Article Text

Abstract
Background Psoriasis is a skin disease with also systemic involvement: its impact on the eye is not well established and often clinically underestimated. Aim of this study was to investigate the presence of ocular discomfort symptoms and of ocular surface changes in a population of patients with psoriasis.
Methods For this cross-sectional, comparative study, 66 patients with psoriasis were subdivided according to the presence of arthritis and to the use of biological therapy. All patients underwent clinical evaluation with the following tests: Ocular Surface Disease Index Questionnaire, Tearscope examination, meibometry, tear film breakup time, corneal and conjunctival fluorescein staining, Schirmer I test, corneal aesthesiometry, meibomian gland dysfunction (MGD) assessment and conjunctival impression cytology. 28 healthy subjects were also enrolled and treated with the same clinical tests. A statistical analysis of the results was performed.
Results Patients with psoriasis showed a significant deterioration of the ocular surface tests, if compared with healthy subjects, demonstrated by tear film lipid layer alteration, tear film instability, corneal and conjunctival epithelial suffering and mild squamous metaplasia at impression cytology. No differences were found in ocular surface test results of the psoriatic group when patients were divided according to the presence of arthritis, whereas the anti-inflammatory treatment with biological drugs demonstrated a significant improvement of corneal stain and MGD.
Conclusions Our findings suggest that the ocular surface involvement in patients with psoriasis indicates the need of periodic ophthalmological examinations to diagnose the condition and allow a proper treatment, so contributing to the amelioration of patients’ quality of life.
- Tears
- Ocular surface
- Conjuctiva
- Cornea
Statistics from Altmetric.com
Introduction
Psoriasis is an immune-mediated, inflammatory disease affecting the world population with an estimated prevalence of 2%–3% and a negative impact on quality of life.1 An altered gene expression profile is responsible for the production of specific psoriatic phenotypes, determining skin alterations also present in non-lesional areas. This may result in barrier function alteration, contributing to the release of proinflammatory mediators and hence to the maintenance of an inflammatory condition.2 Psoriasis is a chronic disease often presenting with relapses and remissions, and accompanied by manifestations involving also other organs apart from the skin1; therefore, it can be considered a systemic disorder rather than merely a skin disease.
Despite psoriasis is one of the most studied dermatological disorders, its impact on the eye was not well established and is often clinically underestimated. The most recognised ocular complication in course of psoriasis is anterior uveitis, mainly found in association with psoriatic arthritis in human leukocyte antigen-B27 positive subjects.3 It is possibly responsible for significant vision impairment and sometimes with an onset preceding skin manifestations.4 5 Other reported ophthalmic complications of psoriasis, such as blepharitis, conjunctivitis, keratitis and xerosis, were considered as a localisation of psoriatic plaques on the ocular surface structures. However, information about their actual prevalence are limited6 and vary considerably between ophthalmic and dermatological studies.5 Hence, the precise aetiopathogenic mechanisms of ocular surface involvement in psoriasis still need to be clarified; in fact, apart from a direct eye involvement with psoriatic plaques, it may be the consequence of the psoriatic phenotype able to induce immune-mediated inflammatory processes in organs different than skin2 or of iatrogenic complications in course of psoriatic treatments. Whatever the pathogenesis, the chronic suffering of the ocular surface causes tear film impairment and visual disturbance.7
Aim of this study was to investigate the presence of ocular discomfort symptoms and ocular surface changes, with particular regard to tear film alterations, in a population of patients with psoriasis and to compare such changes with a population of healthy subjects.
Materials and methods
Study population
Patients with psoriasis were enrolled, for this cross-sectional, comparative study, at the Dermatology Unit of the University of Messina.
General information about the psoriasis course was carefully gathered, with particular regard to: duration of the disease, presence/absence of joint involvement, past or current therapies, involvement of the face and Psoriasis Area Severity Index (PASI).8
The Institutional Review Board of the Department of Biomedical Sciences of the University of Messina, Messina, Italy, approved the protocol and the study was conducted in concordance with the tenets of the Declaration of Helsinki. Informed consent was obtained from all the participants after explanation of the nature and the possible consequences of the study.
Inclusion criteria were having psoriasis with and without arthritis, both under systemic treatment with biological drugs (antitumour necrosis factor-α and anti-interleukin (IL)-12/IL-23) or not.
Exclusion criteria were having a treatment regimen based on ciclosporin, methotrexate, retinoids or psoralen and ultraviolet A radiation therapy.9 Also people with any eye disorder or history of contact lens use were excluded from the study.
Furthermore, healthy controls were recruited among staff personnel of the hospital. Exclusion criteria were having any eye disorder or history of contact lens wear and use of any topical or systemic drug potentially interfering with the ocular surface health.
Tests performed
The Ocular Surface Disease Index (OSDI) Questionnaire, designed to assess dry eye disease severity in a scale of normal, mild to moderate and severe, was administered to all the subjects included in the study immediately before the ophthalmological examination. It includes 12 questions relating to past week experience with the presence of ocular discomfort symptoms, vision-related functioning and environmental triggers.10 A score ≤12 was considered normal, a score between 13 and 32 indicated mild to moderate dry eye, whereas a score ≥33 indicated severe dry eye.11 12
The ophthalmological examination included ocular surface study, visual acuity assessment, tonometry and fundus examination.
For the ocular surface study, the clinical tests were performed according to the following sequence:
Tearscope examination (Tearscope Plus, Keeler, Windsor, UK). It is a lighting system that allows the non-invasive visualisation of the tear film lipid layer over the whole corneal surface, under a ×16–25 magnification at the slit lamp. The lipid layer patterns are classified, based on their appearance, as previously described.13 Lipid patterns, which are transient or of the open meshwork type, are considered to be of poor efficacy and characteristic of a thin lipid layer (~15 nm). Tight meshwork patterns are evaluated as intermediate in efficacy. Wave, amorphous and colour mixing patterns are characteristics of a thick, stable lipid layer (30–80 nm) and considered optimal.13 The observed lipid layer patterns were graded from 0 to 9, where 0 was the absence of lipids and 9 a very thick lipid layer, based on their appearance as previously described.14
Meibometry for the assessment of the meibomian glands secretion, carried out by the Meibometer MB 560 (Courage + Khazaka electronic, Köln, Germany), evaluated the degree of diaphanisation of an adsorbent tape applied on the central third of the lower lid margin for 10 s. After a waiting period of 5 min, necessary to allow the evaporation of the aqueous component, the tape was placed in a photometer. The degree of diaphanisation, directly correlated to the amount of lipids present on the eyelid margin, was measured in photometric units.
Tear film breakup time (TBUT) was performed using a wetted fluorescein strip (Bio Glo, fluorescein sodium ophthalmic strips, HUB Pharmaceuticals, Rancho Cucamonga, California, USA), instilling one drop into the lower fornix; the surface was observed at the slit lamp through a cobalt blue filter. The time gap between a blink and the appearance of a dark spot on the cornea was recorded and the mean of three consecutive measurements was reported.15
Ocular surface fluorescein staining: 3 min after TBUT determination, the corneal and conjunctival scores were obtained according to the National Eye Institute/Industry Workshop scoring system.16 For corneal assessment, five areas were considered and, in each area, the staining pattern was graded with a score: 0 (no alterations), 1 (isolated dots), 2 (confluent dots) and 3 (patch of epithelial defect). The global score was obtained by adding the scores of the different areas, with a total score ranging from 0 to 15. For conjunctival assessment, the score was obtained adding a yellow filter (Wratten 12, Eastman Kodak, Rochester, NY, USA) for the observation. Four areas were identified, two nasal and two temporal, for a total score ranging from 0 to 12.
Schirmer I test: a filter paper strip (Alfa Intes Industria Terapeutica Splendore, Casoria, Napoli, Italy) was applied between the outer and the middle third of the lower lid. The length of the wetted part of the strip was measured after 5 min: a wet length <5 mm was considered abnormal.15
Cochet-Bonnet aesthesiometry (Luneau Ophtalmologie, Chartres, France) was performed at the central cornea as previously described.17
Meibomian gland dysfunction (MGD) assessment was performed as previously described.10 Gland drop-out, expressibility and quality of the meibum, shape, degree of vascularisation and the presence of keratinisation of the lid margin were the parameters used to score MGD. The score ranged from 0=normal to 4=severe lid margin alteration. The evaluation was carried out on the lower lid margin.
Impression cytology specimens were collected from the bulbar conjunctiva at the 12 o’clock position, 3 mm from the limbus, using Supor 200 filters (Gelman Sciences, Ann Arbor, Michigan, USA).18 19 The filters were pressed to adhere firmly to the conjunctival epithelium and then were peeled off. The filter paper with the specimen was fixed in 4% paraformaldehyde in phosphate-buffered saline (pH 7.4) for 24 hours and then processed for the periodic acid–Schiff Papanicolaou stain.20 21 The evaluation was carried out according to a previously described scoring system.22 In brief, seven parameters were evaluated: specimen cellularity, cell-to-cell contacts, nucleus/cytoplasm ratio (N/C), nuclear chromatin, goblet cell distribution, keratinisation and presence of inflammatory cells. For each parameter, a score was attributed: 0 for normal pattern, 1 for borderline pattern and 2 for abnormal patterns. A score of 3, only for keratinisation and inflammatory cells presence, was used to indicate severe alterations. A total score was obtained adding the results of each parameter, so that the specimens were classified into three classes: class A (score 0–3) = normal features, class B (score 4–6) = borderline features and class C (score ≥7) = abnormal features.22
Statistical analysis
The MedCalc, V.11.3.0.0, software was used for data analysis. Student’s t-test or Mann-Whitney U test was performed as appropriate; a p value ≤0.05 was considered statistically significant. Main outcome measures were OSDI, Tearscope, meibometry, corneal and conjunctival staining, Schirmer I test, corneal sensitivity, MGD assessment and impression cytology data in patients with psoriasis and controls. Secondary outcome measures were the effects on the ocular surface tests of biological drugs treatment and the presence of arthritis, in patients with psoriasis.
Results
Patients population
In our study 66 patients with psoriasis (33 men and 33 women, mean age 50.7±13.1 years) and 28 healthy individuals (17 men and 11 women, mean age 45.6±16.3 years) were enrolled. The patients with psoriasis were further subdivided according to two criteria:
with or without psoriatic arthritis
using or not using biological drugs (table 1).
Study population
Clinical tests performed
No signs of uveal flogosis, ocular hypertension or retinal damage were found in the patients with psoriasis included in the study.
Comparing the ocular surface of psoriatic patients with controls, statistically significant worst values were found in the patients with psoriasis for the following parameters: OSDI score (p=0.01), lipid film thickness at Tearscope (p<0.0001), TBUT (p<0.0001), conjunctival stain (p=0.02) and MGD score (p=0.0008). Furthermore, a statistically significant difference was also found for corneal stain (p=0.02), Schirmer I tests (p=0.01) and aesthesiometry (p=0.0009), even if the mean values for patients with psoriasis were within normal limits. No differences were found for meibometry (table 2, figure 1A).
Results of clinical tests performed in healthy controls and in patients with psoriasis (also divided in arthritic and not arthritic and in treated and not treated with biological drugs)

Results of clinical tests in healthy controls and patients with psoriasis (A), in arthritic and not arthritic patients (B) and in patients treated and not treated with biological drugs (C). *p < 0.05 vs Controls; †p = 0.03 vs No Arthritis; ‡p < 0.05 vs Biological Treatment.
When considering patients with psoriasis divided according to the presence of arthritis, patients with arthritis had a statistically significant higher score versus non-arthritis patients for corneal stain (p=0.03), which was also statistically significantly different than controls (p=0.01). OSDI, Tearscope, TBUT, Schirmer I test, aesthesiometry and MGD were significantly different versus controls for both groups of patients with psoriasis (table 2, figure 1B).
Dividing patients with psoriasis between those under treatment with biological drugs or not, it was found that among those treated with biological drugs, 23.3% showed ocular surface involvement, while this involvement was observed in the 52.8% of the untreated patients with psoriasis. Untreated patients had significantly worst values for corneal fluorescein stain (p=0.05) and MGD (p=0.01) than treated patients. Furthermore, untreated patients had all parameters, except meibometry, significantly worst than healthy controls, whereas treated patients had significantly different values for OSDI, Tearscope, TBUT, conjunctival stain, aesthesiometry and MGD when compared with healthy controls; corneal stain and Schirmer I tests were not significantly different (table 2, figure 1C).
Impression cytology data
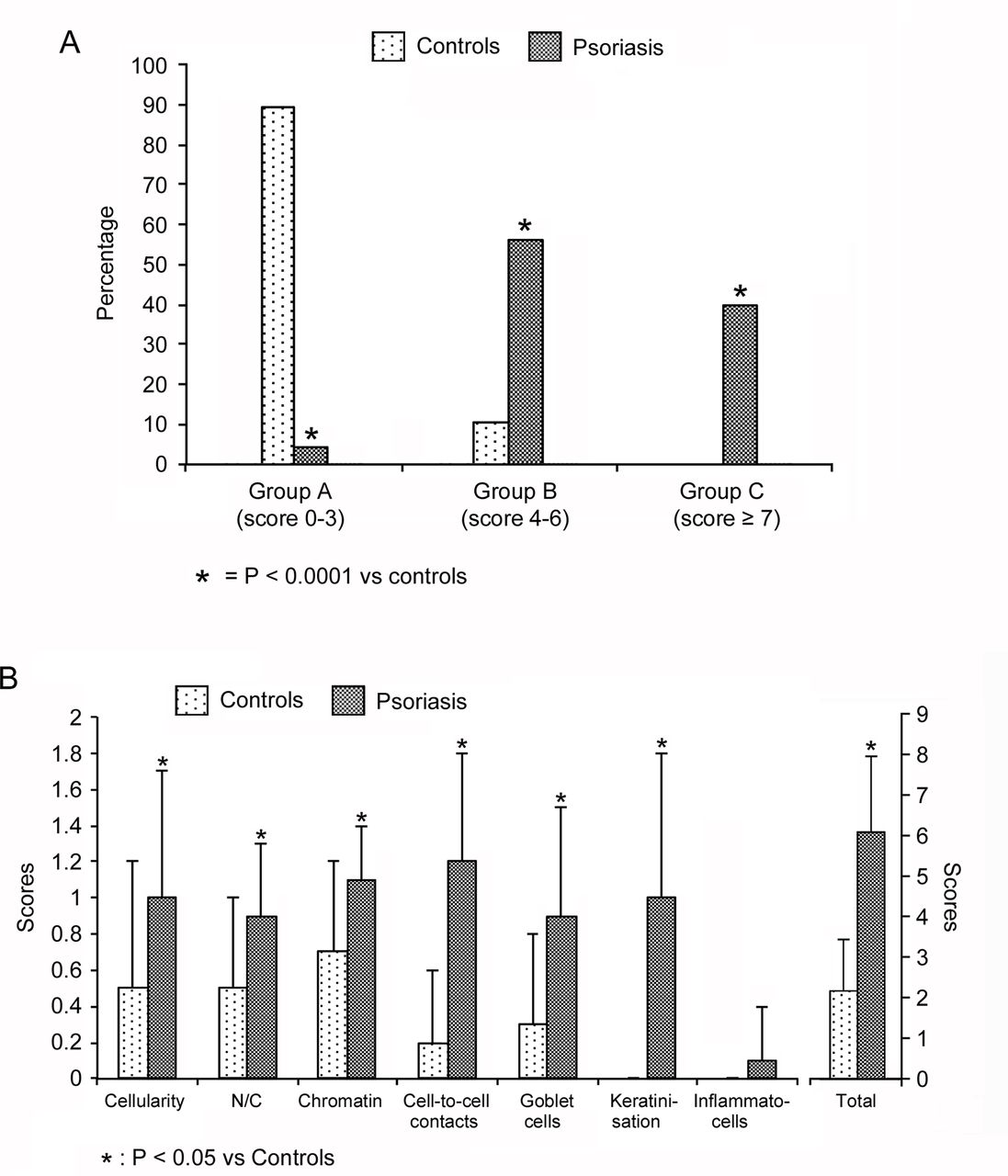
The conjunctival impression cytology showed that, among the patients with psoriasis, 3 were included in group A (score 0–3), 37 obtained a score ranging from 4 to 6 (group B) and the remaining 26 were assigned to group C (score ≥7 which indicates a clearly abnormal aspect of the specimen); healthy controls were mostly included in group A (25 patients with a total score ranging from 0 to 3) while the other 3 were in group B (score 4–6) showing borderline alterations. Considering the general classification of the specimens, a statistically significant difference was found between the two groups (p<0.0001) (figure 2A).

(A) Prevalence of the different classes of impression cytology in healthy controls and patients with psoriasis. (B) Results of the cytological parameters in healthy controls and patients with psoriasis.
Comparing the seven cytological parameters, it was found that patients with psoriasis showed a statistically significant difference for each parameter and for the total score, excluding the presence of inflammatory cells versus controls (table 3, figures 2B and 3).
Results of cytological tests performed in healthy controls and in patients with psoriasis (also divided in arthritic and not arthritic and in treated and not treated with biological drugs).

{kind=link}
{kind=link}
{kind=link}
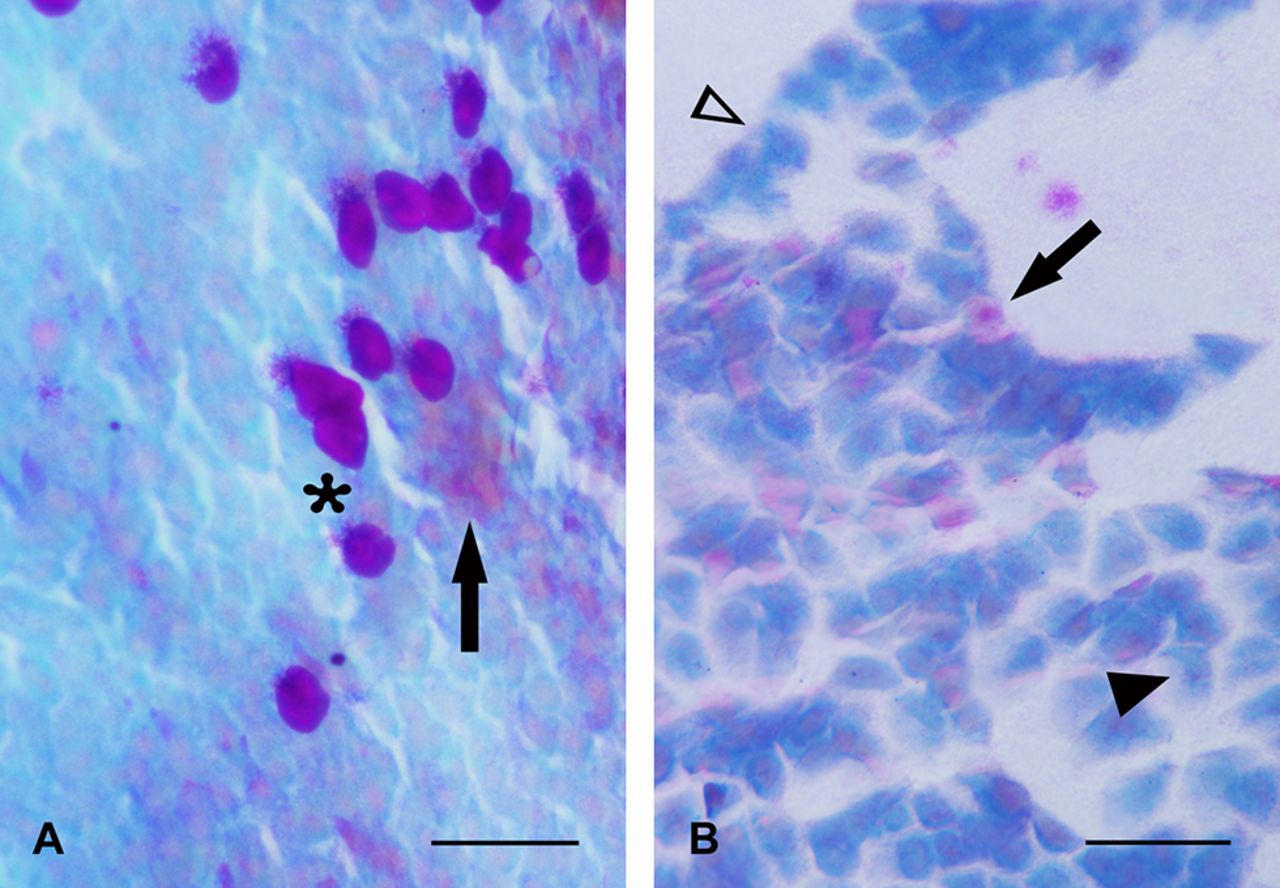
(A) Conjunctival impression cytology specimen from healthy subject. Note the presence of multilayered epithelium with well evident goblet cells (*) and sometimes cells with normal aspect, but faint keratinisation (arrow). (B) Conjunctival impression cytology specimen from patient with psoriasis. The epithelial cells appear isolated, sometimes with a reduced nucleus/cytoplasm ratio (arrowhead) and condensed chromatin (empty arrowhead). Scale bar=50 µm.
Dividing the patients with psoriasis in those having or not arthritis, it was shown that both groups of patients with psoriasis showed a statistically significant difference versus healthy controls, excluding the presence of inflammatory cells. Comparing the two groups of patients with psoriasis, patients with arthritis had a significantly higher cytological score for the goblet cell distribution (table 3).
Furthermore, dividing patients with psoriasis between those treated with systemic biological drugs or not, it was observed that both groups showed a significant difference versus healthy controls for all the parameters studied, with the exception of inflammatory cells presence. No differences could be observed between the two groups of patients, with and without biological treatment (table 3).
Discussion
Previous papers about the ocular surface alterations in patients with psoriasis showed changes limited to few clinical tests,4 23 whereas in the present paper we described the results of several tests, nowadays available, with particular regard to the lipid layer behaviour. Our results give a more complete evaluation of the ocular surface changes also including qualitative and morphofunctional data, that is, qualitative evaluation of the meibum with meibometry and the use of Tearscope for the distribution of the lipid layer on the underlying mucoaqueous layer of the tear film. Furthermore, these evaluations were carried out in patients undergoing biological treatments or not and with psoriatic arthritis or not, giving, in such way, a more detailed analysis of different aspects of psoriasis.
Although as already described in the introduction, patients with psoriasis generally do not complain for any ocular discomfort, some of the results show an ocular surface involvement in the disease, even if mild. Under this aspect, the presence of corneal damage, particularly in subjects with arthritis and without biological treatment, might be clinically significant, as it can be also the case of TBUT, significantly lower than controls. Also MGD may be clinically significant, as indicated by the score. On the other hand the changes of Schirmer test and aesthesiometry although statistically significant do not appear to be clinically relevant, as they are within normal limits.
From our data it appears that patients with psoriasis have an impairment of the ocular surface structure and function. The first striking datum is the evidence that their response to the OSDI Questionnaire demonstrated the presence of an ocular discomfort that could be considered the consequence of a mild/moderate dry eye, although they were not asking for ophthalmological assessment and undervalued the ocular symptoms. This might be the consequence of the attention mainly paid to the socially invalidating skin condition, while mild/moderate symptoms involving different organs and apparently not correlated with the disease were unclaimed and not investigated appropriately. Therefore, clinical conditions like dry eye were largely under diagnosed.
The clinical tests performed were aimed to assess either function or structure of the ocular surface. Among the functional tests, meibometry and Tearscope studying the lipids of the tear film are the less frequently reported in ocular surface studies.
Meibometry provides a quantitative measure of the lipids present on the lid margin and it was used to assess their amount in healthy subjects24 and patients with dry eye.25 In the present study, it was the only parameter that failed to demonstrate a difference between psoriatic and normal subjects. This datum was in accordance with what found in the seborrhoeic areas of psoriatic skin versus controls.2 This result might appear in contrast with the higher MGD presence demonstrated in patients with psoriasis versus controls. However, since the lid margin can be considered structurally a seborrhoeic area, the changes in the amount of lipids determined by a mild/moderate MGD are not sufficient to induce modifications of sebometric values.
The results of the Tearscope Study demonstrated that patients with psoriasis had a thinner tear film lipid layer than controls. The importance of a thick lipid layer to reduce tear evaporation was underlined in previous papers, where the relationship with meibomian glands conditions was also pointed out.13 26 27 The interference patterns observed represent variation in thickness of the lipid film depending on the molecular organisation of the lipid molecules and their relationship with the underlying mucoaqueous subphase of the tear film.28 The evidence that patients with psoriasis showed thinner lipid layer than controls might seem in contrast with the meibometry results, which failed to demonstrate a difference between patients and controls. However, it should be considered that meibometry relates to the quantity of lipids present on the lid margin,25 while the Tearscope accounts for a functional behaviour of the interaction between the lipid layer and the underlying mucoaqueous subphase of the tear film.28
For impression cytology, almost all parameters, excluding inflammatory cells presence, were involved. The parameters more changed were: specimen cellularity, cell-to-cell contacts, nuclear chromatin and presence of keratinisation. The specimen cellularity can be related to cell membrane structural changes and is the consequence of the adhesion between the cell surface and the filter used to harvest the cells; cell-to-cell contacts are the expression of the epithelial intercellular junctions integrity, so that a monolayer of isolated cells could be observed in altered epithelia. The nuclear chromatin is more evident when the cells undergo functional damage. The presence of keratine indicates the anomalous synthesis of intermediate filaments, interfering with cell plasticity. These alterations are the expression of a state of squamous metaplasia that in patients with psoriasis can be classified as mild–moderate.
Regarding the population of patients divided according the presence or absence of arthritis, no differences were found between the two groups; however, both groups showed a statistically significant difference for clinical and cytological parameters versus controls. The only cytological parameter showing a statistically significant difference between the two groups was the goblet cell population, which was reduced in patients with arthritis, so indicating a deeper damage in this group.
As to the possible differences related to the systemic treatment with biological drugs, it was shown that a mild protective effect was obtained by the treatment for the cornea and the MGD, two parameters related to the inflammatory status of the ocular surface. No other differences were found between the two groups.
In conclusion, the ocular surface alterations, occurring in course of psoriasis, although less evident than other accompanying lesions, should be considered and appropriately diagnosed,29 in order to avoid the development of chronic lesions that might be detrimental for the patients’ quality of life.
References
Footnotes
Contributors EA designed the study, performed clinical tests and wrote the paper; LR, EIP and AI performed the tests; RG evaluated patients with psoriasis; SPC contributed to study design and selection of patients with psoriasis; DP contributed to study design and evaluated cytological specimens; PA contributed to the study design, wrote the paper and evaluated all data.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The Institutional Review Board of the Department of Biomedical Sciences of the University of Messina, Messina, Italy.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance