisation was described and it was appropriate (table of random numbers, computer generated, etc.); for question 2, the method of double-blinding was described and it was appropriate (identical placebo, active placebo, dummy, etc.).
It is generally accepted that studies with Jadad scores of ≥3 reflect ‘good’ reporting quality, whereas ratings of <3 reflect qualitatively poorer studies, impacted by a lower internal validity.
Outcome measures
The primary outcome of this systematic review was the evaluation of the efficacy of topical CsA treatment on DED by subjective report of symptomatic improvement within 4 weeks post treatment. Since timepoints for outcome assessments vary appreciably by trial, we considered other timepoints as reported in included studies.
Secondary outcomes of this study included: (i) ocular surface staining as defined by the mean values in total rose bengal or fluorescein or lissamine green scores from baseline to follow-up; (ii) aqueous tear production as measured by the mean values in Schirmer I test (without anaesthesia) or Schirmer II test (with anaesthesia) scores (mm/5 min); (iii) tear film stability as measured by the mean values (in seconds) of TF-BUT; (iv) change in the frequency of artificial tear use; (v) mean values in OSDI score; and (vi) safety parameters (ocular and systemic adverse events).
Statistical analysis
RevMan5 software was used to analyse the data. We tested the heterogeneity between studies using the χ2 test, with significant heterogeneity (p<0.05) precluding meta-analysis.
Results
The 18 studies included in the systematic review dated from 1993 to 2012; all of the studies were published in ophthalmic journals.8–25 A total of 5 trials were performed in Europe, 2 in Asia and 11 in America. There were seven multicentre studies, and all were RCTs. In all, 15 studies were double masked or single (investigator) masked, and 3 were unmasked. Nine studies were sponsored by a pharmaceutical company (table 1). Based on the study design, the trials under examination scored a mean 2.8±0.6 points according to the Jadad scale. Specifically, none of the trials scored 0 points or 1 point, 5 trials (27.8%) scored 2 points, 11 trials (61.1%) scored 3 points and 2 trials (11.1%) scored 4 points; none of the trials fulfilled all the established criteria of proper clinical trial design and scored 5 points (table 2).
Study design and characteristics of randomised clinical trials included in the systematic review
Total Jadad score of randomised clinical trials included in the systematic review
A total of 2479 patients with DED were enrolled in these studies. Mean age was 52.4 years old. The mean follow-up was 5.4±3.6 months. Only six trials specified the washout period, with a mean washout from previous treatments of 1.5 weeks (tables 1 and 3).
Of the 18 included studies, 5 evaluated CsA efficacy in specific DED populations: 1 study included patients with severe trachomatous dry eye, 1 study included contact lens wearers, 1 study included patients with thyroid orbitopathy, 1 study included only patients with Sjögren's syndrome (SS) while 3 studies included SS and non-SS patients with DED and 1 study included patients with dry eye before a laser-assisted in situ keratomileusis (LASIK) procedure. Of the remaining 13 RCTs included in this systematic review, 2 studies included patients with DED who had already been previously treated with CsA eyedrops and 1 study included patients with DED refractory to conventional treatments. Three RCTs enrolled patients with moderate-to-severe DED, and seven studies included patients with DED without specifying type or severity of the disease (table 3).
Characteristics of study populations in the randomised clinical trials (RCTs) included in the systematic review
All studies included in this systematic review evaluated efficacy and safety of different CsA formulations. A total of 10 studies evaluated a CsA 0.05% ophthalmic emulsion versus placebo or vehicle or artificial tears: 1 study in 60 patients for 6 months;13 2 studies evaluated CsA 0.05% in 74 patients for 12 months,20 and in 50 patients in a 12-month extension trial;22 1 study in 233 patients for 2 months;19 1 study in 42 patients for 16 weeks;21 1 study in 47 patients versus vehicle (n=47) or tofacitinib (n=233) for 8 weeks;24 1 study in 21 patients having LASIK who started treatment 1 month before surgery and discontinued it for 48 h post LASIK and then resumed it for additional 3 months;12 1 study in 44 contact lens wearers for 3 months;14 1 study in 45 patients with thyroid orbitopathy for 6 months;17 and 1 study in 64 patients with trachoma for 6 months.15
A total of 3 additional studies used CsA 0.05%: 1 used a 0.05% CsA ophthalmic emulsion versus placebo comparing the result to a topical vitamin A treatment in 150 patients;16 1 evaluated CsA 0.05% ophthalmic emulsion twice a day versus once a day in 100 patients for 24 weeks;23 and 1 study evaluated CsA 0.05% in oil in 51 patients for 12 weeks.25
Among the RTCs on CsA 0.05%, eight studies used the commercially available CsA eyedrops Restasis.12 ,13 ,15–17 ,20 ,21 ,23
Laibovitz et al8 evaluated safety and efficacy of CsA 1% ophthalmic corn oil ointment treatment versus vehicle in a crossover study of 26 patients for 14 weeks, and Gunduz and Ozdemir9 evaluated a CsA 2% in olive oil eyedrop formulation versus vehicle in 30 patients for 2 months.
A total of 3 studies evaluated CsA at different concentrations: Baiza-Duran et al evaluated 0.05% and 0.1% CsA in aqueous solution as compared to vehicle in 183 patients for 14 weeks, Sall et al compared 2 concentrations (0.05% and 0.1%) of a CsA ophthalmic emulsion versus vehicle in 877 patients for 6 months and Stevenson et al evaluated 4 different concentrations (0.05%, 0.1%, 0.2% and 0.4%) of a ciclosporin A oil-in-water formulation versus vehicle for 3 months in 162 patients.10 ,11 ,18
Ciclosporin was compared to artificial tears in eight studies and to vehicle in eight studies. One study compared CsA twice a day to CsA once a day, and one study compared CsA to retinol palmitate or no treatment (table 1).
Nine studies included in this review evaluated ocular symptoms and/or total symptom score as clinical outcomes of treatment efficacy (table 4). All reported a significant amelioration of at least one ocular symptom with CsA eyedrop treatment8 ,10 ,11 ,13 ,15 ,16 ,18 ,19 ,24 (see online supplementary table). However, in seven of these trials, CsA treatment induced no amelioration of at least one symptom.8 ,10 ,11 ,13 ,16 ,18 ,19 Specifically, burning/stinging, foreign body sensation and photophobia were evaluated in six RCTs showing no improvement in 100%, 50% and 83%, respectively.8 ,10 ,11 ,13 ,16 ,18 ,19 No improvement was also observed in itching (evaluated in four RCTs),8 ,10 ,11 ,13 pain and tearing (evaluated in two RCTs)8 ,10 ,11 ,18 and mucous secretion (evaluated in one RCT).8 CsA treatment showed improvement of blurred vision in three out of four RCTs evaluating this symptom8 ,10 ,13 ,16 and dryness in two out of five RCTs.10 ,11 ,13 ,18 ,19
Outcome measures of the clinical trials included in the systematic review
Two trials used the same scale from 0–4 to evaluate ocular discomfort by considering the following symptoms: stinging/burning, itching, sandiness/grittiness, blurred vision, dryness, light sensitivity, pain or soreness.10 ,11 Sall et al used a similar scale but without photophobia.13 Chen et al evaluated dryness, foreign body sensation, photophobia and burning in a similar 0–4 scale.19 Kim et al evaluated subjective symptoms in a 0–4 scale without specifying which symptoms were assessed.16
The other trials used different scales to evaluate symptoms. Specifically, Laibovitz et al assessed symptoms by using patients’ diaries (itching, burning, redness, tearing, blurred vision, nasal dryness, sensitivity to light, foreign body sensation, mucous production, limitation of daily activities, mouth dryness and overall symptoms) rated from 0–3.8 Baiza-Duran et al evaluated dryness, burning, photophobia, tearing, ocular fatigue and foreign body sensation on a scale from 0–3.18 Willen et al evaluated a total symptoms score by the sum of foreign body sensation, burning/stinging, ocular fatigue, photophobia graded from 0–3.14 Guzey et al evaluated the presence of a total symptom score with a 0–12 point scale based on each of 4 symptoms (foreign body sensation, burning, ocular fatigue, photophobia) graded from 0–3.15
All 18 studies evaluated tear function by Schirmer test. Specifically, the type I Schirmer test (without anaesthesia) was performed in eight trials.9 ,11 ,13 ,16 ,18 ,19 ,21 ,22 The type II Schirmer test (with anaesthesia) was used in seven trials.12 ,14 ,15 ,17 ,20 ,23 ,25 Two studies used Schirmer I and II tests.10 ,24 The study by Laibovitz et al did not specify which Schirmer test was used.8
Schirmer I scores significantly improved from 0.13 to 3 mm/5 min with CsA in six trials.10 ,16 ,19 ,21 ,22 ,24 Schirmer II scores significantly improved from 2.5 to 6.17 mm/5 min with CsA in five trials,10 ,15 ,20 ,24 ,25 a finding confirmed by all but the Altiparmak et al study where the placebo group showed a significant amelioration when compared to the CsA group17 (table 4 and see online supplementary table).
All studies except Salib et al evaluated TF-BUT.12 A significant amelioration of TF-BUT with CsA was described in eight trials with a range from 1.02 to 9.88 s,9 ,15 ,16 ,20–23 ,25 confirmed by all but the study by Altiparmak et al in which a significant amelioration was observed in the placebo group when compared to CsA.17 No significant differences were observed in the other RCTs (table 4 and see online supplementary table).
Ocular surface staining assessed by either fluorescein, rose bengal and/or lissamine green was evaluated in 17 trials with amelioration from −0.11 to −3.05 with CsA in 9 trials8–10 ,15 ,16 ,19–22 (table 4 and see online supplementary table).A total of 11 studies evaluated the OSDI questionnaire score,10–12 14–16 ,20 ,22–25 with a significant amelioration with CsA in 6 trials11 ,15 ,20 ,22 ,24 ,25 (table 4 and see online supplementary table).
Five RCTs assessed patients’ need to use artificial tears, showing an overall reduction in the frequency of use.10 ,11 ,19 ,22 ,24 However, only Sall et al demonstrated a significant improvement in CsA versus vehicle10 (table 4 and see online supplementary table).
One trial evaluated patients’ quality of life using the National Eye Institute Refractive Error Quality of Life instrument-42 (NEI-RQL-42) questionnaire, and showed no significant changes following CsA treatment.14
A total of 16 studies evaluated safety parameters and adverse events,8–13 ,15 ,16 ,18–25 with no trial reporting serious adverse event with the treatments evaluated (table 1).
Since most of the included RCTs used different scales, timepoints, and CsA formulations and concentrations for assessing different outcome measures, statistical comparison of CsA efficacy through a meta-analysis of data was not possible.
Discussion
This systematic review analysed the results of RCTs that aimed at evaluating topical CsA for the treatment of DED.
Ciclosporin A ophthalmic emulsion has been proposed and approved by US—but not European—regulatory agencies in patients whose tear production is presumed to be suppressed due to ocular inflammation. From the results of this systematic review, we can conclude that the use of CsA as an anti-inflammatory treatment for dry eye is safe as it has not demonstrated serious ocular or systemic adverse effects.
As for CsA efficacy in terms of clinical outcomes, the results of included trials are quite heterogeneous, and do not allow us to definitely state that CsA is effective in patients with DED.10 ,11 ,18–25 Additionally, when CsA is used in other conditions associated with dry eye, such as post surgery, contact lens use, thyroid orbitopathy or trachoma, the beneficial effects are not confirmed except for trachomatous dry eye, highlighting that further studies are needed to identify the subpopulations that could benefit from CsA.12 ,14 ,15 ,17 Although the Jadad mean score of RCTs included in this review was of 2.8±0.6 points, 13 out of the 18 included studies showed a score higher than 3 points, indicating a good quality.
Among the RCTs evaluating topical CsA treatment in patients with DED, there remain several hurdles that do not allow us to draw conclusions fostering an evidence-based approach to DED management: specifically, we were unable to conduct a meta-analysis because of the clinical heterogeneity observed between studies. Different outcomes, different scales for the evaluation of results and different timepoints of outcome evaluation resulted in it being impossible to describe a summary effect for any of the treatments included in this review and, therefore, in a lack of evidence supporting the recommendation of one specific concentration, formulation or dosage of CsA for treating DED. Specifically, the results of this systematic review do not allow us to answer to the most common clinical questions on the use of CsA in dry eye, such as if there are some advantages to using CsA together with artificial tears or CsA alone, what is the most effective concentration in DED management, or what is the best topical CsA formulation.
Another issue that may be responsible for the differences among studies that did not allow us to perform a meta-analysis of data is the variation in clinical presentation of patients with DED recruited in the RCTs, which are often mixed populations of patients including patients with Sjögren's dry eye, patients with non-Sjögren's dry eye and patients with evaporative dry eye of different severities. Such variability inevitably results in different evaluations of treatment effects. Another common issue in RCTs for DED relates to the standard outcome measures used (such as Schirmer test, TF-BUT, vital staining) that have limited sensibility and specificity and are not repeatable. In order to pursue the goal of a homogeneous patient population in a chronic disease such as DED, it may be useful to replace high expectations for the perfect medical intervention allowing treatment to ultimately resolve the disease state, with less exciting but still useful outcomes. It will be also important for clinical trials in DED to randomise patients with similar aetiologies and clinical stages, as there could be a different response to various therapeutic procedures during the course of this chronic disease among different patients.26
In summary, evidence emerging from RCTs on topical CsA for DED published so far supports that it is a safe treatment but their heterogeneity affects the strength of recommendations to healthcare providers and policymakers for optimal management. It is likely that future clinical and epidemiological studies will provide more definitive recommendations about the timing, efficacy and relative costs/benefits of anti-inflammatory treatment with CsA for dry eye.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors All authors contributed to the paper by searching and identifying clinical trials included in the systematic review, writing and critically evaluating the manuscript as well as making figures and tables. MS and FM also contributed to the study design and statistical analysis.
-
Funding This work was supported by Italian Drug Agency (AIFA) FARM8ACX7M research grant.
-
Competing interests SB is a medical consultant for Allergan; AL is a medical consultant for Dompé.
-
Provenance and peer review Not commissioned; externally peer reviewed.