Article Text

Abstract
Objectives Determine if perfluorooctanoic acid (PFOA) is associated with an incident disease in an occupational cohort.
Methods We interviewed 3713 workers or their next of kin in 2008–2011, and sought medical records for self-reported disease. These workers were a subset of a previously studied cohort of 32 254 community residents and workers. We estimated historical PFOA serum levels via a job-exposure matrix based on over 2000 serum measurements. Non-occupational exposure from drinking water was also estimated. Lifetime serum cumulative dose (combining occupational and non-occupational exposure) was our exposure metric. We studied 17 disease outcomes with more than 20 validated cases.
Results The median measured serum level was 113 ng/mL in 2005 (n=1881), compared with 4 ng/mL in the US. Ulcerative colitis (10-year lag) showed a significant trend (p≤0.05) with increasing dose (quartile rate ratios (RRs)=1.00, 3.00, 3.26, 6.57, n=28, p for trend=0.05), similar to earlier findings in the community study. Rheumatoid arthritis (no lag) showed a positive trend in a categorical trend test (RRs=1.00, 2.11, 4.08, 4.45, n=23, p for trend=0.04). Positive non-significant trends were also observed for prostate cancer, non-hepatitis liver disease and male hypothyroidism, which have been implicated in other studies. A significant negative trend was found for bladder cancer and asthma with medication. No marked trends were seen for high cholesterol, which had been seen in the community study.
Conclusions Ulcerative colitis and rheumatoid arthritis were positively linked to PFOA exposure among workers. Data were limited by small numbers, under-representation of hard-to-trace decedents and few low-exposed referents.
Statistics from Altmetric.com
What this paper adds
-
Perfluorooctanoic acid (PFOA) causes tumours, liver inflammation and changes in immunity in rodents. Health effects in humans remain controversial.
-
This is the first cohort study of disease incidence among workers exposed to PFOA; these workers had high level of exposure.
-
We found a positive exposure-response trend for PFOA and ulcerative colitis, with some evidence as well of an increased trend for rheumatoid arthritis; both of these are autoimmune diseases. There was also more modest evidence of positive trends for prostate cancer, male thyroid disease and non-hepatitis liver disease. There were significant negative exposure-response trends for bladder cancer and asthma with medication.
Background
Perfluorooctanoic acid (PFOA) is a man-made 8-carbon perfluorinated compound (PFC) which has been used in manufacturing fluoropolymers, such as polytetrafluoroethylene (Teflon), and other non-stick products (Scotch Guard, Gore Tex).1 PFOA is persistent in the environment and is not metabolised in the body; it has a half life in humans of approximately 2.3–3.4 years.2–4
Human exposure to PFOA can occur through occupational exposure5 or through food (contamination during preparation and from packaging), drinking water,6 house dust7 and air.8 PFOA was found in the serum of more than 99% of the general USA population in the 2005–2006 National Health and Nutrition Examination Survey (NHANES), with a median concentration of 4 ng/mL.9 Production of PFOA has recently been stopped in the USA due to suspected toxicity but according to the Environmental Protection Agency (EPA), PFOA continues to be used in manufacturing (epa.gov/oppt/pfoa/index.html, last accessed 19 November 2014). However, PFOA persists in the serum of the US population, with no decreases having been observed in the period 2003–2008.9
In animals, such as mice, rats, and non-human primates, observed effects of PFOA relating to chronic diseases have included tumours of the testicles, liver and pancreas; decreases in some immune responses; atrophy of spleen and thymus; hepatomegaly and impaired thyroid hormone homeostasis.1 ,10 ,11
In humans, the primary associations that have been observed have included ulcerative colitis (an autoimmune disease),12 thyroid disease,13 high cholesterol,14 ,15 kidney cancer,16 ,17 testicular cancer,17 ,18 prostate cancer19 ,20 and non-malignant kidney disease.16 Pregnancy-induced hypertension has also been associated with PFOA.21
Although PFOA is present at low levels in the serum of virtually everyone in the USA, there are a few US communities with high exposure to it. One of these communities is located in the mid-Ohio valley near a DuPont plant in West Virginia, which emitted PFOA into the air and water from 1951 to 2001 after using it to make Teflon and other polyfluorinated products.22 In 2004, a lawsuit brought by the community against DuPont was settled. As part of the settlement, a baseline survey was conducted (called the C8 Health Project) in 2005/2006, in which serum PFOA was measured in 69 000 past and present residents of the six contaminated water districts (including some workers from the DuPont plant).22 In addition, a scientific panel was set up (the C8 Science Panel) to study possible associations between PFOA and health. The C8 Science Panel (c8sciencepanel.org, last accessed 19 November 2014) conducted a number of studies of the community surrounding the plant and of workers in the plant. The current study is an extension of the work conducted by the C8 Science Panel.
The 3713 workers considered here are a subset of two prior studies conducted by the C8 Science Panel, an occupational mortality study16 and a combined community/worker study of disease incidence.22
The mortality study included all workers with at least 1 day of work at the DuPont plant between 1948 and 2002 (n=5791).16 We estimated PFOA serum levels over time for these workers by considering occupational5 and residential exposures (the latter from contaminated drinking water).6 In the mortality study, we found positive dose–response trends for kidney cancer and kidney disease, based on small numbers of deaths.16
We have also previously conducted a cohort study of disease incidence among community residents living near or working in the DuPont plant (n=32 254).22 This study combined incidence data from a community cohort (n=28 541) with incidence data from a subset of workers from the cohort mortality study, ie, those whom we were able to interview, and who had good work and residential history data (n=3713). Studies of disease incidence have advantages over mortality studies: (1) these can be used for analysis of non-fatal diseases, (2) incident cases are usually more numerous than deaths from specific causes, and (3) these are more directly relevant to causal inference given that they are free from the effects of treatment after disease occurrence.
In the combined community/worker cohort incidence study, we found positive trends between PFOA and kidney cancer, testicular cancer, thyroid disease, ulcerative colitis and high cholesterol.12 ,13 ,15 ,17 However, no comprehensive results for incidence only among the workers have been previously published; this is the subject of the current report. There has been no prior cohort study of disease incidence among PFOA-exposed workers, with the exception of one report of cancer incidence in an occupational cohort.23
High-exposure groups are often the most useful for studying human health effects. Workers often have higher PFOA exposures than the general population. A subset of the 3713 workers considered here (n=1881), who had their serum PFOA measured in 2005/2006, had a median serum level of 113 ng/mL, much higher than the surrounding community (median 24 ng/mL), and the general US population (4 ng/mL).22
Methods
More detailed methods used for the combined community/worker cohort have been described previously by Winquist et al.22 Below we summarise these methods briefly, focusing particularly on health aspects relating to the workers.
Population and data collection
The original worker cohort assembled by DuPont at their West Virginia plant included 6026 workers with at least 1 day of work between 1948 and 2002.24 Of these, 5791 had been included in our prior worker cohort mortality study, which had followed workers for mortality throughout 2008.16 Death certificates obtained from the worker morality study were used to identify the next of kin for deceased workers.
We were able to interview 4391 (73%) of these 6026 workers or their next of kin, after obtaining informed consent either verbally or on the Web. The primary reason for not interviewing workers was the inability to find them or proxies for them, especially for older and deceased workers. We were able to obtain an interview for 79% (3822 of 4837) of workers who had not died, but for only 48% (569 of 1189) who had died of the 6026 target population. Of the 4391 workers for whom interviews were obtained, 3713 (85%) had retrospective exposure estimates and were included in this analysis; the remaining 678 were excluded due to lack of occupational exposure estimates or insufficient residential history information prohibiting estimation of their residential exposure. Of the 3713 workers in the analysis, 6% had interviews completed by their next of kin (due to being deceased or too sick to complete the interview).
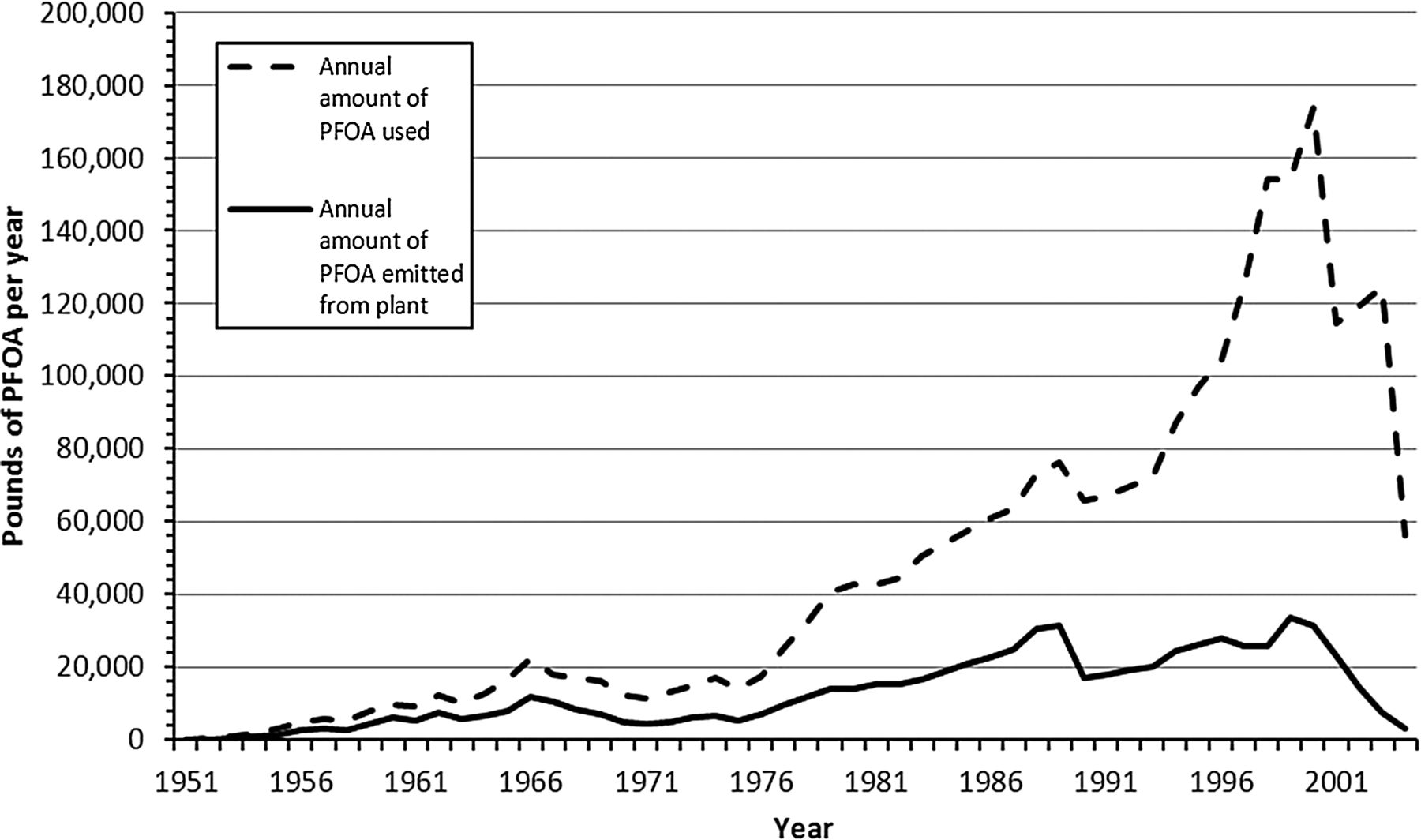
Interviews were conducted in two rounds, from 2008 to 2011. We sought to interview all workers twice, with the second interview seeking data about any new disease incidence since the first interview. Among the 3713 included in the analysis, some workers were interviewed only once (of those in the final cohort, 166 had round 1 interviews only, 549 had round 2 only and 2998 had interviews at the two time points). Person-time at risk ended at the latest available interview. Interviews collected information about demographics, smoking, residential history (all residences since birth), medical history and reproductive history. Residential history was truncated artificially at 1970 for 23% of the cohort analysed here due to conflicting questions in the interviews; this resulted in an underestimation of exposure for these participants, but as the emissions from DuPont were very low before 1970 (see figure 1), the residential exposure before 1970 was minimal and hence, the errors in cumulative exposure would have been minimal.

{kind=link}
Perfluorooctanoic acid (PFOA) usage and air/water emissions over time at the DuPont plant.5
We collected data for a number of chronic disease outcomes and sought their medical record validation (coronary heart disease, stroke, chronic obstructive pulmonary disease, autoimmune disease, type 2 diabetes, liver disease (hepatitis and non-hepatitis), Parkinson's disease, Alzheimer's disease, thyroid disease, asthma with reported current medication and cancer). Participants reporting disease were asked the year of disease diagnosis. Permission to seek medical records was asked of all interviewees reporting a disease.
We also collected data on three self-reported outcomes for which workers had sought medical attention, but for which we did not seek medical record validation. These were osteoarthritis, hypertension and high cholesterol. Analyses of these outcomes were restricted to participants who reported they were currently taking prescription medication for the condition (34%, 87% and 66%, respectively). We did not seek medical record validation for these outcomes based on the significant extra cost of collecting medical records for these common outcomes and our belief that these are less likely to be falsely reported as present when not severe enough to be treated.
Estimates of yearly PFOA serum levels
We used estimated retrospective yearly PFOA serum levels as our exposure measure. These had both an occupational and a residential component.
Occupational exposure
PFOA was used at the plant from 1950 to 2004, with the peak usage occurring in the 1990s and sharply decreased usage and emissions after 2001, as seen in figure 1.
To estimate the yearly PFOA serum level of each worker in the prior mortality study of the worker cohort, a job-exposure matrix (JEM) was created.5 We used this JEM in our current analysis of the worker incidence cohort. There were five job category/job group combinations in the matrix, three of which had subgroups: (1) direct PFOA exposure in the Teflon production area (fine powder/granular polytetrafluoroethylene in the chemical department, with a dichotomous variable for working in the chemical operator job group); (2) direct PFOA exposure among workers in the other copolymer production areas that used PFOA, including fluorinated ethylene propylene and perfluoroalkoxy fluoropolymer operations; (3) intermittent direct PFOA exposure or plant background PFOA exposure jobs such as the tetrafluoroethylene monomer production operations, and Teflon and copolymer jobs, including laboratory workers, engineers, upper-level supervisors and clerks, with a dichotomous variable for working in a tetrafluoroethylene monomer job group; (4) maintenance jobs with intermittent direct or plant background PFOA exposures, with a dichotomous variable for having been assigned to the Teflon/copolymer maintenance job group and (5) non-Teflon/copolymer production division jobs with no PFOA use (plant background PFOA exposures).
The JEM was based on over 2000 serum samples collected from workers during the period 1979–2004 from workers with at least 1 year work experience in the job category at the time of sampling (these workers may or may not be in our worker cohort). These serum samples were matched to the job category/job groups listed above to estimate yearly serum levels in each category/group by using a general linear model taking correlation of repeated measures into account. This model regressed observed log serum PFOA level on job category/group, previous years in that category/group for a worker and the amount of PFOA used at the plant in any given year, and used a spline function for calendar time.
It should be noted that our occupational serum estimates crudely incorporate any residential exposure, as these are based on observed serum levels in workers, which reflects their residential as well as occupational exposure. Residential exposure could at times be high for workers living in residential areas with drinking water highly contaminated with PFOA.25 For workers, who had estimated and measured serum levels in 2005/2006 (n=1881), measured and estimated serum levels correlated well (Spearman correlation 0.67).
Residential exposure
Retrospective serum estimates for community residents, due to exposure to PFOA-contaminated drinking water, were obtained from a multistage modelling procedure described in detail elsewhere.6 Briefly, an environmental fate and transport model was used to generate yearly estimates, from 1951, of PFOA concentrations in the local air, surface water and groundwater. These estimates were based on historic emission estimates from the plant, the physicochemical properties of PFOA, and local geological and meteorological data. To estimate each person's yearly PFOA intake rate in a community-exposure model, the estimates of air and water PFOA concentrations from the fate and transport model were used in combination with residential history information from the 2005/2006 C8 Health Project and our 2008–2011 surveys along, information about drinking water sources and water consumption rates, and public water supply network maps. Finally, a pharmacokinetic model was used to generate yearly serum PFOA concentration estimates based on each person's yearly intake rate estimates, demographic information, self-reported body weight, estimated background exposures and PFOA half life estimates.6
Combining occupational and residential serum estimates
Yearly serum estimates from the occupational exposure model were used for the years when people worked at the plant if these were higher than residential estimates; if they were lower, the residential (community) estimates were used. For approximately 82% of workers, yearly occupational exposure estimates were always higher than corresponding residential estimates. For the years after working at the plant, serum estimates were decayed at a rate of 18% per year, based on a presumed half life of 3.5 years,4 until they reached a level predicted by the model for community residential exposure. Model-based exposure estimates were available through 2008. Serum concentration estimates for 2009 until the time of the last interview were generated assuming a constant decay rate of 18% per year.
Analyses
Analyses were restricted to validated cases; self-reported non-validated cases were excluded from the analysis. We used Cox regression models with age as the time scale, and time-varying exposure and covariates to analyse data for the worker cohort. The risk period started at age 20 years or from 1951, whichever was later, and continued until disease occurrence or the end of study at the last interview. Risk sets were formed for each case of disease based on selecting those who had not had the disease at the age of the case at time of the case's diagnosis; time-dependent cumulative exposure was calculated for all members of the risk set only up until the age of diagnosis of the case. Our principal exposure metric was cumulative exposure, with or without a 10-year lag period. Cumulative exposure was calculated as the sum of yearly exposure estimates from birth through any given year. Models were controlled for gender, race (Caucasian/non-Caucasian), education (less than high school, high school, some college and college) and body mass index (<18.5, 18.5–24.9, 25–29.9, ≥30.0 kg/m2), and time-varying smoking (current, former, never) and alcohol consumption (current, former, never). These variables were chosen as potential confounders on the basis of being associated with both exposure and a number of disease outcomes, and have been previously used in our analysis of the combined community/worker cohort. Models were stratified by year of birth for a 5-year period to control for potential confounding (exposure changed markedly over calendar time and incidence for some diseases has also changed over calendar time). Analyses were restricted to outcomes with 20 or more cases. The proportional hazards assumption was tested via an interaction term between time (the age variable) and log cumulative exposure, which was not significant in any of the disease-specific analyses.
Cumulative exposure was analysed as a continuous (linear or log transformed) or categorical variable. Analyses using continuous variables were essentially parametric tests for trend. We conducted categorical analyses by using quartiles, with common cut points across all diseases, with cutpoints for quartiles the same across all diseases. The cutpoints were chosen based on the quartiles of cumulative exposure for all cases combined. Trend tests for categorical analyses used a weighted linear regression of log rate ratios (RRs) on the midpoints of the quartile categories, with the line constrained to pass through the origin and weights equal to the inverse of the variance of the log RRs. The categorical trend tests avoided strong parametric assumptions about the shape of the exposure-response curve using individual data and instead looked for a linear trend in response across categories of cumulative exposure.
Results
We first compared the 3713 workers included in the incidence analysis and the 2313 not included (1635 not able to be interviewed, 678 with incomplete residential or work history). The included workers were less likely to be known to have died by the end of the study (6% vs 43%), were more likely to be female (20% vs 17%), and were younger (median year of birth 1951 vs 1943). Comparing the 3713 included workers to those excluded workers who had complete work history (n=2068), the included workers had started work later (1979 vs 1970), and had higher cumulative occupational exposure (mean 8.6 vs 6.5 ppm/years); both groups had worked a similar amount of time (mean 20 vs 19 years). These differences are largely due to the fact that workers who were older started to work earlier and were more likely to have died, and were also those more difficult to trace. Younger workers were more likely to be female and also to have had higher exposures, as use of PFOA in the plant peaked relatively recently, in the late 1990s (figure 1).
Descriptive statistics for the cohort included in the analysis are found in table 1. The median year of birth was 1951; 6% of the cohort were known to have died by the end of the study. Most cohort members were male, Caucasian, never-smokers, ever-alcohol drinkers and had obtained more than a high school education. The median measured serum level (for those who were measured in the C8 Health Project 2005/2006, n=1881) was 113 ng/mL in 2005 compared with 4 ng/mL in the US population, while the median predicted level from the exposure prediction model for these 1881 workers (based on residential and occupational exposures) in 2005/2006 was 94 ng/mL. The mean measured and predicted levels (325 ng/mL and 218 ng/mL, respectively) corresponded less well than the median, as the distribution of serum levels had a large variance and means were highly affected by extreme values.
Descriptive statistics for a cohort of workers employed between 1948 and 2002 at a DuPont plant in West Virginia (n=3713)
Table 2 provides data on the number of self-reported cases of disease, the number for whom we obtained medical records and the per cent validated from medical records. Overall, 2845 cases of chronic disease were self-reported in this worker cohort; we obtained medical records for 83%. Of those for whom we obtained medical records, 81% of were validated.
Number of reported and validated cases of chronic diseases in workers
Disease-specific survival analysis results, with no lag or a 10-year lag, are shown in table 3 and restricted, as noted previously, to those outcomes with 20 or more cases. We found a positive trend using the log of cumulative exposure for ulcerative colitis (n=28) which was significant at the 0.05 level for no lag and a 10-year lag. The trend test across quartiles was also statistically significant for the analysis of cumulative exposure with a 10-year lag. The highest exposure category for ulcerative colitis (with a 10-year lag) had a RR relative to the first quartile of 6.57 (95% CI 1.47 to 29.40).
Disease-specific RRs for PFOA from Cox regression for outcomes with 20 or more cases
No other disease showed a statistically significant positive trend using the log transform trend test. However, rheumatoid arthritis (like ulcerative colitis, this is an autoimmune disease) showed a significant positive trend (p=0.04, no lag, n=23) using the trend test based on the quartile midpoints. The highest exposure category for rheumatoid arthritis (no lag) had a RR relative to the first quartile of 4.45 (95% CI 0.99 to 19.9), borderline significant at the 0.05 level. A limitation of the findings for both of these autoimmune diseases among workers is the small number of cases.
We also found a significant positive trend for type 2 diabetes (lagged 10 years) using the categorical trend test. However, the observed increase in RRs was quite modest, none of the quartile RRs were appreciably elevated and the statistical significance of the trend may have stemmed largely from the large number of cases (n=408).
Prostate cancer with a 10-year lag showed a positive trend across quartiles (p value categorical trend 0.10; n=129). Similarly non-hepatitis liver disease (35 cases, 10-year lag) also showed a positive trend in categorical analyses (p=0.08 in categorical trend test), as did male thyroid disease (10-year lag, 82 cases; p=0.06 in categorical trend test). However, none of the highest quartiles RRs were significantly elevated relative to the first quartile at the 0.05 level.
It should be noted that some trends were negative. In particular, bladder cancer showed a negative trend using log cumulative dose (for the analysis with no lag) and the categorical trend test (for the analysis with a 10-year lag), albeit based on a limited number of cases (n=23). We also found a negative trend for asthma with medication (no lag) in the categorical trend test.
Discussion
We have found significant (at the 0.05 level) positive trends between PFOA and both ulcerative colitis and rheumatoid arthritis, and suggestive positive trends for prostate cancer, non-hepatitis liver disease and male thyroid disease. A significant negative trend was found for bladder cancer and asthma with medication.
Our positive findings for ulcerative colitis among the workers is in agreement with our prior findings for this disease in the combined community/worker cohort, where this disease was the most strongly associated with PFOA from among all diseases studied.12 Here too, among the workers, both trend tests (continuous log transformed cumulative exposure or using the midpoints of the quartiles) were significant at the 0.05 level. A second autoimmune disease, rheumatoid arthritis, also showed a strong positive trend in quartile analyses, but only the trend test using the midpoint of the quartiles was statistically significant. We did not find a trend in rheumatoid arthritis in our combined community/worker cohort,12 although the cumulative exposures were generally much lower in the community than among the workers; the cut points for the quartile analysis (no lag) in the community/worker combined cohort were 0.12, 0.23 and 1.43 µg/ml-years, compared with the cut points of 3.03, 6.16 and 11.42 µg/ml-years used here for the workers.
These findings raise the possibility that, in high doses, PFOA could be associated with more than one autoimmune disease, but the limited number of cases suggests caution in making any inferences. No general autoimmune mechanism has been proposed for PFOA, although there are several candidates for a mechanism for ulcerative colitis. Suggested mechanisms linking PFOA and ulcerative colitis include shifts in the balance of tissue macrophages towards an anti-inflammatory phenotype and/or a T helper cell-like response to specific antigens.26
There are also suggestive findings for prostate cancer (n=129), non-hepatitis liver disease (n=35), male thyroid disease (n=82, highest category RR=2.16 (0.98 to 4.77), no lag), and to a lesser extent, type 2 diabetes (n=408). However again these trends were found only in the quartile analyses and not while using the continuous log-transformed cumulative dose as the basis for a trend test. Our findings for prostate cancer, non-hepatitis liver disease and male thyroid disease have some support in earlier work. Positive prostate cancer trends, generally of borderline significance, were found in Vieira et al18 (ecological study in the mid-Ohio valley), Eriksen et al19 (study in population with background PFOA levels), and Lundin et al20 (study in population with occupational levels). Positive trends in male thyroid disease were found in our community/worker combined cohort study.13 However, that study also found positive trends among women, whereas our current findings were largely limited to men. Findings for non-hepatitis liver disease in other occupational cohorts have shown mixed results11 and our own combined community/worker cohort did not find positive trends (http:www.c8sciencepanel.org/prob_link.html, last accessed 21 November 2014). However, Gallo et al27 did find a positive association between PFOA measured in 2005/2006 in the mid-Ohio Valley and increased alanine transaminase liver enzyme levels, in a cross-sectional analysis. The liver is also a site of interest because liver tumours are caused by PFOA in rodents and liver enlargement is also seen in rodents.10
Regarding type 2 diabetes, we found a very modest positive trend using the categorical trend test, for which statistical significance may have been driven by large numbers (n=408); none of the quartile RRs were appreciably elevated. There have been two earlier occupational mortality studies with positive findings based on small numbers. Lundin et al20 studied mortality among 3993 workers at a 3M plant in Minnesota and found a twofold excess of diabetes among the ‘probably exposed’ (42% of the workers) compared with the Minnesota population (RR=2.0, 95% CI 1.2 to 3.2, 18 diabetes deaths). Probably and definitely exposed workers compared with never-exposed workers had a relative risk of diabetes death of 3.7 (1.4 to 10.1, 18 vs 5 deaths). Steenland and Woskie16 also found a twofold excess of diabetes mortality comparing the same exposed DuPont workers studied here with other non-exposed DuPont workers from different plants (n=38, standardised mortality ratios (SMR) of 1.90, 1.35 to 2.61), with little trend across quartiles of cumulative serum levels (SMRs=1.9, 1.5, 2.3 and 1.9). In contrast with these mortality findings, studies of the community surrounding the DuPont plant found no increases in diabetes morbidity or glucose, with much greater numbers of diabetes cases.28 ,29
We found no indication of positive trends between PFOA and high cholesterol (self-reported medicated hypercholesterolaemia), which is in contrast to our finding in the combined community/cohort study.15 Our findings in the combined community/worker study were largely confined to men, especially men aged 40–60. When we analysed the male workers aged 40–60 for cholesterol in the current study, we found RRs by quartile (no lag) of 1.00, 1.25, 1.12 and 1.18. However, in the combined community/worker study, the rate increase was seen primarily between the first and second quintiles, with little increase across subsequent quintiles, and the category cut points in that study were much lower (the start of the second quartile in the current study was in the range of the fourth quintile in the combined study).
We found a significant (at the 0.05 level) negative trend for bladder cancer with a 10-year lag, based on a relatively small number of cases (n=29). This is noteworthy because of finding a positive trend by exposure category for bladder cancer incidence (n=93) at another plant using PFOA (3M) in Minnesota (RR=1.66 (0.86 to 3.18) in the highest category, no test for trend given).24 We also found a significant negative trend (p=0.05) for asthma (no lag) with medication. To the best of our knowledge there are no other data for incident asthma in the literature.
In general, the workers in the current study had much higher exposures than the community cohort, and consequently our quartile analyses are based on quartile cut points which are much higher than those used in the community analysis. It is possible that restriction to workers might miss trends at lower exposures which flatten out at higher exposures30 or reveal trends that are apparent only at very high exposures. Further follow-up of this cohort will yield larger numbers of cases and allow for more inferences.
Strengths of our study include obtaining data on disease incidence for the majority of our target population, verification of self-reported disease via medical records, use of estimated serum PFOA as our exposure measure, retrospective occupational exposure assessment based on over 2000 serum samples and detailed work history, residential retrospective exposure assessment based on detailed plant emissions data and residential history, and exposure estimates which correlated well with measured serum levels. Weaknesses include limited sample size for some outcomes; for example, we had too few cases of kidney cancer and testicular cancer, two end points which had positive findings in the combined community/worker cohort, for meaningful analysis when restricting to workers only. Other limitations of our study were our ability to interview and analyse data for only 62% of the target population (raising the possibility of selection bias if exposure-response data differed in the excluded vs the included), potential error in estimated past exposure via a model, our relative inability to locate the next of kin of hard-to-trace decedents (so that they were under-represented, limiting power for some fatal diseases), and failure to obtain medical records for 17% of those self-reporting disease.
References
Footnotes
-
Funding This research was funded by the C8 Class Action Settlement Agreement (Circuit Court of Wood County, West Virginia, USA) between DuPont and Plaintiffs, which resulted from releases into drinking water of the chemical perfluorooctanoic acid (PFOA or C8). Funds were administered by an agency that reports to the court.
-
Competing interests None.
-
Ethics approval Emory University Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.