Article Text

Abstract
Background: The lack of efficient medical interventions for combating increasing sickness absence rates has lead to the introduction of alternative measures initiated by the Norwegian National Insurance Service or at workplaces.
Aim: To determine whether minimal postal intervention had any effect on the length of sick leave.
Methods: Randomised, controlled trial with a one year follow up in Northern Norway in 1997 and 1998; 990 consecutive newly sick-listed persons with musculoskeletal or mental disorders were studied. Within the intervention group, 495 eligible sick-listed persons received a general information letter and a questionnaire as their sick leave passed 14 days. Possible intervention effects were analysed by survival analysis of the probability of returning to work within one year, and logistic regressions with benefits at one year as the dependent variable.
Results: The overall reduction of 8.3 (95% CI −22.5 to 6.0) calendar days in mean length of sick leaves in the intervention group compared to controls, was not statistically significant. However, intervention significantly reduced length of sick leaves in subgroups with mental disorders, and with rheumatic disorders and arthritis, and overall for sick leaves lasting 12 weeks or more. Young people with low back pain showed an adverse effect to intervention. The overall relative risk of receiving benefits due to sickness after one year in the intervention group was 0.69 (95% CI 0.51 to 0.93) compared to controls.
Conclusion: The results should encourage employers, insurance institutions, and authorities to initiate challenges as questions on the length of sick leave and possible modified work measures, during the first few weeks of sick leave, for at least some groups of sick-listed persons.
- NIO, National Insurance Office
- RDA, rheumatic disorders and arthritis
- RTW, return to work
- musculoskeletal
- randomised controlled trial
- sickness absence
- sick leave
- sick-listed persons
Statistics from Altmetric.com
The increasing rate of sick leave experienced in most Western European countries challenges insurance companies, employers, and public authorities to identify measures to reduce the associated burdens on individuals, workplaces, and finances. In Norway, employees can report themselves sick for three days, four times a year. If sick beyond three days, the sick leave must be confirmed by a medical doctor through a standardised medical certificate. Sick leave beyond eight weeks needs an extended medical certificate, and a formal decision within the National Insurance Office (NIO) is required for sickness benefits beyond 12 weeks. If the employee is not able to return to work after a year, they can receive rehabilitation benefits, on certain medical terms, for another year. Musculoskeletal disorders contributed to 48.8% of sick leave periods exceeding 16 days in 2001 in Norway, while mental disorders came second at 18.8%, increasing their proportion from 14.4% in 1999.1
Reviews on the treatment and rehabilitation of low back pain, and rehabilitation of other musculoskeletal disorders have provided, at best, only ambiguous recommendations for medical strategies to reduce the length of sick leave.2–4 The National Insurance Services have focused on efficient medical interventions for combating the increasing rate of sickness absence. However, intensified inquiries of medical certificates within the NIOs did not reveal the expected effect.5 In 2000, the “Sandman Report” (sickness absence and disability pensioning) provided a policy guideline of a reinforced dialogue between employees and employers to reduce the level of sick leave.6 Several studies supporting this policy have revealed considerable potential for reducing sick-leave periods by adjustment of work demands,7–9 and indicated the necessity of work adjustments in successful rehabilitation.10 However, the initiation of work adjustments by the NIO is time consuming, and hence the search for more cost effective interventions is continuing.
The aim of this study was to determine whether there is any effect on the length of sick leave by minimal postal intervention, including information on available work measures for sick-listed persons, and questions on the expected length of the current sick leave and on any relevant work adjustments for the ongoing sick leave.
METHODS
Inclusions
Some 1000 persons certified as sick for longer than 14 days with musculoskeletal or mental disorders (ICPC, L and P diagnoses),11 were included consecutively in this randomised prospective study in the cities of Tromsø and Harstad in Northern Norway. The enrolments were performed during two periods: October and November 1997, and March and April 1998. The sick-listed subjects were assigned consecutive numbers from 1 to 1000 according to the order of their enrolment; at the end of each day they were randomly distributed by their number into the intervention group (499 persons) or the control group (501 persons) according to a pre-drawn list.
The sickness certificates for each person included information on gender, age, diagnoses, occupations, and the current certified period of sick leave. The total length of sickness absence, the first year after start of the inclusion sick leave, was collected from the National Sickness Benefit Register for 996 of the included persons. Two persons with full-time disability pension and one person with initially misclassified diagnosis were excluded. Three intervention envelopes were returned by the postal service without reaching the addressee; these two men and one woman were included in intention-to-treat analysis but excluded from the general analysis. A conservative assessment supported their exclusion as their shorter-than-average sick leaves would have marginally favoured an effect of intervention.
According to intention-to-treat principles all subjects that received the intervention package were kept in the intervention group regardless of response. Of the 495 persons in the intervention group, 160 (32.3%) answered the questionnaire. A total of 159 persons answered the questions on possible reduction of this sickness absence; 159 had marked their wishes on the copy to their NIOs or not: 61 persons had marked yes.
The intervention group finally comprised 192 men and 303 women, and the control group comprised 197 men and 298 women (table 1). The mean age was 40.9 (median 41, range 17–66) years in cases and 39.9 (median 39, range 18–66) years in controls.
Baseline characteristics in the intervention (I) and control (C) groups, and mean length of sick leave
Intervention
Via a minimal intervention package posted 14 days after the start of the current sick leave, the intervention group received brief general information on possible work related measures if sick-listed, and a questionnaire related to the actual sick leave. The intervention package is summarised in box 1. Together with the information letter and the questionnaire was a letter on consent to answer the questionnaire and on the possibility to arrange for contact with the NIO office. Some 291 persons returned the request; of these, 161 had filled in the questionnaire. The local NIOs undertook normal follow up activities during this period, and were unaware of the group status for the included subjects except for 61 sick-listed subjects who provided their NIO officers with a copy.
Analysis and data management
Comparisons between categorical variables were analysed by χ2 tests. In cross-sectional analysis after one year, χ2 tests and binary logistic regression with backward conditional removal at p = 0.10 were used to explore candidates for the final model, analysed using the enter method. Differences in the length of sick leaves—as a continuous but not normally distributed variable—were analysed by the Mann–Whitney two-sample test and Kaplan–Meier analyses. The 95% confidence interval (CI) of differences in length was calculated assuming a normal distribution. Cox proportional hazards models were used to calculate the hazard ratio with 95% CI, of returning to work. A hazard ratio greater than one indicates increased chance of return to work (RTW) according to the actual coding. All tests were two sided and required p < 0.05 to be considered significant. The analyses were performed with SPSS software (version 11.0).
Continuous calendar days (or weeks) with benefits due to sickness were used in the analysis of length. If benefits changed from sickness benefits to maternity benefits or old age pensions, the sick-leave period was ended and censored in survival analyses. The maximum length was set to 365 days and right censored in survival analysis. The time of formal decision regarding further sickness benefits after 12 weeks was used as a cut-off for evaluating possible short or long term effects. Persons receiving maternity benefits or old age pensions were excluded from cross-sectional analyses.
Musculoskeletal diagnoses in sickness certificates were recoded into low back pain (L02, L03, L84, L86), neck disorders (L01, L83), shoulder and arm disorders (L08–12, L92, L93), injuries (L72–81), unspecified (L99), and rheumatic disorders and arthritis (RDA disorders) (L04, L13–20, L29, L70, L82, L87–91, L94–98). The last group included 20 persons with rheumatic diseases, 12 with osteoarthritis (hip, knee, and unspecified), 19 with other knee disorders, 20 with symptomatic joint disorders (pain), and 28 with more generalised muscular pain, including seven persons with fibromyalgia. Mental disorders were recoded into depression (P03, P76) and other mental disorders. In multivariate analysis, each group was coded (“no” or “yes”) and the RDA disorders were used as the reference, if not specified otherwise.
In diagnosis stratified analysis, the neck, shoulder and arm, injuries, and unspecified musculoskeletal disorders groups were successively recoded into the “other musculoskeletal” group, according to intervention survival curves indicating no obvious intervention effects.
Occupation given on sickness certificates was classified into health and teaching work, administrative, clerical and sales work, agriculture and fisheries work, transport and communication work, manufacturing work, service work, and unknown occupation. In multivariate models the subgroups were coded (“no” or “yes”) with unknown together with agriculture and fisheries as the reference occupation.
Education level was estimated according to professional titles in sickness certificates and grouped into not more than 12 years of formal education, and more than 12 years of education including indeterminable education level.
Ages were recoded into 10 year groups, with the first expanded to 17–29 years.
Approval
The Regional Ethical Committee approved the protocol; the Norwegian Data Inspectorate licensed the necessary register of sick-listed subjects, and approved the linkage to follow up data on sick leaves.
RESULTS
The ongoing sick leaves represented a total of 48 007 days of continuous absence due to sickness in the intervention group, compared to 52 104 days in the control group. The reduction of 4097 days in the intervention group corresponded to a mean reduction of 8.3 days for each sick-listed person. The mean length of sick leave was 97.0 and 105.3 days, respectively (table 1), while the median length was 48 days in both groups.
In the intention-to-treat analyses, length of sick-leave in the intervention group was reduced by a mean of 8.6 days (95% CI −5.6 to 22.8) compared to the control group.
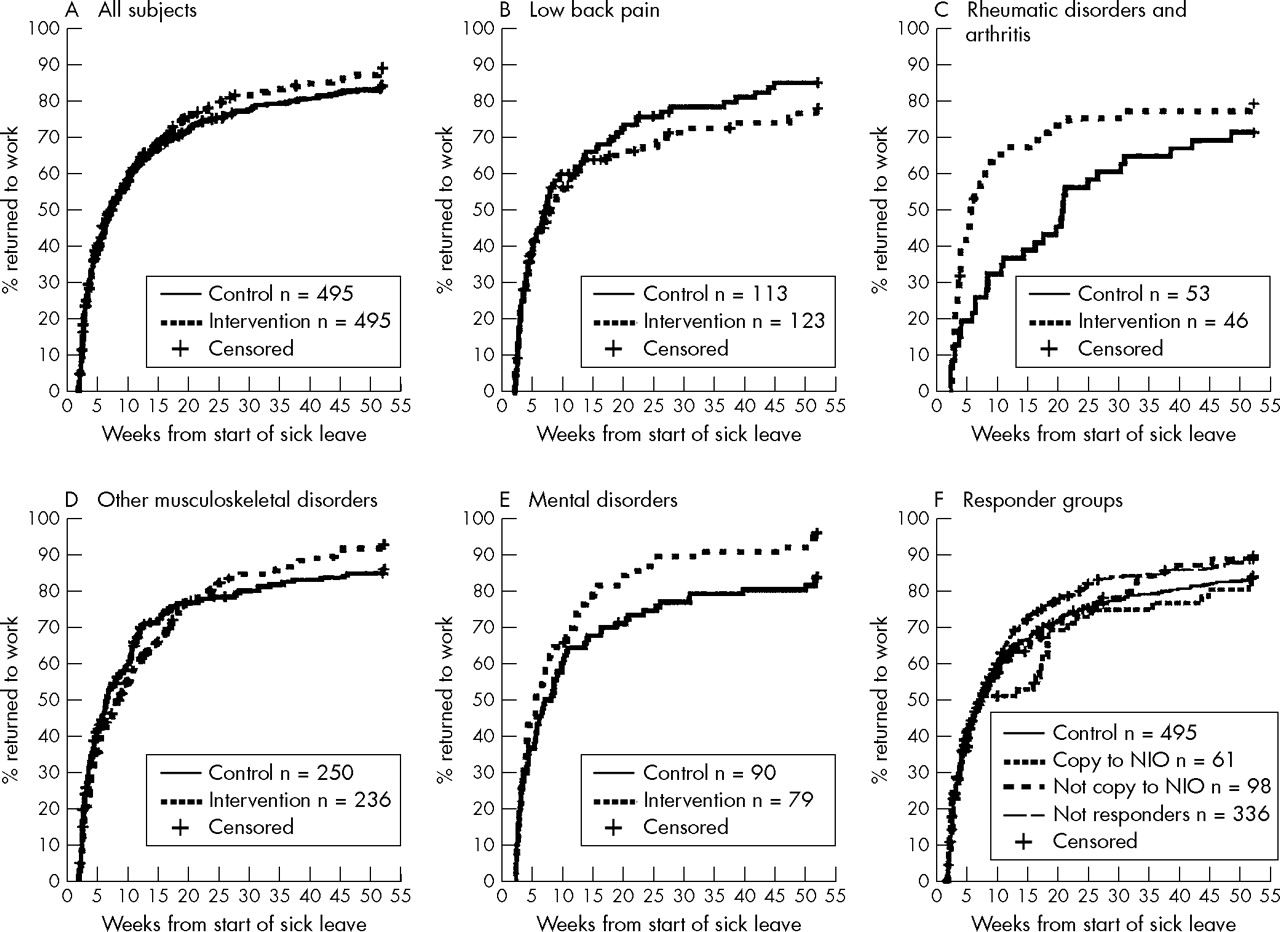
Stratified analyses on the diagnostic groups showed shorter sick leaves in the intervention group except for low back pain and neck disorders (table 1 and fig 1). The intervention effect was most apparent for sick-listed persons with RDA or mental disorders. The RTW rates were practically identical in intervention and control groups during the first 12 weeks of sick leave, except for the RDA group (fig 1C). The minimal intervention resulted in an overall significant reduction in the length of sick leaves lasting 12 weeks or longer, although an inverse effect was observed for persons sick-listed for low back pain. In the low back pain group sick-listed beyond 12 weeks, interaction analyses in the Cox model showed significant interaction terms, age group × intervention (p = 0.02). In stratified Cox proportional hazards models (table 2), the inverse intervention effect for low back pain was restricted to 33 sick-listed persons younger than 41 years and with not more than 12 years’ education. They had a hazard ratio of 0.39 (95% CI 0.21 to 0.74) for RTW compared to the 37 persons in the control group. In the RDA group, the reduction effect of minimal intervention was restricted to the group of sick-listed subjects with less education (hazard ratio = 2.51, 95% CI 1.26 to 5.00). Gender and occupation did not significantly influence the intervention effect.
Hazard ratios of return to work after minimal postal intervention compared to control group, analysed in separate Cox proportional hazards models with length of sick leave as the dependent variable

{kind=link}
Percentages of sick-listed subjects who had returned to work as a function of weeks from the start of sick leave for (A) all subjects; subjects stratified into four major diagnostic groups: (B) low back pain, (C) rheumatic disorders and arthritis, (D) other musculoskeletal disorders, (E) mental disorders; and (F) the intervention group stratified into response alternatives.
The return to work (RTW) curves indicated delayed (reduced) RTW from 6 to 16 weeks in the responder group (n = 160) with observed RTW of 33 (95% CI 23.4 to 44.3) subjects compared to the expected 43.6. Observed RTW in the subgroup requesting copy to NIO was 7 (95% CI 2.9 to 13.5), expected 16.6 (fig 1F). Observed RTW among the 52 subjects positively expecting reduction of the actual sick leave if modified work measures were implemented was 4 (95% CI 1.1 to 9.6), expected 9.9.
Results after one year follow up
One year after the start of the actual sick leave 121 persons were receiving sickness benefits, 32 vocational rehabilitation benefits, 59 medical rehabilitation benefits, and 50 disability pension. Another 80 persons received maternity benefits, 7 received old age pension, and 2 were registered dead, leaving 639 persons without any benefits from the National Insurance Service.
The risk of receiving benefits due to sickness after one year was reduced in the intervention group (table 3). The interaction terms, education × intervention, was significant (p = 0.04) in the regression model for any benefits in total material.
Odds ratios (OR), calculated in binary conditional logistic regression models, for receiving social service benefits due to sickness one year after the start of sick leave, if a sick-listed subject was exposed to minimal intervention at 14 days of sick leave
DISCUSSION
According to the intention-to-treat analysis of the main outcome, no overall statistically significant effect of minimal postal intervention on the length of sick leave was found. However, this randomised, controlled study revealed that minimal postal intervention could reduce the length of sick leave among persons with mental or RDA disorders, the length of sick leave lasting at least 12 weeks, and the chance of receiving benefits due to health related problems after one year. Simultaneously, the results disclosed a potential inverse effect in young persons with little formal education and low back pain, and a potential delay in the RTW in the period from 6 to 16 weeks for sick-listed persons presuming an effect of modified work, or those providing their NIO with a copy of their response.
Material
To reduce the risk of selection bias, the sick-listed persons were assigned consecutive numbers at enrolment and then randomised into the intervention or control group according to the pre-drawn randomisation list. Ten sick-listed subjects were later excluded: three did not meet the inclusion criteria, the National Sickness Benefits Register information was not available in four cases, and three cases in the intervention group never received their intervention envelope. The distributions of diagnosis, occupation, age, gender, and education were comparable between the two groups, indicating no selection bias.
The intervention
The intervention group received an envelope with information and a questionnaire. One third of the subjects in this group answered the questionnaire, indicating that they had read and most likely reflected on the questions. The use of a National Insurance Office envelope is likely to reduce the probability of the post being disposed of without opening, as subjects might assume that the payment of benefits depends on their responding to letters from the National Insurance Office. The information letter started with a heading “Follow up of sick-listed”, and stated that the participation was voluntary. Although answering the questionnaire was voluntary, we believe that most sick-listed people in the intervention group read at least part of the information and questionnaire to decide whether or not they should respond. By reading at least some of the questions they were exposed to the intervention strategy, regardless of returning the questionnaire or not.
Awareness of being studied
In this open study, both intervention and control groups were exposed to the usual activities from their general practitioners and their National Insurance Offices. In contrast to the control group, those in the intervention group were explicitly made aware of being registered the following year regarding the length of their sick leave. The focus on sick leave itself might influence its length, which might be seen as a result of the awareness of being watched—this is often classified as a “Hawthorne effect”.12 However, if this awareness effect was pronounced in the present study, we would have expected a more immediate general response in the intervention group.
Chronic disorders and effect of intervention
The design did not address what actually happened at the workplaces. Intervention effects mediated through modified working conditions would, if unprepared, take some time.13 Firstly, due to the time to accept the idea, then a period for dialogue with the employer—and probably the sick-certifying general practitioner in a majority of cases—before effectuating any modified work. The possibility of returning to work with sickness benefits and active sick listing would also involve officers at the National Insurance Offices.14
Differences between sick-listed subjects with or without chronic disorders might contribute to the prompt effect in the subgroup dominated by chronic RDA disorders and the correspondingly late effect in other groups. The majority of sick-listed subjects who returned to work during the first 8–12 weeks in the other diagnostic groups are probably not those with chronic diseases. A higher level of preparedness on how to work with impairment, or that simply knowledge of modified work possibilities promotes the RTW in chronic disorders, might explain the effect in the RDA group. Effective interventions would be welcomed due to the overall lower RTW within one year, and longer mean sickness absence in the RDA group contributes considerably to the cost of sickness absence.15
Box 1: Summary of intervention package posted 14 days after the start of actual sick leave to subjects in the intervention group
Letter to the sick-listed persons containing a brief orientation of the following possible measures:
-
Opportunity to return to adjusted job on sickness benefits for 12 weeks after approval by the NIO
-
Cooperation between employee, employer, and NIO on modified work measures
-
Obligate formal approval by NIO to receive sickness benefits for more than 12 weeks
Questionnaire to the sick-listed persons:
-
Are you familiar with the use of modified work measures at your workplace?
-
Do you think that modified work measures could reduce your actual sick leave? (visual analogue scale (VAS) (“certainly no” to “certainly yes”))
-
Do you think that modified work measures could reduce future sick leave? (VAS)
-
Do you think you could return to work immediately if modified work measures were offered? (VAS)
-
Which measures do you think could reduce the duration of this or future sick leave(s)? (eight alternatives including none and others)
-
How long do you expect this sick leave episode to last? (seven categories)
-
Are you anticipating new episodes of sick leave within the next year?
-
Do you agree to your answers being copied to your local NIO?
During the actual sick leaves the National Insurance Register revealed no difference in the use of active sick leave between the intervention and control groups (20 and 21 episodes, respectively). This frequency was consistent with the general registered use of active sick listing in the county investigated. The deficient difference in the use of active sick listing does not rule out modified work as an important factor for reducing sick leave. Since the increased use of active sick leave in itself does not necessarily result in reduced sickness absence,16 active sick leave might not be a good indicator of other modified work measures.
The register data, unfortunately, do not give valid information on part-time sick leave, and the possible reduction of sickness absence due to change from full-time to part-time sick leave is therefore missed in the analysis. If there is any effect due to part-time sick leave, we would expect this to be in favour of the effect of intervention.
Mental disorders
The effect found in sick-listed persons with mental disorders was unexpected, as studies on interventions for work related stress have not demonstrated reduced absenteeism.17 Activating interventions are, however, found to reduce long-term absenteeism in persons certified sick due to adjustment disorders.18 Although our postal intervention does not match the intervention described by van der Klink et al,18 it might contain elements that promote graded return to work. Dialogue with the employer, and the return to work might be easier when sick-listed persons are informed about the possibilities for modified work. The reduced risk of long-lasting benefits after one year underlines the potential of even minor interventions in this diagnostic group.
An intervention study where sick-listed subjects, after seven weeks on sick leave, were provided with information and offered solution focused therapy, demonstrated no intervention effect, but the tendency was prolongation of sick leave in the intervention group.19 This indicates that questions on knowledge of measures available to reduce sick leave in general, and on the duration and measures needed to abbreviate the ongoing sick leave were more important than providing an information letter offering help to reduce sick leave. A recent Dutch randomised controlled trial, however, could not demonstrate significant sickness absence reduction by introducing health promoting interventions at the worksite.20
The results of this study might indicate that focusing on how to stay at work with health problems is more efficient than focusing on managing health problems to be fit for work, if lowered sickness absence is desirable. An alternative hypothesis is that successful interventions require very early initiation (perhaps within one month of sick leave)—before any side effects of being sick-listed have settled. The interaction of education on the risk of benefits might also indicate that self-influence on the job situation is important.10
Side effects of intervention
The longer sick leave in the intervention group with low back pain (compared to controls) was unexpected. Information on modified work measures might introduce an expectation of something to be done by others, and thereby maintain and even reinforce a passive attitude. This would be in contrast to focusing on, and encouraging being active as most important to a successful RTW.21,22 This would also be in line with studies revealing that excessive use of health care leads to longer sick leave,23,24 no effect of extensive treatments of low back pain patients with good prognoses,24 and of offering a solution focused follow up.19 We were unable to demonstrate a difference in vocational rehabilitation claims, but any expectation to gain these measures might explain that the prolongation effect was restricted to relatively young persons with less education. If the intervention interfered with use of part-time sick leave, the prolonged sick leaves in this group are not necessarily aligned to increased sickness absence.
The observed delay in RTW between 6 and 16 weeks in sick leaves among persons expecting an effect of modified work and/or requested copy to the NIO, might be at risk of bias as the response rate was only 32%. However, in respect of gender, age, diagnoses, and occupation they did not differ from the non-responders.7 Accordingly, the results probably support the necessity of an immediate response and decisions on options to counteract prolongation effects.
These inverse effects on prolonged sick leaves are probably unrecognised, but are very important to programmes aimed at reducing sick leave.
The different responses to minimal postal intervention in different diagnostic subgroups suggest that subsequent RCTs should be focused on disease specific rather than overall sick leave. The potential gain from such a minor intervention in some diagnostic groups should encourage measures leading to reflections on the length, and on the needs for modification of work measures, at very early phases of sick leave.
Main messages
-
Minimal postal intervention significantly reduced the risk for sickness related benefits after one year, and, although not statistically significant, reduced average length of sick leave with 8.3 days.
-
Minimal postal intervention can reduce sick leave in some diagnostic groups.
-
Minimal postal intervention might introduce passive expectations and have the side effect of prolonged sick leave in subgroups.
Policy implications
-
Introducing challenges as questions on length of sick leave and on possible modified work measures in the first few weeks of sick leave seems promising.
-
How, and to whom, these challenges are best introduced, needs further exploration.
Conclusion
This randomised, controlled study revealed that minimal postal intervention might reduce the length of sick leaves in some diagnostic groups, and the likelihood of receiving benefits due to health related problems after one year. However, the study also disclosed potential side effects that might prolong sick leave, probably through the introduction of unrealistic expectations and passivity, if possible measures at work are not readily clarified.
The results should encourage employees, insurance institutions, and authorities to initiate and explore challenges as questions on the length of sick leave, and on possible modified work measures, during the first few weeks of sick leave.
Acknowledgments
The authors would like to thank the Royal Ministry of Health and Social Affairs for funding support (project no 13345). This study could not have been performed without the support and contribution of the county and local National Insurance Offices in Troms.
REFERENCES
Footnotes
-
Published Online First 27 April 2006
-
Competing interests: none declared